Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
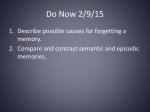
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. AUTHOR QUERY FORM Book: Pediatric Neurology Part I 111 Chapter: 16 Please e-mail your responses and any corrections to: E-mail: [email protected] Dear Author, Any queries or remarks that have arisen during the processing of your manuscript are listed below and are highlighted by flags in the proof. (AU indicates author queries; ED indicates editor queries; and TS/TY indicates typesetter queries.) Please check your proof carefully and answer all AU queries. Mark all corrections and query answers at the appropriate place in the proof (e.g., by using on-screen annotation in the PDF file http://www.elsevier.com/framework_authors/ tutorials/ePDF_voice_skin.swf) or compile them in a separate list, and tick off below to indicate that you have answered the query. Please return your input as instructed by the project manager. Uncited references: References that occur in the reference list but are not cited in the text. Please position each reference in the text or delete it from the reference list. Segovia et al., 2008; Strijbis et al., 2006 Missing references: References listed below were noted in the text but are missing from the reference list. Please make the reference list complete or remove the references from the text. Location in Chapter Query / remark AU:1, page 9 This isn't mentioned in your chapter! AU:2, page 8 Ref not cited in text; OK to delete? TS:1, page 7 The following references are not cited in the text. “Segovia et al., 2008; Strijbis et al., 2006” This Journal title “PNAS” is not available in the Index Medicus 2007. Please check. TS:2, page 7 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. Handbook of Clinical Neurology, Vol. 111 (3rd series) Pediatric Neurology Part I O. Dulac, M. Lassonde and H.B. Sarnat, Editors © 2013 Elsevier B.V. All rights reserved c0080 Chapter 16 Pathophysiology of cerebral palsy 1 STEPHANE MARRET 1, 2*, CATHERINE VANHULLE 1, AND ANNIE LAQUERRIERE 2, 3 Department of Neonatal Medicine and Centre of Child Functional Education, Rouen University Hospital, Rouen, France 2 Microvascular endothelium and neonatal brain damage Research Team, Rouen Institute for Medical Research and Innovation, School of Medicine, Rouen University, France 3 Pathology Laboratory, Rouen University Hospital, Rouen, France p0005 s0005 p0010 p0015 Cerebral palsy (CP) is a range of nonprogressive syndromes of posture and motor impairment, causing activity limitation, and often accompanied by other neurodevelopmental disorders such as specific cognitive or visual deficits (Bax et al., 2006). Nearly half of these disabilities are diagnosed in preterm born children and the other one in full-term born children (Expertise INSERM, 2004). CP is usually classified into topography-based subtypes (quadriplegia, diplegia, hemiplegia, or extrapyramidal disorders) which often result from various insults to different areas within the developing nervous system, occurring in utero, during delivery, or after birth during the first 2 years of life. The vulnerability of different brain structures and types of disability associated with CP are strongly influenced by the gestational age at which brain development is altered. Better insights into the mechanisms of sub-type CP occurrence are urgently needed to lead to brain protection strategies and CP prevention as changes in obstetrical practice and the development of neonatal care over the last 25 years have had little effects on the rate of CP (Nelson, 2008). CAUSAL FACTORS Human population-based epidemiological studies and neuroimaging, in particular resonance magnetic nuclear imaging (MRI), are the best ways of identifying physiopathogenesis of the different subtypes of CP. In the first part of pregnancy until 24 weeks’ gestation, cortical neurogenesis takes place and is characterized by proliferation, migration, and organization of neuronal precursor cells, then neurons. It can be altered by genetic deficits or acquired (viral or toxic) impairments resulting in rare malformations such as lissencephaly or agyria-pachygria, nodular heterotopias, polymicrogyria, schizencephaly, and cortical dysplasia. In the second part of pregnancy, growth and differentiation events (axonal and dendrite growth, synapse formation, and myelination) as well as stabilization processes (neural cell apoptosis, neurite regression, redundant synapse elimination) and specialization of circuitry are predominant and persist after birth and are maximal during the first 2 years of life. Environmental factors such as hypoxiaischemia are involved in the occurrence of CP at this step of brain development. These factors could be severe enough to determine destructive injuries visible using standard imaging (i.e., ultrasonographic study or MRI), predominantly in the white matter of preterm infants and in the gray matter and the brainstem