Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Jatene procedure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac arrest wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
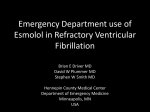
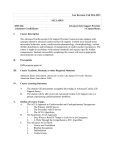
Can the block help the beat? Beta blockers for ventricular fibrillation Caleb J Stephenson, PharmD Department of Pharmacy, University Health System, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio March 6, 2015 Learning Objectives 1. 2. 3. 4. Describe the presentation and management of ventricular fibrillation (VF) Identify the potential cellular benefit of beta blockers during VF Evaluate the evidence regarding beta blockers in VF Formulate a recommendation based on the available literature I. Ventricular Fibrillation (VF) A. Introduction 1,2 1. High-frequency and asynchronous contraction of the ventricles resulting in no cardiac output or blood pressure 2. Almost always fatal i. Approximately 92% of out-of-hospital cardiac arrest die ii. Tends to deteriorate into asystole over time 3. Most common arrhythmia in cardiac arrest 4. The initial rhythm in 65-85% of cardiac arrest patients B. Epidemiology 2,3,4 1. VF accounts for approximately 100,000 deaths each year in the US 2. The incidence in the US is 0.1-0.2% C. Characteristics 5,6 1. Disorganized and totally random activation of ventricle 2. Electrical wavelet activity from multiple wandering locations Figure 1. VF conduction6 http://www.washingtonhra.com D. Presentation 1. VF patients all have similar presentations i. Hemodynamic collapse ii. Lack of blood pressure iii. Absent heart sounds iv. Apnea or agonal breathing 2. Primary vs secondary 7 i. Primary a. Independent of myocardial infarction damage ii. Secondary a. Associated with heart failure or underlying cardiac issues CJStephenson 2 Figure 2. Sinus rhythm evolving into VF on ECG 8 E. Risk Factors 4,9 1. Prior heart disease i. Myocardial infarction (13.6/1000 person-years) ii. Heart failure (21.9/1000 person-years) 2. Premature ventricular contractions 3. Coronary artery disease 4. Family history of cardiac arrest i. 2-fold increase with first degree relative II. Management 10 A. Advanced cardiac life support (ACLS) overview (see Appendix A. for algorithm) 1. Builds on basic life support (BLS) i. Activation of emergency response system ii. High quality cardiopulmonary resuscitation (CPR) iii. Early defibrillation a. First line treatment for VF and ventricular tachycardia b. Only rhythm-specific therapy proven to increase survival c. Biphasic (120-200 joules) or monophasic (360 joules) 2. ACLS team i. Leader ii. Compressions iii. Airway iv. Vitals and defibrillation v. Access and medication vi. Recorder 3. Airway management 4. Ventilation i. Bag-mask ventilation 5. Medications i. Help to facilitate and maintain spontaneous rhythm ii. Increased rates of return of spontaneous circulation (ROSC) 6. Treat reversible causes i. H & T’s CJStephenson 3 Table 1. Reversible causes of cardiac arrest Reversible cause Treatment Hypovolemia Fluids Hypoxia Ventilation (advances airway) Hydrogen ion (acidosis) Ventilation, Sodium bicarbonate IV Hypo-/hyperkalemia Potassium / Sodium bicarbonate IV, Glucose + Insulin, Calcium IV Hypothermia Warming measures Tension pneumothorax Needle decompression Tamponade Pericardiocentesis Toxins Antidote or Reversing agent Thrombosis, pulmonary Fibrinolytic treatment Thrombosis, cardiac Percutaneous Coronary Intervention (PCI) B. ACLS Medication 10 1. Epinephrine i. Endogenous catecholamine with both alpha and beta activity ii. 1 mg IV push every 3-5 minutes iii. Primary benefit is alpha receptor stimulation (vasoconstriction) a. Increase coronary and cerebral perfusion