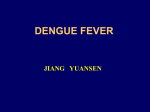
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Neonatal infection wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Infection control wikipedia , lookup
Adaptive immune system wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Monoclonal antibody wikipedia , lookup
West Nile fever wikipedia , lookup
Rheumatic fever wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Molecular mimicry wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Henipavirus wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Innate immune system wikipedia , lookup
This article was published in an Elsevier journal. The attached copy is furnished to the author for non-commercial research and education use, including for instruction at the author’s institution, sharing with colleagues and providing to institution administration. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright Author's personal copy Seminars in Diagnostic Pathology (2007) 24, 227-236 The pathology of dengue hemorrhagic fever Anthony S-Y. Leong, MBBS, MD, FRCPA, FRCPath, FCAP, FASCP, FHKAMed (Pathol), Hon FHKCPath, Hon FRCPT,a K. Thong Wong, MBBS, FRCPath,b Trishe Y-M. Leong, MBBS (hons), FRCPA, FCAP,c Puay Hoon Tan, MBBS, FAMS, MD, FRCPath, FRCPA,d Pongsak Wannakrairot, MD, FRCPTe a From the Hunter Area Pathology Service and University of Newcastle, Newcastle, Australia; Department of Pathology, University of Malaya, Selangor, Malaysia; c Victoria Cytology Service, Melbourne, Australia; d Department of Pathology, Singapore General Hospital, Singapore; and the e Department of Pathology, Chulalongkorn University, Bangkok, Thailand. b KEYWORDS Dengue hemorrhagic fever; Dengue virus; Inflammatory cytokines; Dendritic cells; Pathology; Hepatitis; Apoptosis; Immunology An estimated 2.5 billion people are at risk of dengue infection, and of the 100 million cases of dengue fever per year, up to 500,000 develop dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS), the life-threatening forms of the infection. The large majority of DHF/DSS occurs as the result of a secondary infection with a different serotype of the virus. While not completely understood, there is evidence that the target cells include dendritic reticulum cells, monocytes, lymphocytes, hepatocytes, and vascular endothelial cells. Viral replication appears to occur in dendritic cells, monocytes, and possibly circulating lymphoid cells, and damage to these and other target cells occurs through immune-mediated mechanisms related to cross-reacting antibodies and cytokines released by dendritic cells, monocytes, and vascular endothelium. There is evidence of a concomitant cellular activation as well as immune suppression during the infection. The activation of memory T cells results in cascades of inflammatory cytokines, including tumor necrosis factor-␣, interleukins (IL-2, IL-6, and IL-8), and other chemical mediators that increase vascular endothelial permeability or trigger death of target cells through apoptosis. Pathological studies in humans are uncommon, and a suitable animal model of DHF/DSS does not exist. The current treatment of DHF/DSS is symptomatic, and prevention is through vector control. As such, there is a great impetus for the development of vaccines and novel therapeutic molecules to impede viral replication in infected cells or counteract the effects of specific inflammatory mediators on target cells. The role of genetics in relation to resistance to DHF/DSS also requires clarification. © 2007 Elsevier Inc. All rights reserved. The global problem The first record of a disease clinically resembling dengue fever (df) can be found in a Chinese medical encyclopedia Address reprint requests and correspondence: Anthony S-Y Leong, MD, Hunter Area Pathology Service, Locked Bag 1, HRMC, Newcastle, NSW 2310, Australia. E-mail: [email protected]. 0740-2570/$ -see front matter © 2007 Elsevier Inc. All rights reserved. doi:10.1053/j.semdp.2007.07.002 dated 992.1 With the expansion of the world shipping trade in the 18th and 19th centuries, both the viruses and their principal mosquito vector, Aedes aegypti, were spread to new geographic regions, particularly along the tropical trading routes and shipping ports. Because spread was slow and via sailing ships, long intervals of 10 to 40 years separated epidemics of the disease. The expansion of dengue was closely related to development and economic growth in tropical countries and the mode of the viral transmission. Author's personal copy 228 Seminars in Diagnostic Pathology, Vol 24, No 4, November 2007 Economic growth is associated with transmigration of large numbers of the population into cities and the development of new cities; this urbanization resulted in a concomitant increase in breeding sites for the mosquito. Accelerated modern travel, particularly by airplanes, allows the introduction of the virus from an endemic area to a denguereceptive area where both the vector and susceptible population exist. The virus is usually carried in an infected but asymptomatic person during the incubation period of the disease, a method of transmission that often accounts for explosive outbreaks of df. In the latter part of the 20th century, globalization and rapid urbanization of many developing tropical countries produced increased transmission and hyperendemicity of the disease. Today, dengue is the most frequent arbovirus infection with more than 100 million cases annually throughout the world, including up to 0.5 million cases of dengue hemorrhagic fever (DHF) and 24,000 deaths.2,3 An estimated 2.5 billion people are at risk for the infection in the subtropical and tropical regions of the world,4 and recent years have witnessed unprecedented global dengue epidemics with large numbers of fatalities5; such statistics make df one of the most important arbovirus diseases in humans today. The magnitude of the global problem is compounded by the fact that there is currently no specific treatment or vaccines for the disease, and control is dependent largely on public health measures directed against the vectors. Presentation, pathogenesis, and