Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hypothyroidism wikipedia , lookup
Sexually dimorphic nucleus wikipedia , lookup
Sex reassignment therapy wikipedia , lookup
Hormonal breast enhancement wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Hormone replacement therapy (menopause) wikipedia , lookup
Gynecomastia wikipedia , lookup
Hypothalamus wikipedia , lookup
Testosterone wikipedia , lookup
Polycystic ovary syndrome wikipedia , lookup
Androgen insensitivity syndrome wikipedia , lookup
Hormone replacement therapy (female-to-male) wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
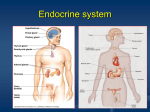
Reproductive SHBG Analyte Information -1- SHBG Introduction Sex hormone-binding globulin (SHBG), also known as sex steroid-binding protein (SBP) or testosterone-estradiol-binding globuline (TEBG), is the transport plasma glycoprotein that binds to specific sex hormones, namely testosterone, DHT and estradiol1. SHBG’s affinity is only for C18 or C19 steroid structures; affinity is also dependent on the relative orientation of the A- and B- steroid rings and the presence of a 17β-hydroxyl group1. Other steroid hormones such as progesterone, cortisol, and other corticosteroids are bound by transcortin. SHBG (Fig.1) consists of of two identical 373 amino acid chains and three oligosaccharide chains. Its molecular weight is 93 kDa. There is only one steroidbinding site per SHBG molecule. Fig.1: Sex hormone binding globulin with testosterone molecule -2- Biosynthesis SHBG is produced mainly in the liver (Fig.2) by hepatocytes and then released into the bloodstream. Small amounts are produced in the brain. In women, production sites include the uterus, placenta, ovaries and adrenal glands as well. In men, androgen binding protein (ABP) is produced by Sertoli cells in the testes. ABP has the same amino acid sequence as SHBG, but differs in its site of production and sugar moiety. SHBG synthesis is influenced by a number of hormonal and metabolic factors. Estrogens and thyroid hormones stimulate its synthesis, whereas androgens act as inhibitors. Other factors are mentioned in the paragraph “Levels”. Fig.2: Human liver Metabolism The biological half-life of SHBG is seven days. Its metabolic clearance is biphasic, with a fast initial distribution from the vascular compartment into extracellular space (half-life of a few hours), followed by a slower degradation phase (half-life of several days). -3- Physiological Function SHBG serves two roles: transporting and regulating the bioavailability of sex hormones. As a transport glycoprotein, SHBG binds to sex hormones such as testosterone, dihydrotestosterone (DHT), estradiol, estriol, estrone and dihydroepiandrosterone (DHEA), carrying them to target tissues via the bloodstream. These hormones are biologically inactive when bound, so SHBG also controls the amount of active sex hormones in circulation, while at the same time maintaining a reservoir of inactive hormones that are protected from degradation. Thus the bioavailability of these hormones is dependent on SHBG levels. Due to its greater affinity for DHT and testosterone than for estrone/estradiol, SHBG also greatly affects the balance of bioavailable androgens and estrogens. In the bloodstream, sex hormones circulate bound mostly to SHBG and to some degree to serum albumin. Only a small fraction is unbound/free (1-2%). The exact proportion of biologically active sex steroid hormones is a subject of ongoing research. It was previously believed that only the free fraction was biologically active; however, it has been confirmed that nearly all albumin-bound sex hormones are also available for tissue uptake. Thus the combined free and weakly-bound (i.e., albumin-bound) sex hormones are sometimes referred to as the bioavailable11 hormones. As mentioned above, sex steroid hormones bound to SHBG are considered biologically unavailable. It has recently been proved, however, that some tissues have plasma membrane receptors that can bind to the entire carrier protein-hormone complex. SHBGbound DHT can activate the membrane signaling mechanism in prostate cells, for instance, increasing cyclic adenosine monophosphate (cAMP) formation and mitogenesis7. SHBG may also have a function in other tissues that have receptors for DHT. Thus sex steroid hormones appear to act in tissues via two distinct receptor structures, steroid receptors and SHBG receptors (RSHBG). SHBG has very high affinity for dihydrotestosterone (DHT) and somewhat lower affinity for testosterone and estradiol (in that order) 3. Affinity for these steroids is on the order of Ka=1x 108-1x109. On the other hand, the capacity of SHBG for these hormones is low. Although each monomeric subunit contains one steroid binding site, the dimer tends to bind only to a single sex steroid hormone molecule. In comparison, albumin has a high capacity for sex steroid hormones, but its affinity for them is 100 times lower than that for SHBG. In males, approximately 44-65% of testosterone and 20% of estradiol circulate bound to SHBG. -4- The corresponding proportions in females are 66-78% and 40-60%, respectively. 