Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Complement system wikipedia , lookup
Major histocompatibility complex wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adaptive immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Innate immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
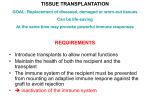
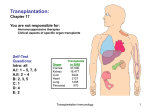
TISSUE TRANSPLANTATION GOAL: Replacement of diseased, damaged or worn-out tissues Can be life-saving At the same time may provoke powerful immune responses REQUIREMENTS • Introduce transplants to allow normal functions • Maintain the health of both the recipient and the transplant • The immune system of the recipient must be prevented from mounting an adaptive immune respone against the graft to avoid rejection inactivation of the immune system TRANSPLANTATION IMMUNOLOGY • THE ALLO-REACTIVE IMMUNE RESPONSE IS DIRECTED AGAINST TRANSPLANTATION ANTIGENS – Major transplantation antigens are encoded by classical MHC genes – Minor transplantation antigens are encoded by any polymorphic gene and are recognized as peptides in the context of MHC – Blood group antigens are considered as tissue-specific transplantation antigens • T CELLS ARE EDUCATED IN THE PRESENCE OF SELF MHC ALLOTYPES • OTHER MHC ALLOTYPES ARE RECOGNIZED AS FOREIGN BY T LYMPHOCYTES • REJECTION OF INCOMPATIBLE TISSUE IS MEDIATED PRIMARILY BY T LYMPHOCYTES • NK CELLS AND ANTIBODY MEDIATED EFFECTOR FUNCTIONS ARE ALSO INVOLVED ORGAN, TISSUE OR CELL TRANSPLANT AUTOLOGOUS autograft SYNGENIC syngraft Skin, muscle, stem cell, dendritic cell, cartilage BLOOD TRANSFUSION Bone marrow-derived haematopoietic cells (HSC) ALLOGENEIC allograft Kidney, cornea, liver, heart, lung bone marrow-derived haematopoietic cells (HSC) GRAFT REJECTION IS THE RESULT OF SPECIFIC IMMUNE RESPONSE Primary rejection mouse strain 10 days 6 months Lymphocyte transfer from immunized mouse Secondary rejection mouse strain 3 days - MEMORY Naive mouse Primary rejection mouse strain 10 days Rapid rejection of the transplant is mediated by a memory immune response Hyperacute rejection is caused by pre-existing antibodies binding to the graft. MECHANISMS OF TISSUE REJECTION • HYPERACUTE REJECTION – Xenograft or AB0 incompatible graft – Natural IgM antibodies against carbohydrates • Galα1-3Gal on xenograft endothelial cells – Antibodies generated upon previous blood transfusion, pregnancy or transplantation – MHC-specific antibodies bind to endothelial cells • Mismatch of recipient serum with donors B and T cells – Complement and clotting system – NK cell – mediated IgG-dependent ADCC – Necrotic tissue demage • EARLY ACUTE REACTION – 2 – 5 days – Previous sensitization of cytotoxic T cells – IgG-dependent ADCC – Necrotic tissue demage • LATE ACUTE and CHRONIC REACTION – 7 – 21 days – Th1 – mediated cellular immune response – Delayed Type Hypersensitivity • Fibrosis • Proliferation of smooth muscle cells • Atherosclerosis – Activation of cytotoxic T lymphocytes BLOOD GROUP AND HLA-SPECIFIC ANTIBODIES INDUCE HYPERACUTE REJECTION THROUGH COMPLEMENT ACTIVATION • THE TRANSFUSION REACTION IS MEDIATED BY ANTIBODIES – Red blood cells do not express MHC class I or class II molecules • A, B, 0 ANTIGENS are expressed by endothelial cells of blood vessels (solid vascularized organs) • ANTIBODIES to blood group antigens bind to blood vessels, activate complement – Type II hypersensitivity – Hyperacute rejection – cannot be reversed, should be avoided • Anti – HLA ANTIBODIES – Arise from pregnancy, blood transfusion, previous transplant – Cross match: test recipient’s serum to donor lymphocytes • • • • Panel reactive antibody (PRA) – % of positive reactions Complement activation Flow cytometry – more sensitive Separated T and B cells to detect MHC class I and MHC class II specific antibodies – Anti – MHC I react with both B and T lymphocytes – Anti – MHC II react with B lymphocytes only ORGAN, TISSUE OR CELL TRANSPLANTATION ALLOGENEIC Late Acute rejection: Both patients and the organ has tissue damage that releases danger signals – INFLAMMATION – ENHANCE MHC expression The immune response is mediated by CD4 and CD8 T-cells Effector mechanisms are identical to that of Type IV hypersensitivity Patients are prepared by administration of immunosuppressive drugs or T-cell specific antibodies prior to transplantation Transplant rejection Host versus graft HVG Acute rejection of a kidney graft through the direct pathway of allo-recognition. Acute rejection takes days to develop The rejected graft is swollen and has deep-red areas of hemorrhage and gray areas of necrotic tissue. Alloreactive T-cells of the recipient or of the donor Can be detected by Mixed Lymphocyte Reaction (MLR) PRESENTATION OF GRAFT - DERIVED PEPTIDES TO RECIPIENT’S T CELLS Recipient T Demaged, apoptotic/necrotic tissue cells and soluble proteins (MHC) Recipient peptide Donor Graft APC Recipient T Donor peptide Donor Recipient T peptide Recipient Host Recipient