pathology The Dengue virus (DV) is a positive-sense, singlestranded RNA surrounded by an icosahedral nucleocapsid. The virus is composed of three structural proteins [the capsid (C), premembrane (prM), and envelope (E) proteins] and seven nonstructural (NS1-7) proteins. With infection, the DV is endocytosed and acidic pH triggers a conformational change of the E protein. This allows fusion of the virus envelope to the endosomal membrane and release of the viral genome into the cytoplasm, where it is translated into viral proteins that replicate in the host endoplasmic reticulum. The newly synthesized viral genomes are packaged as viral core, envelope, and membrane proteins into immature virions before being secreted from the cell.6 The virus belongs to the family of Flaviviridae and the genus Flavivirus, which includes yellow fever, West Nile, Japanese encephalitis, and St. Louis encephalitis viruses. There are four distinct serotypes of DV (DEN1-4), and infection with any one of the serotypes confers lifelong immunity to that serotype. Whereas DVs exhibit 65% to 70% sequence homology, serotype cross-reactive immunity is only transient and wanes after 6 months so that the host remains susceptible to the remaining three heterologous dengue serotypes.7 Presentation DV infection results in protean manifestations ranging from a mild nonspecific or subclinical febrile illness to DHF or dengue shock syndrome (DSS). df uncomplicated has an incubation period of 5 to 9 days. The clinical features are age-dependent. Infants and young adults may only have simple fever with a maculopapular rash. In older children and adults, df is characterized by the sudden onset of high fever of about 40°C, chills, severe headache that is mostly frontal or retro-ocular, skin rash, general malaise, and severe muscle ache in the lumbar region, legs, and joints. There is loss of appetite with nausea and vomiting, and photophobia with puffiness of the eyelids and cervical lymphadenopathy may be present. The fever lasts for 2 to 4 days, and after an afebrile period of about 1 day, a second febrile period may follow, producing the typical “saddle back” temperature curve. At this stage, an itchy maculopapular rash develops, often spreading from the extremities to the trunk to involve the entire body, except for the face. The palms and soles may also be red. Convalescence can take several weeks or months, but there is virtually no mortality associated.8 The triad of fever, rash, and arthralgia requires separation from other nonarbovirus infections, such as measles, rubella, Epstein–Barr virus, cytomegalovirus, and protozoan infections such as toxoplasmosis. Due to the wide clinical variation, it is not possible to make a definite diagnosis on clinical findings alone. A positive tourniquet test (ⱖ10 petechiae/inch2 read 1 minute after release of 5 minutes of pressure midway between systolic and diastolic) and leukopenia (WBC ⱕ5000 cells/mm3) in a febrile patient is highly predictive but still nonspecific for df. Real-time polymerase chain reaction (RT-PCR) to detect the virus remains the gold standard, although this test is not available in many developing nations. The World Health Organization (WHO) distinguishes DHF/DSS from df with hemorrhage, which is considered a mild disease.9 DHF/DSS is associated with poorer outcomes and a mortality rate that approaches 5%.10 The classical features of DHF are high fever, increased vascular permeability with hemorrhagic manifestations, thrombocytopenia (platelet count ⱕ100,000/mm3), and hemoconcentration or signs of plasma leakage. DSS is defined as DHF plus either hypotension for age or narrow pulse pressure in the presence of clinical signs of shock. The increased capillary permeability is generally not accompanied by morphological damage to the capillary endothelium, and there are altered numbers and functions of leukocytes, increased hematocrit, and thrombocytopenia. Raised levels of aspartate-amino-transferase (AST) and alanine amino-transferase (ALT) have been observed in 98% and 37% of patients, respectively, indicating that liver dysfunction is a very common occurrence in DHF.11 As dengue spreads worldwide, there is evidence that the four key criteria of severe disease employed in the WHO grading system (shock, plasma leakage, marked thrombocytopenia, and internal hemorrhage) may not be universally Author's personal copy Leong et al Dengue Hemorrhagic Fever applicable, and many severe cases (including those that involve shock and fatality) may be missed, especially as the criteria were based on initial observations in children with the disease in Southeast Asia.12 Other less common manifestations include neurological symptoms from cerebral edema and encephalopathy from hepatic failure, complications of disseminated intravascular coagulopathy, diastolic dysfunction, abdominal compartment syndrome, adult respiratory distress syndrome,13 acute renal failure,14 postinfectious fatigue syndrome,15 intracranial hemorrhage,16 fulminant hepatitis,17 acute abdomen,18 hemophagocytic syndrome and dyserythropoiesis,19 and myocarditis.20 Pathogenesis The pathogenesis of DHF/DSS is poorly understood and has been the subject of much research interest in recent years. Although df is a self-limiting disease in the great majority of cases, the problem becomes a significant one as the large numbers of infected persons result in about half a million cases per year of potentially life-threatening DHF/ DSS. Up to 90% of DHF/DSS cases occur in secondary heterologous DV infection; the remaining are primary infections, usually in infants between 6 and 12 months of age. Clearly, secondary infection with a heterologous dengue serotype is a major risk factor. To date, several immunological aspects of DV infection have been studied in detail. These relate to the target cells of the virus and their immunological effects and the effects of antibody-mediated mechanisms in heterologous secondary infections. Antibody-enhanced viral duplication After introduction of the dengue virus through the bite of an infected Aedes mosquito, local viral duplication is