Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Epigenetics of neurodegenerative diseases wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Gene expression programming wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Microevolution wikipedia , lookup
Public health genomics wikipedia , lookup
Dominance (genetics) wikipedia , lookup
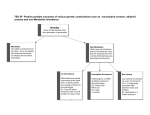
OSAHS Phenotypes : More Understanding BY DR: MOHMMAD EL DESOUKY ABOU SHEHATA Prof of: PULMONOLOGY MASOURA UNIVERSITY Obstructive Sleep Apnea /Hypopnea Syndrome (OSAHS) The syndrome is characterised by obstruction of the upper airway during sleep, resulting in repetitive breathing pauses accompanied by oxygen desaturation and arousal from sleep. This may result in diurnal sleepiness and may lead to cognitive impairment and cardiovascular morbidity Riha R L et al Eur Respir J 2009; 33: 646–655 OSAHS AASM Definition Sleep Apnea • Obstructive apnea is the cessation of airflow for at least 10 seconds with persistent respiratory effort. . • Central apnea is the cessation of airflow for at least 10 seconds with no respiratory effort • Mixed apnea is an apnea that begins as a central apnea and ends as an obstructive apnea OSAHS AASM Definition Sleep Hypopnea • The recommended definition of a hypopnea is a 30% or greater decrease in flow lasting at least 10 seconds and associated with a 4% or greater oxyhemoglobin desaturation. • An alternative definition is a 50% or greater reduction in flow lasting at least 10 seconds and associated with either a 3% or greater oxyhemoglobin desaturation or an arousal. Clinical Manifestation of OSAHS Nocturnal symptoms • Snoring, • Witnessed apneas • Gasping and choking sensations that arouse the patient from sleep • Restless sleep, with patients often experiencing frequent arousals a Daytime symptoms • Not feeling refreshed upon awakening • Morning headache, dry or sore throat • EDS that usually begins during quiet activities (e g, reading, watching television) • Fatigue Prevalence Of ( OSAHS) • • OSAHS is the third most common respiratory condition after asthma and chronic obstructive airway disease 2-4% of the middle-aged population is affected by OSAHS • Up to 20% of the population is thought to have SDB at any one time Bixler EO, et al. Am J Respir Crit Care Med 1998 Young T et al .N Engl J Med 1993; 328: 1230–1235 SEQULUE OF Untreated OSAHS • OSAHS is an independent risk factor for diurnal hypertension • epidemiologically, has been implicated as a risk factor for stroke and other cardiovascular events • OSAHS may contribute to the expression of metabolic syndrome, increased insulin resistance and a higher inflammatory state. Faccenda JF,et al (2001) Am J Respir Crit Care Med 2001; 163: 344–348 Shahar E ,et al (2001) Am J Respir Crit Care Med 2001; 163: 19–25. CLINICO-PHYSIOLOGICAL PHENOTYPES OF OSAHS • A phenotype is any detectable characteristic of an organism determined by an interaction between its genotype and environment • Phenotypic plasticity, is the ability of an organism with a given genotype to change its phenotype in response to changes in the environment, may be applicable to OSAHS. • Thus, a particular genotype may express itself as a different phenotype at different times and in response to different environmental circumstances . Ernande B, Dieckmann U. J Evol Biol 2004; 17: Riha R L et al Eur Respir J 2009; 33: 646–655 Risk Factors Implicated In OSAHS Phenotype Expression • • • • • Obesity and Ageing Gender : Male > Female ; postmenopausal female craniofacial abnormalities, race and certain congenital conditions, such as Marfan’s syndrome, Enviromental risk factors e g Alcohol ; sedative use, sleep deprivation,tobacco use and sleeping in the supine posture • Reduced nasal patency, due to a variety of causes, can contribute to OSAHS Strohl KP,et al, Am J Respir Crit Care Med 1996; 154: 279–289. The Phenotypic Complexity of OSAHS • Upper airway obstruction during sleep is the key pathophysiological feature in OSAHS. • dysfunction of upper airway muscles alone is unlikely to be the sole cause of OSAHS • A number of interrelated pathologies and risk factors interact to produce the OSAHS phenotype • The strongest risk factor is obesity and ageing Riha R L et al Eur Respir J 2009; 33: 646–655 Impact of Normal Ageing in OSAHS Phenotypic Expression • A changes in parapharyngeal fat pad deposition • serotonergic disregulation of brainstem respiratory control (wear and tear ) • age-related changes in bony structures such as edentulism • Variations in neuromuscular control of the upper airway may gain greater importance in the elderly • Increased prevalence of cardiac and cerebrovascular disease • Older subjects may report less daytime sleepiness for a given level of OSAHS • OSAHS in the elderly is less likely to be equivalent to the same disorders that develop in middle or young age. OSAS From Genotype To Phenotype • Hereditary factors are