Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Baker Heart and Diabetes Institute wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
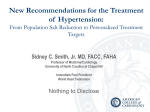
Cardiovascular disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Physiological basis of the care of the elderly client Cardiovascular System 1 Patient scenario RB, 73 year old Caucasian male Medical diagnosis hypertension Prescribed Norvasc, 5 mg qd and Accupril 10 mg BID Often forgets his evening dose Wants “one pill once-a-day” Complains of frequent headache on waking …pill makes him urinate too much …he has a cough that won’t go away …feels fine, maybe he doesn’t need it after all 2 Informal evaluation What additional information do you need? Subjective information Objective information Psychosocial information 3 The cardiovascular system Supplies oxygen to all parts of the body A failure in this system creates a cascade of failure in other systems Regardless of nursing focus, you will encounter cardiovascular concerns in the elderly client due to normal age related changes 4 Review of cardiac structure and function Circulation is established by electrical system of the heart Left side of heart produces enough force to overcome systemic resistance Effective circulation due in part to one way valves between the chambers of the heart Effective circulation is also dependent upon sequential contraction and relaxation of the heart 5 Potential challenges for the elderly client Electrical Coordination Force Valves 6 Preload and afterload Preload is a representation of the pressure stretching the left ventricle after passive filling and atrial contraction (diastole) by the blood returning to the heart Afterload is the amount of pressure produced by the left ventricle in order to contract (systole) 7 Regulation of cardiac function Preload Afterload 8 Contractility Left ventricle efficiency Determined by amount of blood pumped from the left ventricle at end of diastole Affected by Strength of contraction Amount of blood in the ventricle Competency of the valves Peripheral vascular resistance Ejection fraction = stroke volume / left ventricle end diastolic volume 9 The electrocardiogram Normal PR = .12-.20 (3-5 □s) Normal QRS = < .12 (3 □s) Normal sinus rhythm Each P wave followed by QRS Rate 60-90 with <10% variation P wave: atrial depolarization QRS complex: ventricular depolarization T wave: ventricular repolarization Little boxes = .04 sec; Big boxes = 5x.04 = .2 sec 10 Normal age related changes Heart valves become stiff Decreased renin, angiotensin and aldosterone production Arterial stiffening and loss of elasticity Veins thicken and valvular reflux occurs Decreased baroreceptor sensitivity Decrease in number of normal pacemaker cells in sinus node Myocardial hypertrophy 11 Increased size of myocardial cells Thickening of left ventricular wall Resulting systemic effects Increased resistance of peripheral vessels Decreased coronary blood flow Reduced cardiac output Less efficient cardiac oxygen usage Slower response to cardiac challenge if not in good physical condition 12 To prevent debilitation from cardiovascular changes through lifestyle modification… Remain physically active—30 minutes aerobic activity per day most days of the week Avoid obesity—maintain normal BMI between 22-25 Avoid smoking Control blood pressure Control cholesterol levels Restrict sodium intake to 2.4 g/day Limit alcohol to ≤2/day for men, ≤1/day for women 13 Atypical presentation of cardiac disease Presenting complaint may be heartburn, nausea, fatigue Mental status changes Dizziness and falls Agitation Sudden change in cognitive abilities New onset atrial fibrillation Particularly in women: 14 Fatigue Sleep disturbances Epigastric pain Heart disease in elderly women Symptoms may be unrecognized: Sleep disturbances Intermittent chest tightness, squeezing, pressure Back, neck, stomach, jaw discomfort Shortness of breath, nausea, lightheadedness Break out in cold sweat 15 Hypertension A major risk factor for developing other cardiovascular conditions because: 16 It does not always produce its own symptoms Many are unaware they have hypertension It is easily ignored Classifications of blood pressure Optimal: <120/<80 Screen every 2 years Prehypertension: 120-139/80-89 Assess annually Stage 1 HTN: 140-159/90-99 Assess more frequently Stage 2 HTN: ≥160 OR ≥100 Assess more frequently 17 JNC 8 (2014) Guidelines After age 50, SBP >140 is a more important risk factor than DBP A 90% risk of developing HTN exists even in those age 55 who are normotensive 120-139/80-89 is prehypertensive; patients should begin lifestyle modifications Most patients with HTN need 2+ medications Thiazide diuretics should be used to treat uncomplicated HTN Effective therapy requires patient motivation Empathy builds trust and promotes motivation 18 JNC 8 Hypertension Management Lifestyle interventions apply throughout all treatment recommendations Blood pressure goals and medication treatment based on 19 Age Diabetes Chronic kidney disease JNC 8 HTN Management Algorithm: Age ≥60 years No diabetes No CKD 20 Goal SBP • <150 mm Hg Goal DBP • <90 mm Hg JNC 8 HTN Management Algorithm: Age <60 years No diabetes No CKD Goal SBP •< 140 mm Hg Goal DBP •< 90 mm Hg 21 JNC 8 HTN Management Algorithm: All ages With diabetes No CKD Goal SBP •< 140 mm Hg Goal DBP •< 90 mm Hg 22 JNC 8 HTN Management Algorithm: All ages with CKD Goal SBP •< 140 mm Hg Goal DBP •< 90 mm Hg 23 JNC 8 HTN Treatment Guidelines Black No CKD • Thiazide-type diuretic, or, • CCB, or, • Combination 24 Non-Black No CKD • Thiazide-type diuretic, or, • ACEI, or, • ARB, or, • CCB, or, • Combination All Races CKD • ACEI, or, • ARB, or, • Combination with other class “Instant” teaching points regarding HTN It is not the same as anxiety Once you are diagnosed, you are on medication for life* It is defined as systolic blood pressure > 140 mmHg Most cases of HTN are classified as primary HTN—the underlying cause is not known *some exceptions! 