thought to take place in target epidermal dendritic cells that are up to 10 times more permissive to dengue infection than monocytes or macrophages. A C-type lectin expressed by the dendritic cells can bind to the dengue envelope (E) protein and probably serves as a coreceptor for viral entry.21,22 Migration of interdigitating dendritic cells to regional lymph nodes also allows transfer of the virus to T cells. IgG antibodies and enhancement via IgM and complement C3 receptors have been implicated in dendritic cell infection.23,24 The infection of CD14-positive dendritic cells as well as bone marrow dendritic cells leads to the production of TNF-␣, IFN-␣, and IL-10 and inefficient maturation of infected dendritic cells, which undergo apoptosis. The dendritic cells display impaired ability to upregulate cell surface expression of costimulatory, maturation, and major histocompatibility complex molecules, resulting in reduced T cell stimulatory capacity. There is also an impaired ability to stimulate allogenic T cells, which is accompanied by further enhanced IL-10 production.25,26 These findings suggest a possible immune evasion strategy of the virus by impairing antigen-presenting cell function through matura- 229 tion blockade and induction of apoptosis.27 Natural killer cells, which comprise another arm of the innate immune system, may also play a role. These cells can clear virusinfected cells either by direct cytotoxicity or via antibodydependent cell-mediated cytotoxicity. Dengue immune serum has been shown to mediate antibody-dependent cellmediated cytotoxic lysis of DV-infected cell lines.28 Research into the effects of primary DV infection has been hampered by the absence of a true animal model of the disease. Nonhuman primates display viremia but not DHF. Several promising murine models of DV infections have recently been developed, including interferon-␣/ and ␥ receptor-deficient mice that developed encephalitis and nonobese diabetic/severe combined immunodeficent mice reconstituted with human hematopoietic stem cells with skin erythema.29,30 Not surprisingly, because of the severity and mortality associated with DHF immunological reactions, secondary heterologous DV infections have been extensively studied. Antibody-dependent enhancement is one mechanism that has been proposed to explain the severity of DHF/DSS. This mechanism evokes the binding of preexisting dengue antibodies at nonneutralizing conditions to heterologous DV to enable viral entry into FcRII-bearing target cells.31 The target cells are predominantly cells of the reticuloendothelial system of spleen, liver, and bone marrow, including monocytes, lymphocytes, Kupffer cells, and alveolar macrophages.32 The enhanced viral entry into such cells produces an increased viral burden in the host. Anti-E antibodies enhanced infection via FcRII, whereas antiprM antibodies enhanced infection of both FcRII- and nonFcRII-bearing cells.33 Some studies have demonstrated an association between viral burden and disease severity,34,35 with the ability of preinfection plasma to enhance infection of monocytes corresponding to disease severity.36 However, a more recent study contradicts those findings by showing no association between the ability of preillness plasma to enhanced infection in vitro and subsequent dengue viremia or disease severity in secondary dengue-2 or dengue-3 virus infections.37 In the small percentage of DHF cases that manifest during primary DV infection, usually in infants, it has been postulated that maternal transmission of nonneutralizing DV antibodies result in the same phenomenon as described above in adults with secondary infections.38 Although the viral envelope glycoprotein E is responsible for viral attachment and entry, and is the antigenic target for neutralizing antibodies, there are also several viral nonstructural proteins that are involved in viral replication and have other effects in vivo. The dengue nonstructural protein NS1 has both a secreted and cell-associated form. Secreted NS1 levels have been found to be associated with viremia levels in secondary dengue-2 infection.39 Anti-NS1 antibodies appear to have both a protective as well as pathogenic role in DV infection. In animal models, anti-NS1 antibodies protect against lethal flavivirus challenge,40,41 but these Author's personal copy 230 Seminars in Diagnostic Pathology, Vol 24, No 4, November 2007 antibodies to NS1 have also been suggested to have a direct role in the pathogenesis of vascular leakage. Sera from acute dengue-infected individuals are able to bind to human umbilical cord endothelial cells, and this process can be blocked by the addition of recombinant NS1.42 Furthermore, the treatment of such umbilical cord cells with murine antidengue NS1 antibodies, but not Japanese encephalitis NS1 antibodies, induced the production of IL-6, IL-8, and monocyte chemo-attractant protein type 1, an inflammatory response that was abrogated in the presence of recombinant dengue NS1.43 Anti-NS1 antibodies have also been implicated to cause damage to endothelial cells by inducing nitric oxide-mediated apoptosis.42 Antibodies to NS1 persist long after dengue infection has resolved but do not cause pathology. Furthermore, the persistence and kinetics of development of anti-NS1 antibodies during and after secondary DV infection do not correlate with the timing of plasma leakage, raising questions as to the clinical relevance of this in vitro evidence for molecular mimicry. On primary infection with DV, antibodies are generated against NS1 and the viral envelope protein E. Serotypespecific and serotype cross-reactive neutralizing antibodies are directed against the E protein. Enhancing antibodies can affect the severity of the disease as long as 20 years after the primary infection, especially during dengue-2 and dengue-3 infection following a primary infection with dengue-1 virus.44 However, all serotypes have been shown to be capable of causing severe disease,45 and milder disease is associated with lower viral loads and high levels of preexisting heterotype neutralizing antibodies during the secondary