pressure b. Found to improve ROSC iv. Controversial effects with epinephrine a. Increased demand and decreased oxygen 2. Vasopressin i. Nonadrenergic peripheral vasoconstrictor a. V1 receptor activation ii. 40 units IV push for 1 dose a. To replace 1st or 2nd epinephrine dose b. No difference in outcomes verses epinephrine iii. Not affected by pH variation 3. Amiodarone i. Antiarrhythmic agent a. Potassium, sodium, and calcium channel blocker b. Alpha and beta adrenergic blocking properties ii. VF unresponsive to CPR, defibrillation, and vasopressor therapy iii. 300 mg IV push a. Repeat 150 mg if needed iv. Termination of arrhythmias are improved 4. Lidocaine i. Class Ib antiarrhythmic a. Sodium channel blocker ii. 1-1.5 mg/kg IV a. Repeat 0.5-0.75 mg/kg if needed iii. No proven short- or long-term efficacy a. Consider if amiodarone not available CJStephenson 4 III. Cardiac action potential Figure 3. Cardiac electrophysiology Phase 0 Phase 1 Phase 2 Phase 3 Phase 4 Depolarization - Rapid Na+ channels Peak-L-type Ca++ channels Plateau- Rectifier K+ channels Repolarization- Ca++ channels close Resting membrane potential http://www.cvpharmacology.com IV. Catecholamine effects on myocardium A. Catecholamines 1. Bind to G-protein coupled adrenergic receptors i. Intracellular enzyme activation a. Cardiac and/or vascular response Figure 4. Intracellular mechanism of action of catecholamines 11 CJStephenson 5 B. Positive effects 1. Essential for maintaining cardiovascular system 2. “Fight -or-flight” response 3. Life saving effects in hypotension and decreased cardiac output C. Detrimental effects 12 1. Calcium overload i. Hallmark of persistent catecholamine exposure ii. Change in mitochondrial membrane permeability iii. Sarcoplasmic reticulum dilation 2. Oxidative stress i. Hydrogen peroxide formation through catecholamine deamination ii. Superoxide anion radical formation iii. Aminochrome accumulation a. Coronary vasoconstriction 3. Mitochondrial dysfunction i. Opening of mitochondrial permeability transition pore Figure 5. Effects of sustained catecholamine exposure 12 CJStephenson 6 V. Bench Research 13 A. Mann et al used cultures of adult cardiac muscle cells to evaluate norephinephrine 1. Determining norepinephrines effects on cardiac myocytes in vitro i. Cultured cells treated with adrenergic agonist, antagonist, chelating and calcium channel blocking agents ii. Only lowest concentration producing effect reported iii. Response based on spontaneous beating Table 2. Induction of spontaneous cardiac myocyte beating Treatment Control 10-6 M norepinephrine 10-5 M dideoxyadenosine + norepinephrine 10-6 M forskolin 10-3 M dibutyryl cyclic AMP 10-3 M ethylene glycol tetraacetic acid (EGTA) + norepinephrine 10-6 M verapamil + norepinephrine 10-2 M cobalt + norepinephrine 10-5 M lidocaine + norepinephrine 10-5 M tetrodotoxin + norepinephrine 10-3 M dibutyryl cyclic AMP + 10-6 verapamil See appendix B for mechanisms Beating of myocytes (%) 0 20.9 ± 2.5 0 12.5 ± 4.1 20.5 ± 4.6 0 0 0 20.2 ± 3.4 20.8 ± 3.1 0 iv. Results a. Response blocked by removing calcium or blocking slow calcium channels 2. Effects of norepineprine on cAMP levels within stimulated cells i. Cultured cells pretreated with propranolol or normal medium ii. Stimulation with norepinephrine for 1,5,15,and 30 minutes iii. Radioimmunoassay measured cAMP Figure 6. cAMP levels with norepinephrine stimulation CJStephenson 7 iv. Results a. 4 fold increase in cAMP with norepinephrine stimulation b. Propranolol blunted cAMP elevation v. Beta blockers decrease cAMP levels, causing decreased calcium release 3. Effects of norepinephrine stimulation on calcium concentrations i. Cultured cells pretreated with propranolol, normal