nuclei of full-term newborns. Moreover, they occur in an immature brain and could alter the remarkable series of developmental events. CP is therefore the result of destructive and developmental mechanisms. Interruption of oxygen supply to the fetus and brain asphyxia were classically considered to be the main causal factors explaining later CP. But clinically defined birth injury or birth asphyxia account for a minority of cases of CP. Several nonischemic factors have now been recognized in human epidemiological studies and in animal experimental studies (Fig. 16.1). CP is infrequently due to a brain malformation secondary to a unique genetic deficit or an acquired perinatal damage due to a unique acute asphyxic event (Fig. 16.2). In most cases of CP, causal factors do not act in isolation, but in synergy to create a disturbance. A set of predisposing *Correspondence to: Stéphane Marret, Department of Neonatal Medicine and Centre of Child Functional Education. Rouen University Hospital, 1 Rue de Germont, F-7600 Rouen, France. Tel: þ.33.2.32.88.80.97, Fax: þ .33.2.32.88.86.33, E-mail: [email protected] Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:39 Page Number: 1 Title Name: HCN p0020 p0025 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. 2 M. STEPHANE ET AL. Causal factors of cerebral palsy between 20 weeks of gestation and neonatal period Predisposing factors Acute or subacute perinatal factors • Preterm birth • IUGR • Vascular disease of pregnancy • Hormon or Growth factor deficiency • Toxic – In utero stress • Hypoxic-IschemiaReperfusion • Infection-Inflammation Post-natal factors • Chronical hypoxia • Drugs • Nutrition • Mother/baby separation • Socio-economic level ● Window for prevention Developmental disorders Destructive lesions Window for repair Motor and cognitive disabilities f0005 Fig. 16.1. Causal factors of cerebral palsy between 20 weeks of gestation and neonatal period. antenatal factors, perinatal acute or subacute events, and postnatal aggravating factors act together on the developing brain of the fetus and the newborn to alter brain maturation and lead to CP. s0010 Predisposing factors p0030 Predisposing antenatal factors include various genetic, epigenetic, and environmental factors: u0005 ● u0010 ● u0015 ● Congenital abnormalities. There is a consistent observation that children with CP have more congenital abnormalities (cleft lip and palate, hypospadias, gut atresias. . .) than other children (Pharoah, 2007). Genetic factors. They could influence the risk of CP along the cascade of events leading to CP. An increased risk of CP has been observed in some families in a national Swedish database (Hemminki et al., 2007). Genetic factors are involved in some thrombophilias underlying perinatal strokes and secondary CP (Kirton and de Veber, 2009). But it has been suggested that most thrombophilias need another event such as viral or bacterial infection to cause vascular thrombosis (Gibson et al., 2003). Genetic polymorphisms in gene encoding proteins of inflammation or coagulation or vascular endothelium of the placenta are associated with CP in some children (Nelson, 2008). Infections. Among the congenital TORCH (Toxoplasma (Fig. 16.2A), Other (syphilis, varicellazoster, parvovirus B19, Rubella, Cytomegalovirus (CMV), Herpes simplex virus) infections, CMV is Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:39 Page Number: 2 Title Name: HCN ● ● ● ● ● the most frequent virus implicated in brain damage during pregnancy. Congenital enterovirus, arenavirus, and lymphocytic choriomeningitis virus infections are exceptional. Moreover it has been shown that fetal exposure to a variety of viruses may be associated with hypertensive pregnancy disorders and that perinatal exposure to neurotropic viruses is associated with preterm delivery and cerebral palsy (Gibson et al., 2003). Toxic factors. Alcohol is one of the most frequent toxic factors which could determine brain maldevelopment during the whole pregnancy and later CP in case of severe malformation such as lissencephaly (Guerri, 2002). In animal studies, it was observed that it is an additional factor which aggravates damage induced by an acute ischemic or excitotoxic event (Adde-Michel et al., 2005). The role of other maternal types of drug abuse, such as cocaine, seems to be less important than previously thought (Bauer et al., 2005). An increasing number of drugs such as valproic acid taken by the mother during gestation are shown to interfere with brain energy, transport of monocarboxylic acids, and carbohydrate and lipid metabolisms. This alteration may not be transitory but can permanently impair fetal neuronal function and contributes to postnatal neurological disease including CP (Bolanos and Medina, 1997). Multiple gestation. The higher risk of CP observed in this population is due to two main factors: the high rate of preterm birth and co-twin death whether they were same-sex or not. In monozygotic