Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
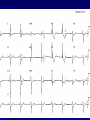
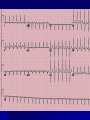
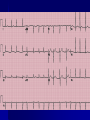
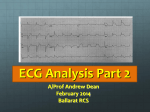
Arrhythmias Dr. Ahmad Hersi Med 441 6/1/2009 Conduction System Septal Branch Depolarization Sequence Catechism Identification Quality Rate Rhythm Axis Waves and intervals Specifics Frontal (limb lead) axis I II aVF Limb-lead Misplacement I II aVF Precordial Leads V1: Right 4th ICS parasternal V4: 5th ICS mid-clavicular line V2: Left 4th ICS parasternal V6: lateral to V4 mid-axillary line Rate Start if possible on a beat whose QRS (usually R wave) is on the border of a large square 300 100 60 40 150 75 50 Count Large squares (0.2 seconds each) This tracing example shows a rate of 100 bpm Rate determination for irregular rhythm * 8 times 10 = 80 bpm 30 For irregular rhythm (such as atrial fibrillation), the method shown on the last slide may be inaccurate. Use this alternate method. Start as before by finding a QRS that lands on the border of a large square (*). Then count 30 large squares (= 0.2 X 30 = 6 seconds). Add up all beats (QRSs) that land within the interval (not counting that first beat (*) and multiple by 10. This equals the number of beats per minute. Rhythm “Cherchez la P” To be convinced of sinus rhythm, you should see a P wave in front of every QRS, and the PR interval should not alter, and be of a plausible length. Lead II is usually the best lead for seeing P waves, and is often used for rhythm strips. QRS Axis Left I (-) aVF (-) II (-) I (+) aVF (-) II (-) Right I (-) aVF (+) II (+) Normal I (+) aVF (+) II (+) Quick Method for QRS Axis I aVF II The P Wave •Normally from sinus node •Upright in I, II, aVF, V4-V6 •Monophasic (except V1) •Normal ranges: o < 0.12 sec wide o < 2.5 mm tall The PR Interval Measure from beginning of P wave to onset of QRS. Usually measure in Lead II Measure the longest PR interval in the limb leads Normal range 0.120.20 seconds < 0.12 = Accelerated conduction > 0.2 = Heart block Right Atrial Enlargement Left Atrial Enlargement The QRS Complex The Q Wave The J - Point QRS Waveforms The ST Segment The T Wave T waves may be normally inverted in aVR (almost always), III (frequently), and V1 (sometimes). T waves are “tall” if their height is: – > 50% QRS height – > 5mm in limb lead – > 10 mm in precordial lead The QT Interval RR The U Wave Causes: – – – – – – Normal Bradycardia CAD Hypertension Hypokalemia Hypercalcemia Left Ventricular Hypertrophy * * * * Right Ventricular Hypertrophy LBBB RBBB Case 1 65 yr woman, presents to ER with Dizziness for 2hrs. In the past, a doctor told her that her heart rate is slow. Healthy otherwise, and is not on med’s. O/E : Bp=170/100 Another dizzy lady Had syncope What is the appropriate therapy? Management ABC V/S If serious symptoms or signs: - Atropine 1 mg - TCP - Dopamine - Epinephrine - Isoproterenol Management If clinically stable: - Prepare for TVP as a bridge device Case 2 25yr old woman 1 hr h/o palpitation No other cardiac symptoms Intermittent palpitation in the last 3 months , this episode is long BP= 120/70 What is your management? Management Narrow Complex tachycardia Serious signs and symptoms Immediate Cardioversion Stable clinically Vagal maneuvers Adenosine or Verapamil Consider BB, Diltiazem , or Digoxin Case 3 60 yrs C/O sudden onset dyspnea for last 1/2hr Past MI 1 yr ago, received thrombolytics. His ECHO at the time revealed impaired LV systolic function Med’s: ASA, Bisoprolol, Lisinopril, and Lasix On exam , BP=80/50 Bouts of palpitations WPW Short PR interval, less than 3 small squares (120 ms) Slurred upstroke to the QRS indicating pre-excitation (delta wave) Broad QRS Secondary ST and T wave changes • An accessory pathway, bundle of Kent, exists between atria and ventricles and causes early depolarisation of the ventricle. Case 4 75 yrs woman Presents to ER with fever and productive cough PMH= HTN BP=150/90 How would you manage ? Management If patient is hypoxemic O2 Control BP ( may chose a BB or CCB for rate control and BP control) Rate control the ventricular response if tachycardia . Consider Long term anticoagulation if no contraindications Normal ECG A 63 year old woman with 10 hours of chest pain and sweating. An 83 year old man with aortic stenosis. A 75 year old woman with loud first heart sound and mid-diastolic murmur. A 59 year old woman with chronic bronchitis. An 84 year old woman with hypertension A 73 year old woman with dizziness. A 70 year old man with exercise intolerance. A 90 year old lady with syncope. A 76 year old man with SOB A woman with Romano-Ward Syndrome A 45 year old women with palpitation and a history of CRF A 47 year old man with a long history of palpitations and blackouts. A 58 year old man on hemodialysis presents with weakness A 28 year old woman with prolonged vomiting