medium alone, or EGTA ii. Calcium concentrations measured directly with tetracarboxylate calcium indicator fura-2 a. Emission of fluorescence measured Figure 7. Calcium concentrations after norepinephrine stimulation iii. Results a. Propranolol and EGTA significantly reduced calcium concentrations iv. Beta blockers and chelating agents decrease calcium concentrations, limiting the overall effects norepinephrine VI. Animal Studies 15-17 A. Cammarata et al (2004) 1. To determine if short-acting beta1-selective blockade during CPR will improve initial and post-resuscitation survival 2. Esmolol group (n=9): 300µg/kg bolus 3. Placebo group (n=9) 4. Methods i. VF induced and left untreated for 6 minutes ii. Resuscitation a. Precordial compressions and mechanical ventilation b. Defibrillation attempted up to 3 times c. Esmolol injected 2 minutes after precordial compression into right atrium iii. ROSC: supraventricular rhythm with MAP 60 mmHg for 5 minute CJStephenson 8 5. ROSC i. Esmolol 9/9 vs placebo 5/9 (p<0.05) 6. Postresuscitation survival prolonged in esmolol group (50 vs 20 hours)(p<0.05) B. Bassiakou et al (2008) 1. Assess whether beta blockade will improve initial cardiopulmonary resuscitation success in piglets 2. Group A (n=10): placebo (saline) + epinephrine 3. Group B (n=10): atenolol + epinephrine 4. Methods i. VF was induced ii. Arrhythmia confirmed by electrocardiography and sudden drop in MAP iii. After induction of VF, mechanical ventilation was stopped and left untreated for 8 minutes iv. Resuscitation procedure a. 100% oxygen and study drugs b. Mechanical chest compressions for 2 minutes c. Defibrillation attempted after 2 minutes d. Maximum of three cycles v. End points: asystole, ROSC, or VF after 3 failed defibrillations 5. 4 animals in group A had ROSC, 9 in group B had ROSC (p< 0.05) Table 3. Different parameter before defibrillation and ROSC after defibrillation Epi + Placebo (n=10) Epi + Atenolol (n=10) SBP 2 minutes post drug administration 73 ± 11 90.5 ± 11.3 DBP 2 minutes post drug administration 32 ± 4.5 49.1 ± 6.9 CPP 19 ± 7.0 27.7 ± 5.3 ROSC 4 9 ROSC First Defibrillation 4 7 ROSC Second Defibrillation 0 2 p<0.05 p<0.05 p<0.05 p<0.05 6. Group A > group B postresuscitation heart rate (p<0.05) C. Killingsworth et al (2004) 1. Part 1: Assess the levels of myocardial interstitial catecholamines at baseline, during 8 minutes of VF, after defibrillation, and during reperfusion i. 8 mixed-breed pigs ii. Open chest with 2 microdialysis probes in lateral wall of LV iii. Catheters placed in aorta and coronary sinus (CS) iv. Interstitial fluid (ISF) from left ventricle collected v. VF induced and continued for 8 minutes vi. Defibrillation CJStephenson 9 Figure 8. ISF norepinephrine and epinephrine during 8 minutes of VF Figure 9. ISF and plasma norepinephrine and epinephrine from the aorta and CS vii. Results a. Significant increase in both norepinephrine and epinephrine during VF b. Aortic and CS levels do not correlate to ISF levels • Plasma levels peak earlier and higher • Decrease rapidly below ISF values c. Longer sustained levels in ISF (p<0.05) 2. Part 2: Determine the effects of short-acting beta blockade on catecholamine surge and survival i. Catheter placed at junction of superior vena cava and right atrium to measure coronary perfusion pressure and central venous pressure ii. 8 minutes of VF iii. External defibrillation iv. 1 mg/kg esmolol (n=8) or placebo (saline) (n=8) intravenously after defibrillation CJStephenson 10 v. ACLS performed in both groups a. Only epinephrine and dobutamine used Table 4. Resuscitation data Survival (p<0.05) Mean number of shocks Total CPR time (min) Survivor CPR time (min) Coronary perfusion pressure (mmHg) Animals requiring dobutamine Placebo (n=8) 3 10 ± 8 27 ± 15 9±8 15 ± 7 1/3 Esmolol (n=8) 7 5±4 13 ± 7 9±7 17 ± 7 2/7 vi. Esmolol improved ROSC VII. Literature Review 18-20 Nademanee K et al. Treating electrical storm: sympathetic blockade verses advanced cardiac life support-guided therapy. Circulation. 