Donor APC T peptide DIRECT PRESENTATION INDIRECT PRESENTATION Host Versus Graft reaction HVG High percentage of T cells are activated DEPLETION OF GRAFT – DERIVED PROFESSIONAL APC REDUCES REJECTION Indirect presentation DC B MOLECULAR BASIS OF THE ALLO-RESPONSE RECIPIENT T CELLS ANTIGENS PRESENTED BY ALLO- AND SELF APC Allo-MHC + allo-peptide Allo-MHC + allo-peptide Allo-MHC + self-peptide Allo-MHC + self peptide Allo-MHC + any-peptide Allo-MHC + any-peptide Self-MHC + allo-peptide Self-MHC + allo-peptide Self-MHC + any-peptide HIGH PERCENTAGE OF RECIPIENT’S T CELLS ARE RESPONDING ACUTE REJECTION KIDNEY TRANSPLANTATION HEART TRANSPLANTATION T CELLS Plasma cells Lymphocytes and plasma cells around renal tubules. Occurs after terminating immune suppression (CSA) T lymphocytes in the myocardium. Labeled with anti-CD3 antibody REJECTION IS PRIMARILY MEDIATED BY MHC-SPECIFIC T LYMPHOCYTES BUT PLASMA CELLS ARE ALSO PRESENT Chronic rejection – may take months Targeted against the vasculature of the transplant Results in the thickening of the vessel wall and narrowing of the lumina E: endothel G: granulocyte T: alloreactive T M: macrophage EL: elastic lamina SMC: smooth muscle Chronic rejection Interstitial fibrosis and chronic inflammation. Renal arteries are fibrous and thickened. No treatment, can occur months or years after transplantation. Interstitial fibrosis after chronic rejection in transplanted kidney. SHORTAGE OF TRANSPLANTABLE ORGANS Animal organs – Xenogeneic transplantation Xenograft PRIMATES – danger of viral transmission PIG – equivalant organs size – hyperacute rejection „natural” anti-pig antibodies in human blood recognize carbohydrates on pig endothelial cells galactosyl α-1,3-galactosyl β-1,4-Nacetylglucosaminyl (Gal) Activate complement – cell damage Human decay acceleration factor (DAF) transgenic pig – several days KO - α-1,3-galactosyl transferase – 6 months survival BONE MARROW TRANSPLANTATION IS A SPECIAL CASE OF ORGAN TRANSPLANTATION Transplantation of the donor’s hematopoietic and immune systems to the recipient • Receipient’s immune response is inhibited – γ-irradiation, drugs – No rejection of the transplant – No host versus graft rejection • Donor bone marrow-derived mature T lymphocytes recognize recipient’s tissues – Graft versus host reaction - against all tissues – Acute autoimmun reaction, can be fatal – Elimination of mature T cells prevents GVH – Methotrexate and cyclosporin A inhibit GVHD – Elimination of mature T cells inhibits engraftment and anti-leukemia effect – may cause rejection DEFECTS OF HEMOTPOIETIC CELLS CAN BE CORRECTED BY BONE MARROW TRANSPLANTATION • Degree of HLA matching of the healthy donor and the patient determines the success of transplantation – Reduces alloreactions against the graft HVG – Reduces graft versus host reaction GVH – Ensures efficient presentation of graft antigens by graft APC in the thymus – Positive selection of graft T lymphocytes on host thymic epithelial cells will produce graft-derived T cells – shared MHC – The host’s immune system will be reconstituted by donor-derived lymphocytes ORGAN, TISSUE OR CELL TRANSPLANTATION Pre-treatment ALLOGENEIC Bone marrow Treat tumor Correct deficiency Cardiovascular diseases Transplant rejection Host versus graft HVG Graft versus Host GVH GVHD CYCLOSPORIN (CSA) AND TACROLIMUS (FK506) TCR/CD3 PLC INAKTIV PLC Ca2+ calcineurin calcineurin PTP-ase ACTIVE P NF-AT NF-ATc Dephosphorylation NF-AT translocation to the nucleus calcineurin PTP-ase calcineurin PTP-ase CsA Blocked by CSA and FK506 FK506 cyclophilin A isomerase NF-ATn FKBP12 isomerase NF-ATn TF Gene activation, expression of cytokines and activation molecules Some more ways to block the rejectionof transplants FTY720: Synthetic analogue of a fungal toxin called Myriocin. Sphingoson-like structure Agonist of the S1P receptor, alters T-cell recirculation, traps them in LNs Peripheral T-cell number is decreased, but no major T-cell defect! BONE MARROW TRANSPLANTATION Special case of tissue transplantation •Graft versus host reaction GVH Graft-donor T Recipient peptide •chronic and systemic • Mature T cells transplanted with the bone marrow react with recipient cells • Elimination of donor T cells can prevent GVHD Recipient APC survive •Graft versus host disease – GVHD Recipient peptide Graft-donor T Graft Versus Host Reaction •Elimination of donor T cells decreases graft versus leukemia effect •Bone marrow transplantation is used for correcting SCID Figure 11.1 The rash characteristic of GVHD often starts on the face. Also involves palms and soles Panel a: early GVHD in the skin. Lymphocytes are emerging from blood vessels (lower arrow) and adhering to the basal layer of the epidermis (upper arrow). Panel b: the basal cells of the epidermis begin to swell and vacuolate. ... GVHD in the colon Inflammatory cells have invaded the crypts of the intestine and destroyed the normal architecture (arrow). Photograph kindly provided by Mark Shlomchik.