twins, where one twin dies, vascular collapse in the survivor or an embolism originating from the circulation of the dead twin can occur resulting in encephalomalacia or porencephaly and secondary CP (Scher et al., 2002). Vascular disease of pregnancy. Preclampsia and intrauterine growth restriction have been demonstrated to be associated in several epidemiological studies with neonatal encephalopathy in full-term newborns and subsequent CP (Badawi et al., 1998). Preterm birth. Separation of the fetus from his natural environment before the end of gestation could alter the normal development of the brain (Livinec et al., 2005). It was demonstrated in animal models that some maternal or placental factors such as vasointestinal peptide act early on the fetal neural axis to stimulate their development (Gressens et al., 1993). Post-term birth. Placental involution which begins in cases of postmaturity makes the brain sensitive to damage (Badawi et al., 1998). Maternal factors. Maternal thyroid disease has been related to neonatal encephalopathy and CP in u0020 u0025 u0030 u0035 u0040 u0045 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. PATHOPHYSIOLOGY OF CEREBRAL PALSY f0010 u0050 3 Fig. 16.2. Macroscopic views of fetal or neonatal cerebral lesions. (A) Coronal section of a fetus with first trimester pregnancy toxoplasma infection. (B) Unilateral schizencephaly in a fetus whose mother had had an interruption of pregnancy. (C) Periventricular leukomalacia with multicavitary lesions in an infant born at 30 weeks’ gestation. (D) Putamen necrosis in an at term newborn with perinatal asphyxia. ● full term infants as well as other factors such as lengthy maternal menstrual interval or diabetes (Nelson, 2008). Sex. A recent emerging concept is that sex may influence the pathogenesis of developmental brain injuries. CP is more prevalent in males than in females. Males with preterm birth had significantly reduced white matter compared with term males while white matter was equivalent in female groups. In contrast preterm females with intraventricular hemorrhage (IVH) showed a reduction in gray matter compared with controls, but males with IVH did not (Johnston and Hagberg, 2007). Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:39 Page Number: 3 Title Name: HCN Acute perinatal events s0015 Birth asphyxia can cause spastic diplegia in very preterm infants and quadriparetic CP with mental retardation from 34 weeks’ gestation at birth. The criteria promulgated by the American College of Obstetricians and Gynecologists and American Academy of Pediatrics to attribute intrapartum hypoxia as a cause of neonatal encephalopathy and later CP in full-term newborns include: (1) an umbilical arterial pH of 7; (2) a moderate or severe neonatal encephalopathy; (3) a later quadriparetic or dyskinetic CP; and (4) an absence of other causes. However CP is seldom preceded by an intrapartum event. The proportion of CP associated with an intrapartum event p0085 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. 4 p0090 p0095 M. STEPHANE ET AL. was found to be 14.5% in a review of the literature in the English language (Graham et al., 2008). Inflammation, maternal fever caused by chorioamnionitis, or urinary tract infection are now well-recognized subacute or acute factors frequently associated with neonatal encephalopathy at birth and with CP risk in several studies regarding preterm, near-term, or full-term infants (Nelson and Grether, 1997; Wu et al., 2003; Bax et al., 2006). In a study of full-term newborns who had CP and for whom genetic and viral pathogenic causes were excluded, 38% of spastic quadriplegia was associated with chorioamnionitis (Wu et al., 2003). Many studies have linked the close associations between perinatal infections and hypoxicischemic insults. Infection/inflammation can potentiate hypoxicischemic insults to the brain and convert a subthreshold insult to a seriously damaging event. But some animal studies did not yield support for the hypothesis that brain damage is due to reduced blood flow in infection (Duncan et al., 2002; Girard et al., 2009). s0020 Postnatal additional factors p0100 These factors are mainly observed in preterm infants in whom the brain after birth is subjected to early influences that are different from those of the materno-placental unit. Several of these factors could dramatically alter brain development, such as stress and separation of mother/baby, nutrition and extrauterine growth retardation, nosocomial infections, enterocolitis, or drugs. The Newborn Individualized Developmental Care and Assessment Program (NIDCAP), which notably takes into account parental and child stress, has beneficial effects in the short term, as it favors an early discharge from hospital (Als et al., 2003). Postnatal infections, enterocolitis, as well as early postnatal use of glucocorticoids in preterm infants have been demonstrated to be independently associated with white matter injury and later CP (Glass et al., 2008; Shah et al., 2008; Halliday et al., 2009). s0025 Socioeconomic status p0105 There is conflicting evidence in the literature regarding socioeconomic differences in families giving birth to children that develop CP. But most recent studies suggest a link between CP and socioeconomic indicators. In a Swedish study, there was a linear association between the incidence of CP (after exclusion of head injuries, chromosomal aberrations, and brain malformations) and socioeconomic status (SES) of the household of the mother (low SES versus high SES adjusted odds ratio 1.36 (1.051.71)) (Hjern and Thorngren-Jerneck, 2008). Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:45 Page Number: 4 Title Name: HCN Finally it is also observed that a significant number of children with CP experienced none of the causal factors outlined above. NEUROPATHOLOGICAL AND HISTOLOGICAL ASPECTS OF PERINATALLYACQUIRED CEREBRAL PALSY IN PRETERM AND FULL TERM NEWBORNS p0110 s0030 Neuropathological and functional aspects s0035 Understanding the development of the immature brain has led to the theory of selective vulnerability, resulting in two main distinctive associations: white matter injury in premature infants and gray matter lesions, in particular of the basal ganglia in full-term neonates presenting with perinatal asphyxia. In full-term infants, hemiplegia is observed in cases of antenatal porencephaly/unilateral schizencephaly (Fig. 16.2B), and perinatal arterial ischemic or hemorrhagic stroke. Fetuses and neonates often have larger infarcts than adults and develop cystic lesions rather than dense gliotic scars. One reason is that the full-term neonate has only one-sixth as many resident astrocytes in the white matter compared with the adult. Thus astrocytic invasion of the infarcted tissue cannot occur, resulting in cavitary lesion. Quadriplegia or dyskinesia are most often the consequence of diffuse basal ganglia and thalamic damage (Fig. 16.2D), cortico-subcortical injury, and/or watershed pattern damage. A disorder of cortical development is rarely observed: abnormal proliferation and neuronal generation as observed in microcephaly, abnormal neuronal migration as noted in type I lissencephaly spectrum or absence of extracellular matrix integrity as in type II lissencephaly, or “cobblestone syndrome” (Francis et al., 2006). In preterm infants, spastic diplegia is the most frequent motor sequela and is significantly associated with diffuse white matter injury with intraparenchymal hemorrhage and/or periventricular cavitary lesions (Fig. 16.2C). These damages are favored by the vascular anatomical developmental step observed in these infants who have larger microvascular territories with poorly developed collateral circulation compared with the adult brain, as well as immaturity of cerebral blood flow autoregulation (partly due to neurogenic immaturity and partly due to the fact that the formation of smooth muscular walls of intracerebral arterioles develop late during gestation, so that even if the neural mechanism is in place, the end-organ cannot respond well in prematurity). Disruption of the corticospinal tracts is responsible for the developmental motor disorders since it is the final pathway for mediating the influence on motoneurons of the brainstem and spinal cord of nearly all cerebellar p0115 p0120 p0125 p0130 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. PATHOPHYSIOLOGY OF CEREBRAL PALSY p0135 efferents and those of the basal ganglia (all via intermediate relay in the thalamus). There are no direct cerebellospinal, striatospinal, or pallidospinal tracts in humans, explaining the dyskinesias and cerebellar deficits experienced by some children, superimposed upon their spastic or hypotonic diplegia. The cerebellum and basal ganglia are also influential in determining final passive muscle tone in cerebral palsy. But in children with CP, brain lesions are highly variable. In a cross-sectional, population-based study conducted in eight European study centers, 11.7% of 351 children with CP had normal MRI findings, the others having white matter injury (42.5%), basal ganglia lesions (12.8%), cortico-subcortical lesions (9.4%), focal infarcts (7.4%), miscellaneous lesions (7.1%), and malformations (9.1%) (Bax et al., 2006). More than half of these children with CP were delivered at full term, while 18.3% were born between 32 and 36 weeks of gestation, 16% between 28 and 31 weeks, and 10.9% below 28 weeks. Almost one in five children were small for gestational age (< 10%). In the population-based EPIPAGE study of all 2901 live births between 22 and 32 completed weeks of gestation observed in nine regions of France in 1997, 29.4% (46) of the 156 children who had CP at 5 years of age had no ultrasonographic abnormalities in the neonatal period (Beiano et al., 2010). The ultrasonographic abnormalities in the other 110 children with CP were as follows: 49% (77) with white matter injury (periventricular cyst or persistent hyperechogenicities or intraparenchymal hemorrhage), 8.9% (14) with intraventricular hemorrhage (IVH) with dilatation, 8.3% (13) with IVH without dilatation, and 3.8% (6) with only a subependymal hemorrhage. s0040 MICROSCOPIC ALTERATIONS s0045 Cerebral lesions in the preterm infant p0140 A window of enhanced vulnerability of white matter between 24 and 34 weeks of gestation is related to the active growth of cerebral pathways. It is a phase of high proliferation, migration, and maturation of glial cells (astrocytes and oligodendrocyte precursors) and of high expression of microglial cells (Billiards et al., 2006). During this period, the cortical subplate contains two types of neurons: GABAergic neurons, which originate from progenitors generated in the ventricular zone and the subventricular zone of the dorsal forebrain or of the ganglionic eminences of the ventral telencephalon, and are migrating respectively radially and tangentially toward the upper cortical layers, and subplate neurons, which serve as sites of synaptic contacts for “waiting” thalamo-cortical and commissural/association cortico-cortical afferents, before entering the cortex to form the thalamo-cortical and cortico-cortical tracts (Petanjek et al., 2009; Volpe, 2009). An endogenous Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:45 Page Number: 5 Title Name: HCN 5 transient subplate circuitry coexists with thalamocortical permanent circuitry. Animal and human data suggest that injury specifically to preoligodendrocytes accounts for subsequent myelination defects after periventricular white matter injury (McQuillen and Ferriero, 2004; Volpe, 2009). Axonal injury and degeneration have been observed in the focal necrotic component and the diffuse component of human white matter injury. Moreover neuronal death and gliosis are common in the subplate, the basal ganglia, and the cerebellum. Neuronal loss of GABAergic neurons in the subplate has been noted in autopsy studies of human preterm newborns with periventricular leukomalacia (Robinson et al., 2006). Contrary to thalamic and basal ganglia neurons, which are vulnerable and often damaged, cortical layer neurons are still immature and less sensitive to hypoxic injuries. But a huge increase in cerebral cortical volume is documented due to an increase in volume of the neuropil of the cortex characterized by acceleration of dendritic differentiation and arborization, development of synapses, later-arriving GABAergic neurons, and proliferation of glial cells and processes. Since GABAergic neurons contribute to the thickness of upper cortical layers, the overall diminution of GABAergic neurons noted in the subplate could have important later structural and functional consequences. Moreover, the germinative zones are characterized by a high angiogenesis and a propensity to hemorrhage due to high expression levels of cyclooxygenase and vascular growth factor. The hemorrhage destroys the germinative zone and the associated venous infarction (intraparenchymal hemorrhage) damages the dorsal telencephalic subventricular zone and the overlying cerebral white matter. The consequences are a destruction of white matter axons, a loss of pre-oligodendrocytes, an interruption of thalamo-cortical axons, and an impairment of the development of the overlying cortical plate. p0145 Cerebral lesions in the full-term brain s0050 An enhanced gray matter vulnerability is observed at this step of brain development which is characterized by rearrangement of intracortical fibers and development of columnar circuitry, explosive formation of synapses, retraction of exuberant callosal axons, and growth of long cortico-cortical pathways stops (Kostovic and JovanovMilosevic, 2006). p0150 BIOCHEMICAL ASPECTS OF PERINATALLY ACQUIRED CELL DEATH AND PROCESS LOSS AND DEVELOPMENTAL DISORDERS Even if CP is most often caused by the interaction of several factors, it is likely that, whatever the causal factors, it results from common pathophysiological mechanisms. s0055 p0155 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. 6 p0160 M. STEPHANE ET AL. Key factors originating in cell death or cell process loss, observed in hypoxicischemic as well as in inflammatory conditions, consists of excessive production of proinflammatory cytokines, oxidative stress, deprivation of growth factors, extracellular matrix modification, and excessive release of glutamate, triggering the excitotoxic cascade. In preterm newborns, all these mechanisms result in a primary defect in myelination, gliosis, and thalamic degeneration with secondary cortical and thalamic maldevelopment. Microglial cells are the first elements to respond after any kind of injury. They could mediate neurotoxicity as they express both metabotropic and ionotropic glutamatergic receptors and adenosine receptors, which have been involved in the inflammatory response (Tahraoui et al., 2001; Pocock and Kettenmann, 2007). Oxidative