2000;102:742-747. Overview Objective To determine the efficacy of sympathetic blockade in treatment of electrical storm (ES) patients and compare their outcomes with ES patients treated according to ACLS guidelines Trial Design Retrospective observational analysis, non-randomized, non-blinded Inclusion Criteria • Recent myocardial infarct (MI) with ES. o ES: ≥20 ventricular tachycardia (VT)/VF episodes per day or ≥ 4 VT/VF episodes per hour o Recent MI: occurring within 72 hours to 3 months before the onset of ES Exclusion Criteria • Onset of MI was <72 hours • Acute pulmonary edema • Previous treatment with intravenous amiodarone • Acute respiratory failure • Acquired or congenital long QT syndrome • Recent coronary revascularization (<1 week before the onset of ES) Outcomes • Termination of ES • Determine short-term and long term effects of treatment Interventions Sympathetic blockade treatment within 1 hour after all ACLS antiarrhythmic medications were discontinued Sympathetic blockade treatments: • Left stellate ganglionic blockade o 10-20 mL 1% xylocaine injected millimeters anterior to lateral process of spine until Horner’s syndrome developed (miosis, partial ptosis) o Repeat with 10 mL 0.25% marcaine or xylocaine if needed • Esmolol 300-500 mg/kg load followed by 25-50 mg/kg/min infusion o Infusion titrated every 5-10 minutes up to 250 mg/kg/min • Propranolol 0.15 mg/kg followed by 3-5 mg dose every 6 hours • ACLS Protocol o Lidocaine 1 mg/kg IV bolus was first antiarrhythmic CJStephenson 11 Repeated once and continuous infusion started at 1-4 mg/min for persistent VF o Procainamide 100 mg bolus was given if no sinus rhythm every 5 minutes up to 500-1000 mg then 2-4 mg/min continuous infusion o Procainamide alternative was bretylium tosylate 5 mg/kg every 5 minutes up to 25 mg/kg Results • No significant differences in any variables o Baseline Characteristics Primary Outcomes Table 5. Characteristics of sympathetic blockade vs ACLS groups Characteristics Sympathetic blockade ACLS (n=22) group 2 (n=27) group 1 Age (years) 59 ± 11 56 ± 9 Men/women 23/4 19/3 Ejection Fraction (%) 31 ± 9 34 ± 6 Calcium antagonist 19 17 Beta blocker 6 3 ACE inhibitor 11 15 Onset of VF after MI 12 ± 10 11 ± 12 (days) K+ <3.5 4 3 • 1-week mortality rate, n=6 (22%) group 1 vs n=18 (82%) group 2 (p<0.0001) • Overall survival to 1 year: 67% group 1 vs 5% group 2 (p<0.0001) Figure 10. Kaplan-Meier survival cure of sympathetic blockade and ACLS group Author’s Conclusion Strengths Limitations Conclusion • Sympathetic blockade along with amiodarone improves survival of ES • • • • • • Standard ACLS vs sympathetic blockade Length of follow-up Treatment was physician preference Retrospective, Non-blinded Sample size ACLS guidelines contained lidocaine which is no longer first line CJStephenson 12 Take Home Points • • • • • Sympathetic blockade was within 1 hour after stopping antiarrhythmics Medications given during ACLS not specified for group 1 Esmolol dosing in mg not µg Sympathetic blockade had better outcomes then ACLS alone Unknown effects of sympathetic blockade without amiodarone Miwa Y et al. Effects of landiolol, an ultra-short-acting β1-selective blocker, on electrical storm refractory to class III antiarrhythmic drugs. Circulation. 