infection. This is not necessarily always true; in the case of secondary dengue-3 virus infection, higher levels of these cross-reactive memory humoral immune responses appeared to be beneficial as demonstrated by reduced viremia levels and decreased disease severity, but the same did not hold true for secondary dengue-1 or dengue-2 virus infection.46 Immunological mechanisms The observation that onset of plasma leakage occurs up to several days following significant reduction or clearance of viremia suggests that, instead of the proposed antibodydependent enhancement due to viral burden, an immunemediated mechanism may be responsible for the extreme capillary permeability that is characteristic of DHF/DSS. Furthermore, despite high viral loads in secondary infections, progression to more severe forms of the infection occurs only in ⬍5% of cases. Serotype-specific and crossreactive T cells have been detected in the peripheral blood of individuals with acute DV infections. It is suggested that these serotype cross-reacting T cells show low affinity for the infecting virus and a higher affinity for another virus serotype (presumably from a previous infection), a phenomenon called the “original antigenic sin.”47 However, definite identification of the primary infecting DV serotype is difficult because neutralizing antibodies can be highly serotype cross-reactive after secondary infection, a caveat that questions the validity of this hypothesis.27 Importantly, it has been dem- onstrated that cross-reactive dengue-specific T cells induce high levels of cytokine production that may lead to increased vascular permeability.48 CD4 and CD8 T cell responses after primary DV infection have shown interesting differences. CD4⫹ T cells produced greater amounts of IFN-␥ to homologous DV antigens, but the ratio of TNF-␣ to IFN-␥ was higher after stimulation with heterologous serotype antigens or CD4⫹ T cell epitopes.49 CD8⫹ T cells have shown partial agonist responses in vitro in which a heterologous serotype variant could sensitize target cells for lysis but not cytokine production or proliferation. Several studies have suggested a possible role for “immunodominant” variants of dengue epitopes in which the sequence of DV serotypes may influence the risk of DHF/ DSS. Human leukocyte antigen (HLA) A2-restricted CD8⫹ T cell responses in primary dengue-immune individuals have shown both quantitative as well as qualitative differences in their cytokine responses to variant dengue epitopes, suggesting that previous infection as well as the sequence of heterologous DV infections may affect subsequent clinical outcome.50 For some epitopes, a single dengue variant was able to elicit the highest response in all donors, regardless of infecting serotype, suggesting that certain epitopes may be immunodominant. A recently identified dengue HLA-A11restricted NS3 T cell epitope has also been found to be presented by HLA A24, an unexpected finding because these alleles belong to different HLA superfamilies.48 Previous infection history to unrelated viruses can also lead to immunopathology, as shown in human and animal models.51 The studies performed so far appear to show a concomitant cellular activation as well as immune suppression during acute DV infection. T cell proliferation to mitogens is impaired during the acute infection, and this appears to be caused by a defect in the antigen-presenting cell.52 There is an impairment of the normal plasmacytoid dendritic cell response in children who subsequently develop DHF. This blunted response is thought to result in inadequate control of viremia with the subsequent enhanced activation of crossreactive memory T lymphocytes resulting in DHF.53 Overall numbers of CD4 and CD8 T cells, natural killer cells, and ␥␦ T cells have been found to be decreased in DHF compared with df, but despite their reduced numbers, CD8 and natural killer T cells expressed higher levels of the activation marker CD69 in patients with DHF compared with uncomplicated df. It has been shown that low affinity memory T cells occur at higher levels than cytotoxic T cells, the latter being lost through apoptosis,47 and DV epitopespecific T cell responses are associated with disease severity.47 Dengue-specific T cells are increased in DHF, but peripheral blood mononuclear cells are unable to produce IFN-␥ in response to dengue epitope stimulation,48 reflecting the reduced ability of monocytes and dendritic cells to present antigen adequately. Alternatively, antigen-induced cell death may ensue after the in vitro stimulation of re- Author's personal copy Leong et al Dengue Hemorrhagic Fever cently activated CD8 T cells,52 a finding that has been directly demonstrated.48,54 The short-lived nature of plasma leakage syndrome seen in DHF is another point to support a functional rather than destructive effect of DV infection on endothelial cells. In vitro studies of human endothelial cell lines infected with DVs can produce pro-inflammatory mediators such as IL-6 and IL-8 RANTES (regulated on activation; normal T cell expressed and secreted), alter intercellular cell adhesion molecule type 1 surface expression and actin cytoskeleton structure, and increase permeability to small molecules.55,56 These effects could be partially reversed by neutralizing antibodies directed against IL-8.55 Also, the infection of human umbilical cord endothelial cells with DV in the presence of antidengue immune serum induced the formation of activated complement via both classical and alternative pathways with complement activation appearing to be mediated by dengue NS1 protein.57 Serum from patients with acute dengue infection induced the activation and apoptosis of cultured endothelial cells that could be partially reversed by anti-TNF-␣ monoclonal antibodies, further supporting the role of inflammatory mediators for plasma leak- A C 231 age.58 A recent murine model for DV-induced lethal vascular permeability has also demonstrated the importance of TNF-␣ as a key mediator of DV induced in mice.59 The presence of IgM, -1-globulin, and fibrinogen has been demonstrated in the cutaneous