1-2% circulate in free form in both sexes, and the remainder is bound to albumin. Levels SHBG levels depend on both sex and age. In fertile women, they are also affected by the phase of menstrual cycle. Serum SHBG levels are relatively low at birth, increase to high levels during infancy, and decrease during puberty1. Sexual dimorphism in serum SHBG levels becomes apparent during and after puberty due to androgen-mediated suppression of serum SHBG in males. Thus higher concentrations of SHBG levels are seen in women than in men. The highest SHBG serum levels of are found in pregnant women near term. Levels at the end of pregnancy may reach values five times the average for nonpregnant women. SHBG serum levels are affected by a number of factors that regulate SHBG synthesis and release. High androgen levels decrease SHBG concentrations; high levels of prolactin, insulin and insulin-like growth factor 1 (IGF-1) have the same effect. Other factors which decrease SHBG levels include obesity, female aging and menopause, glucocorticoids3 and administration of androgens. On the other hand, high estrogen and thyroid hormone levels increase SHBG concentration. Other factors which may increase SHBG levels include stress, male aging, high carbohydrate intake and drugs (e.g., antiepilepticum phenytoin, oral contraceptives). Circulating SHBG levels follow rhythmic variations . Daily variations in SHBG concentrations are similar to those of other proteins and albumins in serum, and are greatly affected by posture9. -5- Fig.3: Changes of SHBG levels during the life cycle Typical SHBG6 levels of children and adult males and females are given in the table 1. For each assay, the relevant reference values are shown in the appropriate Instructions for Use (IFU). -6- Table 1: Typical SHBG levels Specimen (serum) Reference interval (nmol/L) Puberty Tanner stage: Stage I male: 28.0-150 female: 39.0-176 Stage II male: 44.0-160 female: 7.20-107 Stage III male: 5.50-163 female: 28.0-171 Stage IV male: 13.0-88.0 female: 28.0-149 Stage V male: 10.0-60.0 female: 20.0-130 Adult male: 10.0-80.0 female: 20.0-130 pregnancy week 10-15 52-168 week 20-25 172-260 week 35-40 321 - -456 Diagnostic utility – prospects and possibilities As an analyte, SHBG is of great informational value due to its role in three regulatory circuits: the gonadal, thyroid and insular axes. Gonadal axis: The concentration of bound sex hormones significantly affects SHBG production. Its production is reduced in the presence of androgens, -7- including those administered externally; conversely, it is increased in the presence of estrogens, including some estrogen-containing contraceptives. Therefore even mild imbalances result in complications in both sexes. In cases of excessive estrogens (e.g., in boys with gynecomasty), SHBG tends to bind to androgens, rendering estrogens more pronounced. On the other hand, a predominance of androgens leads to a decrease in SHBG production; as a consequence, the proportion of free androgen grows in relation to that of bound androgen. Such a situation may occur in polycystic ovary syndrome (PCOS). Thyroid axis: SHBG levels correlate positively with thyroid hormone levels. Therefore SHBG levels are elevated in cases of hyperthyroidism and dimished in hypothyroidism. In subclinical situations, in which only TSH levels are outside normal limits (diminished in hyperthyroidism; increased in hypothyroidism), measurement of SHBG can serve as independent complementary, laboratory indicator. Insular axis: SHBG and insulin levels correlate negatively with one another. This is why we often find hirsutism in women with impaired insulin sensitivity and hyperinsulinemia (frequent in obese individuals): increased insulin production leads to a drop in SHGB levels, causing an elevation of free androgen concentration and ultimately hirsutism. The above-mentioned PCOS, for instance, is typically accompanied by a decrease in peripheral insulin sensitivity. SHBG levels are also diminished in cases of Reaven’s syndrome (hyperglycemia, hypertension, obesity, decreased HDL cholesterol, elevated triglycerides). Elevated SHBG levels are associated with the following conditions: - hyperthyroidism - excess of estrogens - gynecomastia in men (development of abnormally large mammary glands) - hypogonadism8, particularly in Turner’syndrome - growth hormone deficiency - anorexia nervosa - liver cirrhosis -8- SHBG levels are elevated in older men, pregnant women, postmenopausal women, and during use of oral contraceptives, hormonal replacement therapy, and administration of certain antiepileptic drugs. Decreased SHBG levels are associated with the following conditions: - hypothyroidism - acromegaly - Cushing’s syndrome - nephrotic syndrome - excess of androgens - hirsutism - polycystic ovary syndrome (PCOS)1,3 - obesity - hyperprolactemia - alopecia - Reaven’s syndrome SHBG concentrations may decrease during androgen treatment. Free Androgen Index (FAI): As previously mentioned, SHBG concentrations are influenced by androgen levels, primarily testosterone. Serum SHBG levels are inversely related to free, presumably bioactive testosterone concentrations4,5. There are a number of conditions and medications which may cause