2010;75:856-863. Overview Objective Evaluate the effects of landiolol on electrical storm (ES) refractory to class III antiarrhythmics Trial Design Prospective, observational Inclusion Criteria • Patient had ES o ES: sustained VT/VF twice or more per hour or 3 times or more over 6 hours o Class III antiarrhythmics administered to all patients prior to inclusion • Difficult to treat following established guidelines o CPR, electric cardioversion, antiarrhythmic drugs Exclusion Criteria • Cardiac arrest at time of arrival • Antiarrhythmic drugs before arrival • Renal failure ( SCr >2.0 mg/dL) • Hemodynamically stable VT Outcomes Inhibition of ES, survival, and discharge from hospital Interventions • Landiolol initiated at 2.5µg/kg/min; starting maintenance 10-40µg/kg/min o Effects assessed 10 minutes after administration o Titration using doubling protocol (2.5-5-10-20 etc.) o Maximum dose of 80 µg/kg/min • Severe bradycardia or hypotension in landiolol effective treatment patients o Temporal pacemaker or catecholamines were used as needed o Treatment was discontinued if landiolol treatment was difficult to maintain with supportive treatment • Inhibition of ES o Completely resolved VT/VF for 12 hours after maintenance dose administered o Oral carvedilol or bisoprolol given concomitantly at 2.5 and 1.25 mg/day for landiolol responsive patients Results Baseline • 42 patients admitted to critical care center Characteristics • All had ES and were difficult to treat following established guidelines • 60% had ischemic heart disease • 21 (50%) patients had an acute MI • Mean left ventricular ejection fraction 39 ± 15% • Killip class III and IV in 21(50%) patients • Mean APACHE II score 19 ± 10 • Number of shocks was 5 ± 13 • 17(40%) patients had assisted circulation devices Primary Outcomes • Landiolol inhibited ES in 33 (79%) patients CJStephenson 13 • 25 (60%) patients survived and were discharged • Significant differences were found between survivors and non-survivors Table 6. Significant differences between survivors and non-survivors Survivors (n=25) Non-survivors (n-17) Age (years) 60 ± 16 72 ± 11 Acute MI 8 (32%) 13 (76%) Killip class (I/II/III/IV) 16/1/0/8 4/0/2/11 APACHE II score 15 ± 9 24 ± 11 pH 7.3 ± 0.1 7.2 ± 0.2 Hypertension 16 (64%) 16 (94%) Assisted circulation device 5 (20%) 9 (53%) IABP* *Intra-aortic balloon pump P value 0.01 0.01 0.02 0.01 0.007 0.03 0.04 • • • • • Author’s Conclusion Strengths Limitations Take Home Points Mean duration of landilol treatment was 29 ± 31 hours Mean dose was 7.5 ± 12.2 µg/kg/min Landiolol reduced heart rate (HR) (p<0.0001) No changes noted in blood pressure (BP) 21(64%) patients received carvedilol and 12(36%) received bisoprolol Conclusion When class III antiarrhythmics are ineffective landiolol should be considered for possible ES refractory to antiarrhythmics. • Landiolol used after traditional standards of care failed • Initiated landiolol at very low dose • Specific reassessment period after administration • Clinical features used for evaluation • Lack of control • Differences in baseline characteristics between survivors and non-survivors • Sample size • Treatment for patients experiencing MI was only noted for 1 patient • Landiolol was effective at inhibiting ES in the majority of patients • Non-survivors had significantly different clinical feature than survivors Driver BE et al. Use of esmolol after failure or standard cardiopulmonary resuscitation to treat patients with refractory ventricular fibrillation. Resuscitation. 