stress and glutamate excitotoxicity account for the selective vulnerability of oligodendrocyte progenitor cells, which express the a-amino-3-hydroxy-5-methyl-4-isoazolepropionic acid (AMPA) receptor on their soma and the N-methyl-D-aspartate (NMDA) receptor on their processes (Karadottir and Atwell, 2007; Manning et al., 2008; Bakiri et al., 2009). Disturbances in the distribution of extracellular matrix, and cell or process death which produce axonal guidance molecules within the subplate zone and periventricular crossroads of growing axons, are important factors involved in the alteration of the development of cortical connections in preterm newborns (Kostovic and Jovanov-Milosevic, 2006). In full-term newborns, similar mechanisms induce a primary cortical and basal ganglia neuronal injury. During the immediate phase of reperfusion following diffuse hypoxiaischemia, the cellular energy failure induces in turn a failure of the Na þ/K þ ATPase pump, leading to depolarization of neurons, allowing the influx of Na þ and Ca2 þ water into the cell. The cytotoxic edema leads to cell death apoptosis or necrosis uckman et al., 2001). Moreover, excitotoxicity is (Gl€ due to the failure of energy-dependent reuptake of glutamate, the main excitatory neurotransmitter of the CNS, located at the presynaptic terminal and in the postsynaptic membranes at synapses in the brain. It promotes further influx of water by opening Na þ/K þ channels such as the AMPA receptor as well as Ca2 þ influx via the NMDA receptor. Glutamate receptors are developmentally regulated in both neurons and glia. Glutamatergic synaptic transmission is largely NMDA mediated during development. NMDA receptor density peaks in the early neonatal period followed by a peak in AMPA receptor density. The NMDA glutamate receptor is the predominant mediator of calcium-mediated excitotoxicity in neonatal hypoxicischemic brain injury, mainly through activation of neuronal nitric oxide synthase. The increase in Ca2 þ promotes free radical production, Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:45 Page Number: 6 Title Name: HCN cell membrane damage, and mitochondrial dysfunction, and mediates activation of genes involved in apoptosis. The first phase of cell death occurs immediately following the insult, and corresponds to the primary necrosis of neurons and glial cells. The second phase of cell death occurs hours or days following severe or irreversible injury, corresponding to the delayed form of cell death, known as apoptosis. Ischemia and many other acute, subacute, and chronic neurological processes trigger apoptosis by stimulating caspase or BAX activation, release of mitochondrial cytochrome C, upregulation of FAS death receptor, calpain activation, and PARP ( poly(ADP-ribose) polymerase) overactivation (Vexler and Ferriero, 2001). Other neurotransmitters such as acetyl-cholinergic or adenosine A2a receptors in microglia have also been implicated in these pathological pathways. The vulnerability of gray matter could e also be explained by the fact that in near full term there is a progressive functional maturation of GABAergic hyperpolarization allowing inhibition of neurotransmission parallel to the maturation of the KCC2 transporter expression with a laminar pattern of cortical development (Kostovic and Jovanov-Milosevic, 2006) and also by the fact that transient inhibition of NMDA receptors causes massive age- and region-dependent neuronal death in P0-P14 rat pups (Marret et al., 1995; Ikonomidou et al., 1999). This effect is specific for NMDA blockade and occurs during a stage of ontogenesis coinciding with a period of NMDA receptor hypersensitivity (Ikonomidou et al., 1989). Sex-dependent cell death pathways have been demonstrated in in vivo and in vitro models of hypoxiaischemia and oxidative stress. Males may be more vulnerable to glutamate-mediated excitotoxicity leading to PARP-1 activation and transfer of apoptosis-inducing factor (AIF) into the nucleus, which triggers apoptosis. Females are more vulnerable to oxidative stress, release of cytochrome C from mitochondria, and activation of caspase 3 to produce apoptosis (Johnston and Hagberg, 2007). In the hypoxic newborn mouse brain, a global dyssynchrony in the maturation program was observed: an accentuation of genes subserving presynaptic function contrasts with a suppression of genes involved in synaptic maturation, postsynaptic function and neurotransmission. Alteration in genes controlling myelination and cytoskeletal organization contributing to synapse maturation and neural transmission, enhancement of proapoptotic genes such as caspase 3, upregulation by hypoxia-inducible factor-1a (HIF1a) of vascularendothelial growth factor and its receptor flk-1 responsible for stimulation of angiogenesis, altered vascular permeability, notably in the subependymal zones, and p0165 p0170 p0175 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. PATHOPHYSIOLOGY OF CEREBRAL