25 Results of untreated hypertension Atherosclerosis of the aorta and large vessels accelerates Left ventricular hypertrophy develops Proteinuria due to increased renal arteriole pressure Vascular changes in the retina (A-V “nicking”) Increased stroke risk 26 Nursing management—patients with HTN Evaluate BP bilaterally and in lying, sitting and standing positions Blood pressure varies with time of day and with activity Respond to “white coat hypertension” Home blood pressure monitoring must be confirmed Assess for target organ damage with each encounter 27 Nursing management—patients with HTN High blood pressure screening Promote healthy lifestyle Low fat diet Low sodium diets Weight control Exercise Smoking cessation Controlled alcohol consumption Monitor effects of medication 28 Medication management of hypertension Initial treatment usually involves diuretics Second medication selected pertaining to patient’s health status β-blockers can cause bradycardia, fatigue, exercise intolerance Postural hypotension can occur with adrenergic inhibitors and α-blockers Dry cough, hyperkalemia can occur with ACE inhibitors and angiotensin receptor blockers Calcium channel blockers (esp. Benzothiazepines) may cause decreased cardiac output and slow conduction 29 Hypotension Frequently associated with medication side effects Decreased responsiveness of sympathetic nervous system with age affects autoregulation of cardiac output Lying/sitting (postural) blood pressure: 30 Supine for at least 5 minutes, then check blood pressure Check again after 1 and 3 minutes of sitting or standing Hyperlipidemia Elevated cholesterol is a risk factor for cardiovascular disorders Remember…Keep HDLs high, keep LDLs low! LDL < 100 mg/dl* HDL > 60 mg/dl* LDL *Optimal per JNC7! 31 HDL Benefits of the “statins” Lower LDL cholesterol Anti-inflammatory Antithrombotic Protect plaque stability Generally well tolerated 32 Atorvastatin (Lipitor) Fluvastatin (Lescol XL) Lovastatin (Mevacor) Pravastatin (Pravachol) Rosuvastatin (Crestor) Simvastatin (Zocor) Metabolic syndrome (“syndrome X”) • > 135/80 • Men > 40” • Women > 35” • >150 mg/dl 33 Waist Circ. BP TG BG • >100mg/dl (fasting) Characteristics of metabolic syndrome Abdominal fat cells secrete hormones promoting heart disease and diabetes Patients have below-normal HDL Decreased insulin sensitivity (level of insulin required to process glucose) 34 Treatment plan for metabolic syndrome Cholesterol lowering drugs Antihypertensives Diet high in omega-3 fatty acids Avoid processed foods Exercise 30-45 minutes moderate intensity 35 Ischemic heart disease in the elderly Chest pain is not always present Fatigue Weakness Shortness of breath GI disturbances 36 Chest pain Caused by a mismatch between what the body is able to deliver and what the body requires Supply ischemia—due to decreased blood flow to the heart Demand ischemia—due to increased demand for oxygen In stable angina, chest pain is relieved with rest If not relieved by rest, can progress to myocardial infarction 37 Other causes of chest pain Pericarditis Heartburn, ulcers Chondritis Pulmonary embolus, pneumonia Herpes zoster 38 Treatment of angina Nitroglycerine—vasodilator NTG is treatment of choice Comes in tablets, sprays, patches, ointment, IV, sublingual Tablets for acute attacks Transdermal, capsules, ointments do not work rapidly enough during acute attacks Repeat tablet every 5 minutes for acute attack If no resolution after 3 tablets, patient must be transported to hospital 39 Myocardial infarction findings Occurs in stages, treatment directed to the stage EKG changes—ST elevation Q wave represents infarcted tissue CK-MB elevation 4 to 6 hours after infarction Troponin elevation 6 to 8 hours after infarction Hemodynamic monitoring necessary if heart failure suspected 40 Complications of MI Arrhythmia (dysrhythmia) Conduction blockages Heart failure Pulmonary edema Ventricular aneurysm Pericarditis 41 Anticoagulation treatment of MI Useful within first few hours of event Chew an aspirin while waiting for ambulance! Not all patients are candidates for thrombolytic therapy 42 Aortic stenosis Most common valvular disorder in the elderly Usually due to calcification Risk factors: Hyperlipidemia Diabetes Hypertension Left ventricular hypertrophy Heart failure 43 Heart failure Heart no longer able to provide sufficient cardiac output Men develop after an MI; women after long-standing HTN Compensatory events Increased heart rate Renin → angiotensin I → angiotensin II → increased BP and sodium and water retention Risk factors: 44 Coronary artery disease Hypertension Right sided versus left sided failure 45 Neck vein distention 46 Dysrhythmias (not “arrhythmias!”) Atrial fibrillation most common dysrhythmia Incidence increases with age Not life-threatening by itself; can increase mortality No P-wave Disorganized electrical impulses overwhelm SA node Results in an irregular heart rhythm Treated with anticoagulation (Heparin, Warfarin [Coumadin]) 47 Venous disease Valvular incompetence Pressure transferred to capillaries of lower extremities Cells break down Debris collects Can cause nonhealing ulcers Often misinterpreted as “spider bite” Treatment is compression 48 Formal evaluation What is your nursing diagnosis for RB? What is your desired outcome? What are appropriate interventions pertinent to your desired outcome? 49