2014;85:1337-1341. Overview Objective To compare the outcomes of patients who received esmolol to those who did not receive esmolol during refractory ventricular fibrillation. Trial Design Retrospective observational analysis, non-randomized, non-blinded Inclusion Criteria • Initial rhythm was VF or VT • Cardiac arrest (CA) in the emergency department (ED) or had CA pre-hospital and remained in arrest upon ED arrival • Received at least 3 defibrillation attempts, 300 mg of amiodarone, and 3 mg of adrenaline Exclusion Criteria • Received esmolol before CA or after sustained ROSC Outcomes Not defined Data collected CJStephenson 14 Interventions Baseline Characteristics Patient Outcomes Author’s Conclusion Strengths Limitations • Pre-hospital and ED rhythms • Medications administered • CA management • Presence of ST-elevation myocardial infarction (STEMI) • Timing of ROSC • Patient outcomes Definitions • Temporary ROSC - non-fleeting return of restored circulation lasting more than 30 s, but less than 20 min • Sustained ROSC - 20 min of spontaneous circulation without recurrence of CA Esmolol 500 mcg/kg load followed by infusion at 0-100 mcg/kg/min Results Table 7. Characteristics of esmolol verses no esmolol Characteristics Esmolol (n=6) No esmolol (n=19) Age (yrs) 54.5 56 Male gender (%) 6 (100) 18 (94.7) Initial rhythm VF(%) 5 (83.3) 18 (94.7) Witnessed arrest (%) 5 (83.8) 16 (84.2) Bystander CPR (%) 3/4 (75) 14/18 (77.8) Time from call to EMS 7 6 arrival (min) Total pre-hospital 25 (18,29) 42 (25.5, 51) time (min)(IQR) Table 8. Patient outcomes from esmolol verses no esmolol Esmolol (n=6) No esmolol (n=19) Total ED CPR time (min) 39.5 16 Total CPR time (min) 63 57 Temporary ROSC (%) 4 (66.7) 8 (42.1) Sustained ROSC (%) 4 (66.7) 6 (31.6) STEMI (%) 3/5 (60) 1/7 (14.3) Emergency cardiac 5 (83.3) 3 (15.8) catheterization from ED (%) Survival to ICU admission (%) 4 (66.7) 6 (31.6) Therapeutic hypothermia (%) 4 (66.7) 5 (26.3) Survival to hospital discharge 3 (50) 3 (15.8) (%) Survival to discharge with 3 (50) 2 (10.5) good neurologic outcome (%) Conclusion • Prospective studies of beta-blockers in CA are warranted • Beta-blockers should be considered in patients with RVF once standard therapy has been performed • Inclusion criteria defined exact number of defibrillations and doses of medications needed • Therapeutic hypothermia and catheterization was reported • Retrospective • Sample size • Non-blinded, non-randomized CJStephenson 15 • Take Home Points • • • • Different rates of therapeutic hypothermia and catheterization between the groups Descriptive statistics Improvement in mortality was seen with esmolol although not significant The different rates of therapeutic hypothermia and catheterization may have effected the survival rate Favorable neurologic outcomes are possible with prolonged CPR VIII. Summary of evidence A. Bench research 1. Demonstrates the effects of norepinephrine on cardiac myocytes 2. Use of a beta blocker, calcium channel blocker, or calcium chelator decrease the response to norepinephrine B. Animal studies 1. Use of beta blockers improved ROSC and postresuscitation survival 2. Quantified the levels of catecholamines during VF and CPR in various compartments C. Literature 1. Beta blockers along with antiarrhythmic medication has a positive effect on ROSC in patients with prolonged or recurrent VF 2. Beta blockers alone have not been studied in the setting of VF IX. Conclusion A. Limited evidence for beta blockers in VF B. Current evidence suggests the beta blockers may benefit patient refractory to the current established guidelines. C. Recommendations 1. Beta blockers may be considered after antiarrhythmic administration and all reversible causes have been ruled out. i. After ACLS performed ii. Continued VF iii. Esmolol 500 mcg/kg followed by 25-50 mcg/kg/min CJStephenson 16 References 1. Goyal SK. (2014, Apr 29). Ventricular Fibrillation. Medscape. Retrieved January 25, 2015 from http://emedicine.medscape.com/article/158712-overview. 