PALSY modification in neural differentiation were also observed (Curristin et al., 2002). CONCLUSION s0060 p0180 TS1 TS2 The development of cerebral palsy can be considered the result of a remarkable series of events that occur in the brain during its development, combining injury that is visible on MRI and developmental disturbance. Understanding all the pathways involved in cerebral palsy is crucial as it is likely that only a cocktail of molecules acting on different targets could prevent it. REFERENCES Adde-Michel C, Hennebert O, Laudenbach V et al. (2005). Effect of perinatal alcohol exposure in ibotenic acidinduced excitotoxic cortical lesions in newborn hamsters. Pediatr Res 57: 287–293. Als H, Gilkerson L, Duffy FH et al. (2003). A three-center, randomized, controlled trial of individualized developmental care for very low birth weight preterm infants: medical, neurodevelopmental, parenting, and caregiving effects. J Dev Behav Pediatr 24: 399–408. Badawi N, Kurinczuk JJ, Keogh JM (1998). Antepartum risk factors for newborn encephalopathy: the Western Australian case-control study. BMJ 317: 1549–1553. Bakiri Y, Burzomato V, Frugier G et al. (2009). Glutamatergic signalling in the brain’s white matter. Neuroscience 158: 266–274. Bauer CR, Langer JC, Shankaran S et al. (2005). Acute neonatal effects of cocaine exposure during pregnancy. Arch Pediatr Adolesc Med 159: 824–834. Bax M, Tydeman C, Flodmark O (2006). Clinical and MRI correlates of cerebral palsy The European cerebral palsy study. JAMA 296: 1602–1608. Beiano G, Khoshnood B, Kaminski M et al. (2010). Cerebral lesions and other prognostic factors for cerebral palsy in very preterm infants The EPIPAGE Prospective Cohort Study. Dev Med Child Neurol 52: e119–e125. Billiards SS, Haynes R, Folkerth RD et al. (2006). Development of microglia in the cerebral white matter of the human fetus and infant. J Comp Neurol 497: 199–208. Bolanos JP, Medina JM (1997). Effect of valproate on the metabolism of the central nervous system. Life Sci 60: 1933–1942. Curristin SM, Cao A, Stewart WB et al. (2002). Disrupted synaptic development in the hypoxic newborn brain. PNAS 99: 15279–15734. Duncan JR, Cock ML, Scheerlink JP et al. (2002). White matter injury after repeated endotoxin exposure in the preterm ovine fetus. Pediatr Res 52: 941–949. Expertise INSERM (2004). Déficiences et Handicaps D’origine Périnatale Dépistage et Prise en Charge. Editions INSERM, Paris pp. 1–376. Francis F, Meyer G, Fallet-Bianco C et al. (2006). Human disorders of cortical development: from past to present. Eur J Neurosci 23: 877–893. Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:45 Page Number: 7 Title Name: HCN 7 Gibson CS, McLennan AH, Goldwater PN et al. (2003). Antenatal causes of cerebral palsy: associations between inherited thrombophilias, viral and bacterial infection, and inherited susceptibility to infection. Obstet Gynecol Surv 58: 209–220. Girard S, Khadim H, Roy M et al. (2009). Role of perinatal inflammation in cerebral palsy. Pediatr Neurol 40: 168–174. Glass HC, Bonifacio SL, Chau V et al. (2008). Recurrent postnatal infections are associated with progressive white matter injury in premature infants. Pediatrics 122: 299–305. Gl€ uckman PD, Pinal CS, Gunn AJ (2001). Hypoxic-ischemic brain injury in the newborn: pathophysiology and potential strategies for intervention. Semin Neonatol 6: 109–120. Graham EM, Ris KA, Hartman AL et al. (2008). A systematic review of the role of intra-partum hypoxia-ischemia in the causation of neonatal encephalopathy. Am J Obstet Gynecol 12: 587–596. Gressens P, Hill JM, Gozes I et al. (1993). Growth factor function of the vaso-intestinal peptide in whole embryo cultures. Nature 362: 155–158. Guerri C (2002). Neuroanatomical and neurophysiological mechanisms involved in central nervous system dysfunctions induced by prenatal alcohol exposure. Alcohol Clin Exp Res 22: 304–312. Halliday HL, Ehrenkranz RA, Doyle LW (2009). Early (< 8 days) postnatal corticosteroids for preventing chronic lung disease in preterm infants. Cochrane Database Syst Rev CD001146. Hemminki K, Li X, Sundquist K et al. (2007). High familial risk for cerebral palsy implicates partial heritable aetiology. Paediatr Perinat Epidemiol 21: 235–241. Hjern A, Thorngren-Jerneck K (2008). Perinatal complications and socio-economic differences in cerebral palsy in Sweden: a national cohort study. BMC Pediatr 8: 49. Johnston MV, Hagberg H (2007). Sex and the pathogenesis of cerebral palsy. Dev Med Child Neurol 49: 74–78. Ikonomidou C, Mosinger JL, Salles KS et al. (1989). Sensitivity of the developing rat brain to hypoxic/ischemic damage parallels sensitivity to N-methyl-D-aspartate neurotoxicity. J Neurosci 9: 2809–2818. Ikonomidou C, Bosch F, Miksa M et al. (1999). Blockade of NMDA receptors and apoptotic neurodegeneration in the developing brain. Science 283: 70–74. Karadottir R, Atwell D (2007). Neurotransmitter receptors in the life and death of oligodendrocytes. Neuroscience 145: 1426–1438. Kirton A, de Veber G (2009). Advances in perinatal ischemic stroke. Pediatr Neurol 40: 205–214. Kostovic I, Jovanov-Milosevic N (2006). The development of cerebral connections during the first 2045 weeks’gestation. Semin Fetal Neonatal Med 11: 415–422. Livinec F, Ancel P-Y, Marret S, for the EPIPAGE group et al. (2005). Prenatal risk factors for cerebral palsy in very preterm singletons and twins. Obstet Gynecol 105: 1341–1347. Manning SM, Talos DM, Zhou C et al. (2008). NMDA receptor blockade with memantine attenuates white matter injury in a rat model of periventricular leukomalacia. J Neurosci 28: 6670–6678. To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. 