vessels of patients with DHF with dengue antigen in perivascular mononuclear cells, indicating that the skin rashes associated with DHF are immune-mediated.60 Cytokine cascades, complement, and other mediators Although incomplete, the current evidence suggests that, after massive activation of memory T cells, a cytokine cascade that targets vascular endothelial cells is primarily responsible for the critical leakage of fluid and protein in DHF/DSS. Such cytokines, including IFN-␥, TNF-␣, IL-2, IL-6, IL1-, and IL-8, are released in high concentrations mostly by T cells, monocytes/macrophages, and endothelial cells and are demonstrable in the serum of patients with DHF/DSS. More recent studies have confirmed the presence of elevated levels of IFN-␥, TNF-␣, and IL-10 in patients from Vietnam, India, and Cuba.61-63 Such cytokines have the potential to induce the release and production of other B D Figure 1 Organs from a 2-year-old Thai boy who died from dengue hemorrhagic fever. (A) The eviscerated intestines were markedly edematous and focally hemorrhagic, and there was a hemoperitoneum of 300 mL. (B) The kidneys were edematous with focal hemorrhage and hemorrhage into the calyces and renal pelvis. (C) The liver was swollen with focal hemorrhage. (D) Both lungs were heavy and beefy in consistency and hemorrhagic. Author's personal copy 232 Seminars in Diagnostic Pathology, Vol 24, No 4, November 2007 cytokines so that a complex interactive network results in further increases in the levels of cytokines and other chemical mediators in a cascade, often with synergistic effects on vascular permeability. IFN-␥ is also able to upgrade the expression of Fc␥ receptors on monocytes and macrophages, further facilitating viral replication. Although this cascade of cytokine activation and production stimulated by memory T cells is an attractive proposition in adult DHF/ DSS, it fails to explain the occurrence of this severe form of dengue infection in the primary infection of infants born of dengue-immune mothers. Complement has been suggested to have a role in the immunopathogenesis of DHF/DSS, although its cause remains unknown. Large amounts of dengue NS1, complement anaphylatoxin C5a, and the terminal complement complex SC5b-9 were found in pleural fluids of patients with DHF/DSS.57 Other mediators, such as histamine, tissue plasminogen activator, and macrophage inhibitory factor, have also been found in this disease.64,65 Together with the endothelial permeability seen in DHF, there is a marked thrombocytopenia. This has also been seen in df, although the drop in platelet numbers is less marked. It has been suggested that there is transient suppression of hematopoiesis, although megakaryocytes have not been shown to be infected with the virus.66 Other suggestions for the thrombocytopenia include binding of the virus to platelets in the presence of virus-specific antibody, antivirus antibodies that cross-react with human platelets, and antiplatelet antibodies, the latter in a mouse model.67 The elevation of serum liver enzymes is a frequent finding in DV infection, and infrequently midzonal necrosis is demonstrable in the liver and fulminant hepatitis may occur. Hepatocytes are therefore a likely target for the virus. In vitro infection of HepG2 cells results in apoptosis mediated by TNF-related apoptosis-inducing ligand and other chemokines, such as IL-8, RANTES, and monocyte chemoattractant proteins, with evidence that these actions may be mediated by NS5 protein.68 Other mediators, such as histamine, tissue plasminogen activator, and macrophage migration inhibitory factor, have also been implicated in the pathogenesis of the severe forms of dengue infection.69 volume with augmented endocapillary and mesangial cellularity. Children who die from DHF have entensive edema of viscera with leakage of blood and focal hemorrhage (Figure 1). In a study of five fatal cases of DHF in Vietnamese children, severe hepatitis was observed with midzonal necrosis and micro-vesicular steatosis, although in one patient the liver appeared normal. The necrotic areas showed apoptosis by the TUNEL technique, with destruction of both hepatocytes and Kupffer cells, and there was no recruitment of polymorphonuclear cells or lymphocytes.71 Another study of nine fatal cases with fulminant hepatitis confirmed the presence of DV cDNA by reverse transcriptase in situ PCR in more than 80% of the hepatocytes and in many Kupffer cells. Five livers showed massive hepatocyte necrosis or apoptosis with no accompanying involvement of bile ducts (Figure 2). There was rare bile canalicular cholestasis, and micro-vesicular steatosis was common. The pauci-cellular areas of massive hepatic necrosis showed only rare Kupffer cells to be positive for TNF-␣ and IL-272 compared with the upregulation of these and many other cytokines seen in the livers of fatal cases of hepatitis C. Thrombotic microangiopathy may be observed in the glomeruli (Figure 3), most likely the result of disseminated intravascular coagulopathy from hemoconcentration.14 Localization of DV antigen and RNA by immunohistochemistry and in situ hybridization confirmed the presence of viral antigens in Kupffer cells, lymphoid cells in the splenic red and white pulp, renal tubular epithelium, vascular endothelium of the liver and lung, monocytes in the liver, spleen, and lung, and peripheral blood monocytes and lymphocytes (Figure 4 A and B), although high levels of Pathology There are a limited number of morphological studies in DHF/DSS. In BALB/c mice inoculated with dengue-2 obtained from human serum, focal alterations were found in the liver, kidney, lung, and cerebellum. The presence of the virus in these organs was confirmed by ultrastructural and immunolocalization techniques in mosquito cell cultures of the infected tissues.70 Hepatocytes were ballooned; portal and centrilobular veins were congested; lungs were focally hemorrhagic with vascular congestion and focal alveolitis; cerebellar tissue displayed focal neuronal compaction and perivascular edema; and there was increased glomerular Figure 2 Liver biopsy from a 13-year-old