2. McNally B, Robb R, Mehta M, et al; Centers for Disease Control and Prevention. Out-of-hospital cardiac arrest surveillance - Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005-December 31, 2010. MMWR Surveill Summ. 2011;60(8):1-19. 3. Samie FH, Jalife J. Mechanisms underlying ventricular tachycardia and its transition to ventricular fibrillation in the structurally normal heart. Cardiovasc Res. 2001;50(2):242-50. 4. Sheldon SH, Gard JJ, Asirvatham SJ. Premature Ventricular Contractions and Non-sustained Ventricular Tachycardia: Association with Sudden Cardiac Death, Risk Stratification, and Management Strategies. Indian Pacing Electrophysiol J. 2010;10(8):357-71. 5. Rho RW, Page RL. Chapter 42. Ventricular Arrhythmias. In: Fuster V, Walsh RA, Harrington RA (eds): Hurst's The Heart, 13e. New York, McGraw-Hill, 2011. Available from: http://accessmedicine.mhmedical.com.libproxy.uthscsa.edu. Accessed January 25, 2015. 6. Keldermann RH, ten Tusscher KHWJ, Nash MP, et al. A computational study of mother rotor VF in the human ventricles. Am J Physiol Heart Circ Physiol. 2009;296:H370–H379 7. Volpi A, Cavalli A, Santoro E, et al. Incidence and prognosis of secondary ventricular fibrillation in acute myocardial infarction. Evidence for a protective effect of thrombolytic therapy. GISSI Investigators. Circulation. 1990;82(4):1279-88. 8. Mora LF, Leon AF. Chapter 128. Ventricular Arrhythmias. In: McKean SC, Ross JJ, Dressler DD, et al (eds): Principles and Practice of Hospital Medicine, New York, McGraw-Hill, 2012.Available from: http://accessmedicine.mhmedical.com.libproxy.uthscsa.edu. Accessed January 25, 2015. 9. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation. 2014;129(3):399-410. 10. Neumar RW, Otto CW, Link MS, et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S729-67 11. Gillies M, Bellomo R, Doolan L, et al. Bench-to-bedside review: Inotropic drug therapy after adult cardiac surgery -- a systematic literature review. Crit Care. 2005;9(3):266-79. 12. Liaudet L, Calderari B, Pacher P. Pathophysiological mechanisms of catecholamine and cocaine-mediated cardiotoxicity. Heart Fail Rev. 2014;19(6):815-24 13. Mann DL, Kent RL, Parsons B, et al. Adrenergic effects on the biology of the adult 14. mammalian cardiocyte. Circulation 1992;85:790-804 15. Cammarata G, Weil MH, Sun S, et al. Beta1-adrenergic blockade during cardiopulmonary resuscitation improves survival. Crit Care Med. 2004;32(9 Suppl):S440-3. 16. Bassiakou E, Xanthos T, Koudouna E, et al. Atenolol in combination with epinephrine improves the initial outcome of cardiopulmonary resuscitation in a swine model of ventricular fibrillation. Am J Emerg Med. 2008;26(5):578-84. 17. Killingsworth CR, Wei CC, Dell'Italia LJ, et al. Short-acting beta-adrenergic antagonist esmolol given at reperfusion improves survival after prolonged ventricular fibrillation. Circulation. 2004;109(20):2469-74. 18. Nademanee K, Taylor R, Bailey WE, et al. Treating electrical storm : sympathetic blockade versus advanced cardiac life support-guided therapy. Circulation. 2000;102(7):742-7. 19. Miwa Y, Ikeda T, Mera H, et al. Effects of landiolol, an ultra-short-acting beta1-selective blocker, on electrical storm refractory to class III antiarrhythmic drugs. Circ J. 2010;74(5):856-63. 20. Driver BE, Debaty G, Plummer DW, et al. Use of esmolol after failure of standard cardiopulmonary resuscitation to treat patients with refractory ventricular fibrillation. Resuscitation. 2014;85(10):1337-41. CJStephenson 17 21. Bassiakou E, Xanthos T, Papadimitriou L. The potential beneficial effects of beta adrenergic blockade in the treatment of ventricular fibrillation. Eur J Pharmacol. 2009;616(1-3):1-6. 22. de Oliveira FC, Feitosa-Filho GS, Ritt LE. Use of beta-blockers for the treatment of cardiac arrest due to ventricular fibrillation/pulseless ventricular tachycardia: A systematic review Resuscitation. 