8 M. STEPHANE ET AL. Marret S, Mukendi R, Gadisseux JF et al. (1995). Effect of ibotenate on brain development: an excitotoxic mouse model of microgyria and posthypoxic-like lesions. J Neuropathol Exp Neurol 54: 358–370. McQuillen PS, Ferriero DM (2004). Selective vulnerability in the developing nervous system. Pediatr Neurol 30: 227–235. Nelson KB (2008). Causative factors in cerebral palsy. Clin Obstet Gynecol 51: 749–762. Nelson KB, Grether JK (1997). Maternal infection and cerebral palsy in infants of normal birth weight. JAMA 278: 207–211. Pocock JM, Kettenmann H (2007). Neurotransmitter receptors on microglia. Trends Neurosci 30: 527–535. Petanjek Z, Berger B, Esclapez M (2009). Origins of cortical GABAergic neurons in the Cynomolgus monkey. Cereb Cortex 19: 249–262. Pharoah PO (2007). Prevalence and pathogenesis of congenital anomalies in cerebral palsy. Arch Dis Child 92: F489–F493. Robinson S, Li Q, De Chant A et al. (2006). Neonatal loss of g–aminobutyric acid pathway expression after perinatal brain injury. J Neurosurg 1046: 396–408. Scher AI, Petterson B, Blair E et al. (2002). The risk of mortality or cerebral palsy in twins: a collaborative populationbased study. Pediatr Res 52: 671–681. Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:46 Page Number: 8 Title Name: HCN Segovia KN, McClure M, Moravec M et al. (2008). Arrested oligodendrocyte lineage maturation in chronic perinatal white matter injury. Ann Neurol 63: 520–530. Shah DK, Doyle LW, Anderson PJ et al. (2008). Adverse neurodevelopment in preterm infants with post-natal sepsis or necrotizing enterocolitis is mediated by white matter abnormality on magnetic resonance imaging at term. J Pediatr 153: 170–175. Strijbis EM, Oudman I, van Essen P et al. (2006). Cerebral palsy and the application of the International criteria for acute intrapartum hypoxia. Obstet Gynecol 107: 1357–1365. Tahraoui SL, Marret S, Bodénant C et al. (2001). Central role of microglia in neonatal excitotoxic lesions of the murine periventricular white matter. Brain Pathol 11: 56–71. Vexler ZS, Ferriero DM (2001). Molecular and biochemical mechanisms of perinatal brain injury. Semin Neonatol 6: 99–108. Volpe JJ (2009). Brain injury in premature infants: a complex amalgam of destructive and developmental disturbances. Lancet Neurol 8: 110–124. Wu YW, Escobar GJ, Grether JK et al. (2003). Chorioamnionitis and cerebral palsy in term and near-term infants. JAMA 290: 2677–2684. Au2 Au2 To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter SPi. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. Non-Print Items ABSTRACT Au1 Cerebral palsy (CP), defined as a group of nonprogressive disorders of movement and posture, is the most common cause of severe neurodisability in children. Understanding its physiopathology is crucial to developing some protective strategies. Interruption of oxygen supply to the fetus or brain asphyxia was classically considered to be the main causal factor explaining later CP. However several ante-, peri-, and postnatal factors could be involved in the origins of CP syndromes. Congenital malformations are rarely identified. CP is most often the result of environmental factors, which might interact with genetic vulnerabilities, and could be severe enough to cause the destructive injuries visible with standard imaging (i.e., ultrasonographic study or MRI), predominantly in the white matter in preterm infants and in the gray matter and the brainstem nuclei in full-term newborns. Moreover they act on an immature brain and could alter the remarkable series of developmental events. Biochemical key factors originating in cell death or cell process loss, observed in hypoxicischemic as well as inflammatory conditions, are excessive production of proinflammatory cytokines, oxidative stress, maternal growth factor deprivation, extracellular matrix modifications, and excessive release of glutamate, triggering the excitotoxic cascade. Only two strategies have succeeded in decreasing CP in 2-yearold children: hypothermia in full-term newborns with moderate neonatal encephalopathy and administration of magnesium sulfate to mothers in preterm labor. Comp. by: S.Anand Stage: Proof Chapter No.: 16 Date:20/11/12 Time:21:18:47 Page Number: 9 Title Name: HCN