thought to invoke 40% of the variance in the occurrence of OSAHS in the general population; • the rest is attributable to environmental factors • It is likely that genetic factors associated with craniofacial structure, body fat distribution and neural control of the upper airway muscles interact to produce the OSAS phenotype Redline S, Tishler PV: The genetics of sleep apnea. Sleep Med Rev 2000; 4: 583–602. M Casale et al . Curr Genomics .2009 ; April 10(2): 119-126 Intermediate Phenotypes of OSAHS Due to the considerable clinical heterogeneity of the OSAHS phenotype, the current paradigm of OSAHS was considered as the product of intermediate phenotypes which interact to produce the overall phenotype OSAHS Intermediate Phenotypes • • • • Craniofacial phenotype Obesity phenotype susceptibility to sleepiness phenotype ventilatory and upper airway control. Intermediate Craniofacial Phenotype Morphological features • • • • • cranial base dimensions being more obtuse, inferior displacement of the hyoid bone, increase in lower facial height, a retroposed maxilla and a short mandible macroglossia, adenotonsillar hypertrophy, Intermediate Craniofacial Phenotype Factors Linked To Expression Of Craniofacial Phenotype • Environmental mechanisms play a strong role in determining cranioskeletal growth. These include bad habits such as thumbsucking and abnormal tongue posturing, nasopharyngeal disease, disturbed respiratory function (e.g. mouth breathing), tumours, loss of teeth, malnutrition and endocrinopathy . • Gene involved in the embryogenesis, growth, development and expression of the craniofacial complex are subject to very complex gene–gene and gene–environmental effects and their pathways are yet to be fully elucidated genes controlling final adult height and stature may affect craniofacial growth. These include the vitamin D receptor, beta-2adrenergic receptor, growth hormone, insulin-like growth factor (IGF-1), insulin-like growth factor receptor and growth hormone receptor (GHR). Specifically, IGF-1 has been shown to be an important and independent regulator of maxillofacial and Mandibular growth postnatally Latral cephalometric radiograph showing the Cervico-craniofacial skeletal reference points and lines used for linear and angular measurements.( A: subspinale =the most posterior midline point in the concavity between the anterior nasal spine and the lowest point on the alveolar bone overlying the maxillary incisors ,B: Supramentale = the most posterior medline point on the anterior concavity of the mandibular symphysis a midsagittal MRI image show the nasopharynx and retroplatale narrowing midsagittal MRI image show surface area of the tongue midsagittal MRI image show surface area of the soft palate and retroplatal obstruction Airway of normal subject ( increase lateral dimension than AP) Axial MRI of the velopharynx show the parapharyngeal muscular thickness Intermediate Obesity Phenotype Link between obesity OSAHS • Morbid obesity defined as a body mass index (BMI) of > 30 is present in 60–90% of patients with OSAHS • Central obesity, characterised by a high waist:hip ratio or increased neck circumference, is probably better correlated with OSAHS. • not all obese subjects will snore or have SDB . Pathogenesis of OSAHS • In obesity, fat deposition results in a reduction in nasopharyngeal calibre • Adipokines, such as leptin, may affect the regulation of the respiratory centre Axial MRI show parapharyngeal pad of fat susceptibility to sleepiness Link between sleepiness & OSAHS • Sleepiness, as a consequence of SDB, is required to define OSAHS but does not necessarily correlate with it. • There appears to be a differential susceptibility to somnolence among individuals. Pathogenesis • Sleep is regulated by neuronal and humoral mechanisms that are interdependent • Interleukin (IL)-1; TNF-a ; appear central to the sleep activation pathways, and other sleep-inducing cytokines include IL-10, IL-6, interferon, IL-2, IL-4, • Many of these cytokines are pleiotropic and also implicated in initiating or propagating the sequelae of OSAHS, particularly inflammation ventilatory and upper airway control. Ventilatory control • There is a high degree of heritability of peripheral chemoreceptor responses to hypoxia and hyperoxia in monozygotic twins • Although several studies have shown abnormalities of respiratory control It is debatable whether respiratory control problems are implicated in the pathogenesis of OSAHS OSAHS Phenotype --- Home Message • At present OSAHS has no distinct phenotype definition • OSAHS appears to be a complex polygenic disease. • Intermediate phenotypes interact in different dimensions to produce a single phenotype at a given point in time. • The degree of environmental influence is difficult to gauge but is likely to be considerable. • Progress in determining the genotype of OSAHS is affected by the lack of a consistent definition of phenotype.