2012;83(6):674-683. 23. Surawicz B. Ventricular fibrillation. J Am Coll Cardiol. 1985;5(6 Suppl):43B-54B 24. Zaugg CE. Current concepts on ventricular fibrillation: a vicious circle of cardiomyocyte calcium overload in the initiation, maintenance, and termination of ventricular fibrillation. Indian Pacing Electrophysiol J. 2004;4(2):85-92. 25. Vassalle M, Lin CI. Calcium overload and cardiac function. J Biomed Sci. 2004;11(5):542-65. 26. Santo-Domingo J, Demaurex N. Calcium uptake mechanisms of mitochondria. Biochim Biophys Acta. 2010;1797(6-7):907-12. 27. Gustafsson AB, Gottlieb RA. Heart mitochondria: gates of life and death. Cardiovasc Res. 2008;77(2):33443. 28. Shintani-Ishida K, Yoshida K. Ischemia induces phospholamban dephosphorylation via activation of calcineurin, PKC-α, and protein phosphatase 1, thereby inducing calcium overload in reperfusion. Biochim Biophys Acta. 2011;1812(7):743-51. 29. Sejersted OM. Calcium controls cardiac function--by all means! J Physiol. 2011;589:2919-20. 30. Weiss JN, Qu Z, Chen PS, et al. The dynamics of cardiac fibrillation. Circulation. 2005;112(8):1232-40. 31. Eifling M, Razavi M, Massumi A. The evaluation and management of electrical storm. Tex Heart Inst J. 2011;38(2):111-21. 32. Eftestøl T, Wik L, Sunde K, Steen PA. Effects of cardiopulmonary resuscitation on predictors of ventricular fibrillation defibrillation success during out-of-hospital cardiac arrest. Circulation. 2004;110(1):10-5. 33. Volpi A, Cavalli A, Santoro L, et al. Incidence and prognosis of early primary ventricular fibrillation in acute myocardial infarction--results of the Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardico (GISSI-2) database. Am J Cardiol. 1998;82(3):265-71. 34. Schleifer JW, Srivathsan K. Ventricular arrhythmias: state of the art. Cardiol Clin. 2013;31(4):595-605 35. Henkel DM, Witt BJ, Gersh BJ, et al. Ventricular arrhythmias after acute myocardial infarction: a 20-year community study. Am Heart J. 2006;151(4):806-12. 36. Gheeraert PJ, De Buyzere ML, Taeymans YM, et al. Risk factors for primary ventricular fibrillation during acute myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2006;27(21):2499-510. 37. Panfilov A, Pertsov A. Ventricular fibrillation: evolution of the multiple-wavelet hypothesis. Phil. Trans. R. Soc. Lond. A. 2001:359;1315-1325 38. St John Sutton M, Lee D, Rouleau JL, et al. Left ventricular remodeling and ventricular arrhythmias after myocardial infarction. Circulation. 2003;107(20):2577-82. 39. Bourque D, Daoust R, Huard V, et al. Beta-blockers for the treatment of cardiac arrest from ventricular fibrillation? Resuscitation. 2007;75(3):434-44. 40. Altschulda RA, Billmanb GE. Beta 2-adrenoceptors and ventricular fibrillation. Pharmacol Ther. 2000:88;1– 14 41. de Oliveira MA, Brandi AC, Dos Santos CA, et al. The calcium paradox - what should we have to fear? Rev Bras Cir Cardiovasc. 2014;29(2):249-54. 42. Adameova A, Abdellatif Y, Dhalla NS. Role of the excessive amounts of circulating catecholamines and glucocorticoids in stress-induced heart disease. Can J Physiol Pharmacol. 2009;87(7):493-514. 43. Jalife J. Ventricular fibrillation: mechanisms of initiation and maintenance. Annu Rev Physiol. 2000;62:2550. CJStephenson 18 Appendix A. ACLS algorithm Appendix B. Mechanism of action Dideoxyadenosine Forskolin Dibutyryl cAMP Ethylene glycol tetraacetic acid (EGTA) Cobalt Tetrodotoxin Verapamil Adanylate cyclase inhibitor Direct action stimulates adenylate cyclase cAMP analog Chelating agent Depresses oxygen uptake by the mitochondria Block the pore of the Na+ channel Non-dihydropyridine calcium channel blocker CJStephenson 19