Chinese boy from Singapore who presented with dengue hemorrhagic fever and fulminant hepatitis. The needle core biopsy showed extensive pauci-cellular necrosis concentrated in the midzone, but in areas tending to involve the entire lobule, the portal tract elements were not involved (arrows). The nuclear debris represented apoptotic bodies. Author's personal copy Leong et al Dengue Hemorrhagic Fever 233 vesicles in cutaneous vascular endothelium has suggested that the presence of viral antigen in these cells represents endocytosis and not infection.73 Genetic predisposition and resistance Figure 3 A 46-year-old Chinese woman with dengue hemorrhagic fever. Her hemoglobin was 3 g/dL, platelets 64,000/dL, and hematocrit 26.4%. Peripheral blood flim showed no evidence of fragmented cells. Thrombotic microangiopathy was evident in the renal biopsy (arrows, methanamine silver). viral RNA were only found in the antigen-bearing cells of the spleen and peripheral blood supporting viral replication in these latter cells (Figure 4C and D).32 Viral antigen was present in the endothelium of the organs studied, but there was no evidence of viral replication. The presence of increased numbers of ultrastructural vacuoles and pinocytic The patient’s genetic background appears to be a critical factor in determining progression to DHF/DSS. Outbreaks in Cuba have shown a reduced risk of people of Negroid race for DHF/DSS compared with those of Caucasoid race,74 an observation coinciding with the low reported incidence of dengue disease in African and Black Caribbean populations. Although dengue has been documented in 19 African nations and the virus repeatedly isolated, only sporadic cases of dengue have been reported, and mainly in nonindigenous populations. Even when outbreaks have been reported in Africa and the Seychelles, the clinical manifestations have been very mild.75 There is a clear absence of DHF/DSS despite hyperendemic dengue virus transmission in the Haiti,76 this despite the annual infection rate in Port-au-Prince being about 30% higher than that of Yangoon, Myanmar, where DHF/DSS rates and fatalities are high. Although polymorphic genes have been suggested as possible contenders to account for the genetic susceptibility, the HLA region is an obvious candidate as it encodes several proteins involved in the immune response, including complement and TNF-␣. Certain HLA types have been both A B C D Figure 4 Avidin– biotin peroxidase staining with antidengue polyclonal antibodies for three serotypes (hyperimmune mouse ascitic fluid; kindly provided by R.E. Shope. WHO Centre for Tropical Diseases, University of Texas Medical Branch, Galveston, TX). (a) Staining was seen in Kupffer cells. (b) The antigen was present in the white pulp of the spleen as well as in scattered larger monocytes in the red pulp. (c) In situ hybridization showed viral genome in macrophages and stimulated lymphoid cells of the splenic red pulp and peripheral blood monocytes (d).32 Author's personal copy 234 Seminars in Diagnostic Pathology, Vol 24, No 4, November 2007 positively and negatively associated with DHF. For example, variations in HLA-A locus were significantly associated with susceptibility to DHF/DSS77; HLA-DR04 has the reverse association.78 Genetic background may also be related to the proliferation of low-affinity T cells, or the persistence of cytokine production by these cells, or both factors together. Conclusions Current information on the immunopathogenesis of DHF/ DSS is still fragmentary. The severe forms of the DV infection occur as secondary infections. The target cells appear to be dendritic cells, monocytes, hepatocytes, T lymphocytes, and possibly vascular endothelial cells. The disease results from two major immune mechanisms that involve the production of nonneutralizing enhancing antibodies that cross-react between the serotypes of DV enhancing viral entry into dendritic cells and monocytes to increase the viral load and produce inefficient maturation of the infected cells. The other component of the immune response involves the massive activation of memory T cells sensitized in a previous infection. This activation results in the proliferation and release of pro-inflammatory cytokines and a cytokine cascade that targets the susceptible cells causing cell death through apoptosis and is responsible for the fluid and protein leakage and the liver damage characteristic of DHF/DSS. Research is hampered by the absence of a suitable animal model for DHF/DSS, and detailed pathological studies in humans are few. Current treatment is largely symptomatic, and prevention is through vector control, making it imperative that greater understanding of the pathogenesis be achieved with the view of developing novel molecules to inhibit viral replication and to stem the damaging effects of immune mediators. There is also impetus for vaccine development, and a greater understanding of the relation of resistance to the severe forms of the infection and genetics is needed. References 1. Gubler DJ: Dengue/dengue hemorrhagic fever: history and current status. Novartis Found Symp 277:3-16, 2006 2. Gubler DJ: Dengue and dengue hemorrhagic fever. Clin Microbiol Rev 11:480-496, 1998 3. Gibbons RV, Vaughn DW: Dengue: an escalating problem. Br Med J 324:1563-1566, 2002 4. Burke DS, Monath TP: Flaviviruses, in Knipe DM, Howley PM (eds): Fields Virology (ed 4, vol 1). Philadelphia, PA, Williams and Wilkins, 2001, pp 1043-1126 5. Chaturvedi UC, Nagar R, Shrivastava R: Dengue and dengue hemorrhagic fever: implications of host genetics. FEMS Immunol Med Microbiol 47:155-166, 2005 6. Fink J, Gu F, Vasudevan SG: Role of T cells, cytokines and antibody in dengue fever and dengue hemorrhagic fever. Rev Med Virol 16: 263-275, 2006 7. Halstead SB: Neutralization and antibody-dependent enhancement of dengue viruses. Adv Virus Res 60:421-467, 2003 8. Fernando RL, Fernando SSE, Leong AS-Y: Tropical Infectious Diseases. London, Greenwich Medical Media, 2001, pp 279-280 9. World Health Organisation: Dengue Hemorrhagic Fever: Diagnosis, Treatment, Prevention and Control (ed 2). Geneva, World Health