an increase or decrease in SHBG levels. At the same time, free testosterone levels may be changed without altering total testosterone levels, or vice versa. Thus, true androgen status can be assessed either by measuring free testosterone directly or by calculating the ratio of total testosterone (TT) to SHBG. This ratio is called the Free Androgen Index (FAI) or the Testosterone Free Index (TFI). FAI = TT (nmol/L)/SHBG (nmol/L) x 100 -9- Diagnostic utility-Practical applications SHBG levels are determined primarily in order to evaluate androgen status in men and women. Measurement of SHBG concentration is a useful tool in the evaluation of mild androgen metabolism disorders, and it identifies those women with hirsutism whoa are likely to respond to estrogen therapy. As the ratio of total testosterone to SHBG correlates well to both measured and calculated values for free testosterone, SHBG measurement helps to identify subjects with excessive androgen activity. Diagnosis and follow-up of women with symptoms or signs of androgen excess (PCOS and idiopathic hirsutism) Many conditions characterized by mild to moderate androgen excess in women, particularly PCOS, are associated with low SHBG levels. Most women with these conditions are also insulin resistant, and many are obese. A defect in SHBG production can lead to an excess in bioavailable androgens, which in turn causes an increase in insulin resistance that depresses SHBG levels even further. The Free Androgen Index (FAI) is lower than normal, while total testosterone remains normal. Thus an increase in free testosterone with a simultaneous decrease in SHBG is an indicator of possible PCOS. Monitoring sex steroid or anti-androgen therapy The primary method of monitoring sex steroid or antiandrogen therapy is direct measurement of the relevant sex steroids and gonadotropins. However, clinical assays are not available for many synthetic androgens and estrogens. In these instances, rises in SHBG levels indicate successful anti-androgen or estrogen therapy, while falls indicate successful androgen treatment. Diagnosis of disorders of puberty Boys with signs of precocious puberty may have elevated levels of SHBG. Diagnosis and follow up of anorexia nervosa Patients with anorexia nervosa have elevated SHBG levels. With successful treatment, levels start to fall and nutritional status improves. Normalization of SHBG levels precedes and may predict the normalization of reproductive function. - 10 - Diagnosis of thyrotoxicosis SHBG levels are elevated in instances of this condition. There are situations in which assessment of true thyroid status may be difficult: in patients with thyroid hormone transport protein abnormalities with suspected thyroid hormone resistance, or with suspected inappropriate thyroid stimulating hormone (TSH) secretion such as a TSH-secreting pituitary adenoma. In such cases elevated SHBG levels suggest tissue thyrotoxicosis, while normal levels indicate euthyroidism. In patients with gradually worsening thyrotoxicosis, serial SHBG measurement may assist in the timing of treatment (in addition to clinical assessment, thyroid hormone and TSH levels measurement). Diagnosis and follow-up of insulin resistance, and risk assessment of cardiovascular status and type II diabetes in women In patients with known insulin resistance, or with a high risk of type II diabetes, low SHBG levels may predict progressive insulin resistance, cardiovascular complications, and the progression of type II diabetes. Increased SHBG levels may indicate successful treatment. References 1. Hammond G.F.: Molecular properties of corticosteroid binding globulin and the sex-steroid binding proteins. Endocrin Rev, 1990, 11, 65-79 2. Tietz: Textbook of Clinical Chemistry, 3nd Ed., Burtis C.A., Ashwood E.R., eds. W.B. Saunders Company, 1999, p. 1603 3. Rosner W.: The functions of corticosteroid-binding globulin and sex hormonebinding globulin: recent advances, Endocrin. Rev., 1990, 11, 80-91 4. Mathur R.S., Moody L.O., Landgrebbe S., Williamson H.O.: Plasma androgens and sex hormone-binding globulin in the evaluation of hirsute patients, Fertil. Steril., 1981, 35, 29-35 5. Nanjee M.N., Wheeler M.J.: Plasma free testosterone. Ann. Clin. Biochem., 1985, 22, 387-390 6. Alan H.B. WU, PhD, DABCC, FACB: Tietz Clinical Guide To Laboratory Tests, 4th edition. W.B. Saunders Company, Philadelphia, 2006, 982-983 7. Rosner W., Hryd D.J., Khan M.s. et al.: Sex hormone binding globulin binding to cell membranes and generation of a second messenger, J.Androl., 1992, 13, 101106 - 11 - 8. Griffin J.E., Wilson J.D.: Disorder of testes and male reproductive tract. In Williams Textbook of Endocrinology, 8th ed. J.D.Wilson and D.W. Foster, Eds., Philadelphia, W.B.Saunders Co., 1992, pp. 799-852 9. Valero-Polito J., Fuentes-Arderiu X.: Daily rhythmic and non-rhythmic variations of follitropin, lutropin, testosterone and sex-hormone-binding globulin in men, Eur.J.Clin.Biochem., 1996, 34, 455-462 10. Stanczyk F.Z.: Steroid hormones In: Infertility, Contraception and Reproductive Endocrinology, 3rd ed., D.R.Mishell, V.Davajan and R.A.Lobo, Eds., Boston, Blackwell Scientifici Publications, 1991, pp. 53-76 1. - 12 -