Organisation, 1997 10. Wilder-Smith A, Schwartz E: Dengue in travellers. N Engl J Med 353:924-932, 2005 11. Nugyen TL, Nguyen TH, Tien NT: The impact of dengue hemorrhagic fever on liver function. Res Virol 148:273-277, 1997 12. Balmeseda A, Hammond SN, Perez MA, et al: Short report: assessment of the World Health Organisation scheme for classification of dengue severity in Nicaragua. Am J Trop Med Hyg 73:1059-1062, 2006 13. Kamath SR, Ranjit S: Clinical features, complications and atypical manifestations of children with severe forms of dengue hamorrhagic fever in South India. Indian J Pediatr 73:889-895, 2006 14. Boonpucknavig V, Soontornniyomkij V: Pathology of renal diseases in the tropics. Semin Nephrol 23:88-106, 2003 15. Seet RCS, Quek AML, Lim ECH: Post-infectious fatigue syndrome in dengue infection. J Clin Virol 38:1-6, 2007 16. Kumar J, Kumar A, Gupta S, et al: Dengue hemorrhagic fever: an unusual cause of intracranial hemorhage. J Neurol Neurosurg Psychiatry 78:253, 2007 17. Ling LM, Wilder-Smith A, Leo YS: Fulminant hepatitis in dengue hemorrhagic fever. J Clin Virol 38:265-268, 2007 18. Khor BS, Liu JW, Lee IK, et al: Dengue hemorrhagic fever patients with acute abdomen: clinical experience of 14 cases. Am J Trop Med Hyg 74:901-904, 2006 19. Lu PL, Hsiao HH, Tsai JJ, et al: Dengue virus-associated hemophagocytic syndrome and dyserythropoiesis: a case report. Kaohsiung J Med Sci 21:34-39, 2005 20. Wiwanitkit V: Dengue myocarditis, rare but not fatal manifestation. Int J Cardiol 10:122, 2006 21. Pokidysheva E, Zhang Y, Battisti AJ, et al: Cryo-EM reconstruction of dengue virus in complex with the carbohydrate recognition domain of DC-SIGN. Cell 124:485-493, 2006 22. Pulendren B, Ahmed R: Translating innate immunity into immunological memory: implications for vaccine development. Cell 124:849863, 2006 23. Cardosa MJ, Porterfield JS, Gordon S: Complement receptor mediates enhanced Flavivirus replication in macrophages. J Exp Med 158:258263, 1983 24. Gollins SW, Porterfield JS: A new mechanism for the neutralisation of enveloped viruses by anti-viral antibody. Nature 321:421-467, 1986 25. Palmer DR, Sun P, Celluzzi C, et al: Differential effects of dengue virus on infected and bystander dendritic cells. J Virol 79:2432-2439, 2005 26. Chang TH, Liao CL, Lin YL: Flavivirus induces interferon-beta gene expression through a pathway involving RIG-I-independent IRF-3 and PI3K-dependent NF-kappaB activation. Microbes Infect 8:157-171, 2006 27. Green S, Rothman A: Immunopatholgical mechanisms in dengue and dengue hemorrhagic fever. Curr Opin Infect Dis 19:429-436, 2006 28. Navarro-Sanchez E, Despres P, Cedillo-Barron L: Innate immune responses to dengue virus. Arch Med Res 36:425-435, 2005 29. Shresta S, Kyle JL, Beatty PR, et al: Early activation of natural killer and B cells in response to primary dengue virus infection in A/J mice. Virology 319:262-273, 2004 30. Bente DA, Melkus MW, Garcia JV, et al: Dengue fever in humanised NOD/SCID mice. J Virol 79:13797-13799, 2005 31. Littaua R, Kurane I, Ennis FA: Human IgG Fc receptor II mediates antibody-dependent enhancement of dengue virus infection. J Immunol 144:3183-3186, 1990 Author's personal copy Leong et al Dengue Hemorrhagic Fever 32. Jessie K, Fong MY, Devi S, et al: Localisation of dengue virus in naturally infected human tissues, by immunohistochemistry and in situ hybridisation. J Infect Dis 189:1411-1418, 2004 33. Huang KJ, Yang YC, Lin YS, et al: The dual-specific binding of dengue virus and target cells for the antibody-dependent enhancement of dengue virus infection. J Immunol 176:2825-2832, 2006 34. Vaughn DW, Green S, Kalayanarooj S, et al: Dengue viremia titre, antibody response pattern, and virus serotype correlate with disease severity. J Infect Dis 181:2-9, 2000 35. Libraty DH, Endy TP, Houng HS, et al: Differing influences of virus burden and immune activiation on disease severity in secondary dengue-3 virus infections. J Infect Dis 185:1213-1221, 2002 36. Kliks SC, Nisalak A, Brandt WE, et al: Antibody-dependent enhancement of dengue virus growth in human monocytes as a risk factor for dengue hemorrhagic fever. Am J Trop Med Hyg 40:444451, 1989 37. Laoprasopwattana K, Libraty DH, Endy TP, et al: Dengue virus (DV) enhancing antibody activity in pre-illness plasma does not predict subsequent disease severity or viremia in secondary DV infection. J Infect Dis 192:510-519, 2005 38. Kliks SC, Nimmanitya S, Nisalak A, et al: Evidence that maternal dengue antibodies are important in the development of dengue hemorrhagic fever in infants. Am J Trop Med Hyg 38:411-419, 1988 39. Libraty DH, Young PR, Pickering D, et al: High circulating levels of the dengue virus non-structural protein NS1 early in dengue illness correlate with the development of dengue hemorrhagic fever. J Infect Dis 186:1165-1168, 2002 40. Chung KM, Nybakken GE, Thompson BS, et al: Antibodies against West Nile virus non-structural protein NS1 prevent lethal infection through Fc gamma receptor-dependent and independent mechanisms. J Virol 80:1340-1351, 2006 41. Costa SM, Paes MV, Barreto DF, et al: Protection against dengue type 2 virus induced in mice immunized with a DNA plasmid encoding the non-structural 1 (NS1) gene fused to the tissue plasminogen activator signal sequence. Vaccine 24:195-205, 2006 42. Lin CF, Lei HY, Shiau AL, et al: Antibodies from dengue patient sera cross-reacts with endothelial cells and induces damage. J Med Virol 69:82-90, 2003 43. Lin CF, Chiu SC, Hsiao YL, et al: Expression of cytokine, chemokine, and adhesion molecules during endothelial activation induced by antibodies against dengue virus non-structural protein 1. J Immunol 174:395-403, 2005 44. Alvarez M, Rodrigue-Roche R, Bernardo I, et al: Dengue hemorrhagic fever caused by sequential dengue 1-3 infections at a long interval: Havana epidemic. Am J Trop Med Hyg 75:1113-1117, 2006 45. Endy TP, Nisalak A, Chunsuttiwat S, et al: Spatial and temporal circulation of dengue virus serotypes: a prospective study of primary school children in Kamphaeng Phet, Thailand. Am J Epidemiol 56: 52-59, 2002 46. Endy TP, Nisalak A, Chunsuttitwat S, et al: Relationship of preexisting dengue virus (DV) neutralizing antibody levels to viremia and severity of disease in a prospective cohort study of DV infection in Thailand. J Infect Dis 189:990-1000, 2004 47. Mongkolsapaya J, Dejnirattisai W, Xu XN, et al: Original antigenic sin and apoptosis in the pathogenesis of dengue hemorrhagic fever. Nat Med 921-927, 2003 48. Mongkolsapaya J, Duangchinda T, Dejnirattisai W, et al: T cell responses in dengue hemorrhagic fever: are cross-reactive T cells suboptimal? J Immunol 176:3821-3829, 2006 49. Mangada MM, Rothman AL: Altered cytokine responses of denguespecific CD4⫹ T cells to heterologous serotypes. J Immunol 175: 2676-2683, 2005 50. Bashyam HS, Green S, Rothman AL: Dengue virus-reactive CD8⫹ T cell display quantitative and qualitative differences in their response to variant epitopes of heterologous viral serotypes. J Immunol 176:28172824, 2006 235 51. Page KR, Scott AL, Manabe YC: The expanding realm of heterologous immunity: friend or foe? Cell Microbiol 8:185-196, 2006 52. Mathew A, Kurane I, Green S, et al: Impaired T cell proliferation in acute dengue infection. J Immunol 162:5609-5615, 1999 53. Pichyangkul S, Endy TP, Kalayanarooj S, et al: A blunted blood plasmacytoid dendritic cell response to an acute systemic viral infection is associated with increased disease severity. J Immunol 171: 5571-5578, 2003 54. Simmons CP, Dong T, Chau NV, et al: Early T cell responses to dengue virus epitopes ion Vietnamese adults with secondary dengue virus infections. J Virol 79:5665-5675, 2005 55. Talavera D, Castillo AM, Dominguez MD, et al: IL8 release, tight junction and cytoskeleton dynamic reorganisation conducive to permeability increase are induced by dengue virus infection of microvascular endothelial monolayers. J Gen Virol 85:1801-1813, 2004 56. Dewi BE, Takasaki T, Kurane I: In vitro assessment of human endothelial cell permeability: effects of inflammatory cytokines and dengue virus infection. J Virol Methods 121:171-180, 2004 57. Avirutnan P, Punyadee N, Noisakran S, et al: Vascular leakage in severe dengue virus infections: a potential role for the non-structural viral protein NS1 and complement. J Infect Dis 193:10781088, 2006 58. Cardier JE, Marinao E, Romano E, et al: Proinflammatory factors present in sera from patients with acute dengue infection induce activation and apoptosis of human microvascular endothelial cells: possible role of TNF-␣ in endothelial cell damage in dengue. Cytokine 30:359-365, 2005 59. Shresta S, Sharar KL, Prigozhin DM, et al: Murine model for dengue virus-induced lethal disease with increased vascular permeability. J Virol 80:10208-10217, 2006 60. Boonpucknavig S, Boonpucknavig V, Bhamarapravati N, et al: Immunofluorescence study of skin rash in patients with dengue hemorrhagic fever. Arch Pathol Lab Med 103:463-466, 1979 61. Perez AB, Garcia G, Sierra B, et al: IL-10m levels in dengue patients: some findings from the exceptional epidemiological conditions in Cuba. J Med Virol 73:230-234, 2004 62. Nguyen TH, Nguyen TL, Lei HY, et al: Association between sex, nutritional status, severity of dengue hemorrhagic fever, and immune status in infants with dengue hemorrhagic fever. Am J Trop Med Hyg 72:370-374, 2005 63. Chakravarti A, Kumaria R: Circulating levels of tumor necrosis factoralpha and interferon-gamma in patients with dengue and dengue hemorrhagic fever during an outbreak. Indian J Med Res 123:25-30, 2006 64. Huang YH, Lei HY, Liu CC, et al: Tissue plasminogen activator induced by dengue virus infection of human endothelial cells. J Med Virol 70:610-616, 2003 65. Chen LC, Lei HY, Liu CC, et al: Correlation of serum levels of macrophage migration inhibitory factor with disease severity and clinical outcome in dengue patients. Am J Trop Med Hyg 74:142-147, 2006 66. Wang S, He R, Patarapotikul J, et al: Antibody-enhanced binding of dengue-2 virus to human platelets. Virology 213:254-257, 1995 67. Lin CF, Lei HY, Liu CC, et al: Generation of IgM anti-platelet autoantibody in dengue patients. J Med Virol 63:143-149, 2001 68. Medin CL, Fitzgerald KA, Rothman AL: Dengue virus non-structural protein/NS5 induces interleukin-8 transcription and secretion. J Virol 79:11053-11061, 2005 69. Pang T, Cardosa MJ, Guzman MG: Of cascades and perfect storms: the immunopathogenesis of dengue hemorrhagic fever-dengue shock syndrome (DHF/DSS). Immunol Cell Biol 85:43-45, 2007 70. Barreto DF, Takiya CM, Paes MV, et al: Histopathological aspects of Dengue-2 virus infected mice tissues and complementary virus isolation. J Submicrosc Cytol Pathol 36:121-130, 2004 71. Huerre MR, Lan NT, Marianneau P, et al: Liver histopathology and biological correlates in five cases of fatal dengue fever in Vietnamese children. Virchows Arch 438:107-115, 2001 72. Carvalho de Macedo F, Nicol AF, Cooper LD, et al: Histologic, viral, and molecular correlates of dengue fever infection of the liver using Author's personal copy 236 Seminars in Diagnostic Pathology, Vol 24, No 4, November 2007 highly sensitive immunohistochemistry. Diagn Mol Pathol 15:223228, 2006 73. Sahaphong S, Riengrojpitak S, Bhamarapravati N, et al: Electron microscopic study of the vascular endothelial cell in dengue hemorrhagic fever. Southeast Asian J Trop Med Pub Health 11:194-204, 1980 74. de la C Sierra B, Kouri G, Guzman MG: Race: a risk factor for dengue hemorrhagic fever. Arch Virol 152:533-542, 2007 75. Gubler DJ: The global pandemic of dengue/dengue hemorrhagic fever: current status and prospects for the future. Ann Acad Med Singapore 27:227-234, 1998 76. Halstead SB, Streit TG, Lfontant JG, et al: Haiti: absence of dengue hemorrhagic fever despite hyperendemic dengue virus transmission. Am J Med Hyg 65:180-183, 2001 77. Loke H, Bethell DB, Phung CX, et al: Strong HLA class-I restricted T cell responses ind engue hemorrhagic fever. A double-edged sword? J Infect Dis 184:1369-1373, 2001 78. LaFluer C, Granados J, Vargas-Alarcon G, et al: HLA-DR antigen frequencies in Mexican patients with dengue virus infections: HLA-DR4 as a possible genetic resistance factor for dengue hemorrhagic fever. Hum Immunol 63:1039-1044, 2002