Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Adaptive immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Major histocompatibility complex wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
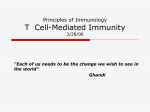
Cellular and Gene Therapy for Major Histocompatibility Complex Class II Deficiency Franck Matheux1,2 and Jean Villard1 1 Immunology and Transplant Unit, Division of Immunology and Allergology, Geneva University Hospital, 1211 Geneva 4; and 2Department of Genetics and Microbiology, Geneva Medical School, 1211 Geneva, Switzerland P rimary immunodeficiency diseases represent a heterogeneous group of inborn errors of the immune system affecting children in their first years of life. All of these syndromes are characterized by abnormalities in the development, maturation, or function of cells of the immune system. Although the phenotypes of these hereditary immunodeficiency diseases (typically characterized by an extreme susceptibility to infections) are fairly uniform, the genetic defects that are responsible are very heterogeneous. One example of primary immunodeficiency is called severe combined immunodeficiency (SCID). Blood analyses of SCID children are characterized by absence of T cells, B cells, and sometimes natural killer (NK) cells. Several genetic defects have been demonstrated to lead to the same phenotype. SCID can result from mutations in the adenosine deaminase gene, which encodes for a protein implicated in DNA synthesis and cell survival. SCID can result in defects in the Janus tyrosine kinase (Jak) 3 or in genes involved in the rearrangement of T and B cell antigen-specific receptors (the RAG 1 and RAG 2 genes). SCID can also result from a defect in the gene encoding a chain of the common receptor of several cytokines [the common J-chain (Jc) gene]. This defect is called SCID-X1 (5). Other well-known primary immunodeficiencies are characterized by a defect in antibody production. These include the X-linked agammaglobulinemia, in which mutations in the gene encoding Bruton tyrosine kinase lead to the disease. The hyper-IgM syndrome is another example of an antibody production defect, wherein the B cells are not able to switch from IgM to IgG, IgA, or IgE. The X-linked form of the disease (called HyperIgM-1) is caused by an absence of the CD40 ligand (CD40L) protein. This protein is expressed at the cell surface of the activated T cell, and the interaction between CD40L and CD40, expressed at the cell surface of the B cell, is crucial for the antibody switching in the germinal center of lymph nodes (5). Major histocompatibility complex class II (MHC II) deficiency is another primary immunodeficiency, phenotypically homogenous but genetically heterogenous, that will be described latter in more detail. Most of these syndromes are severe, and bone marrow transplantation (BMT) is currently the only therapy for curing patients with primary human immunodeficiency. Unfortunately, most patients do not have histocompatible donors and 154 News Physiol Sci 19: 154158, 2004; 10.1152/nips.01462.2003 receive alternate therapy with nonhistocompatible BMT, which has a high rate of severe complications (5). Therefore, the optimization of other therapies is necessary for children suffering from these rare genetic disorders. Transplantation of autologous hematopoietic stem cells genetically modified to express the defective gene (stem cell and gene therapy) is an alternative approach that may prove to be superior to histocompatible BMT. In 2000, the first study of gene therapy for children suffering from SCID-X1, which accounts for more than half of SCID cases, was published. As mentioned above, the SCID-X gene is caused by mutations of the gene encoding a common receptor of several cytokines (the Jc gene). The disease is very severe and is characterized by the absence of both T and NK lymphocyte subsets from the periphery. SCID-X1 represents the most suitable situation for gene therapy because in one study (1) the correction of the genetic defect relieved the block in early lymphoid development and provided a growth advantage to corrected T lymphocytes. In this study, the correction of hematopoietic cells with a wild-type Jc gene led to spectacular positive results. The T cells appear in the peripheral blood, and the immune functions were restored in most of these treated SCID-X1 patients. Unfortunately, two of them developed leukemia several months after the treatment. Insertion of the transgene in the vicinity of the LM-only (LMO-2) gene has been detected. The function of the LMO-2 protein is not clearly defined, but this protein has been previously implicated in T cell leukemia (6). These results provide the proof of concept that cellular and gene therapy is a valid alternative to treat monogenic congenital disease, particularly primary immunodeficiency. However, the two cases of leukemia clearly show that not all of the processes are completely controlled. Monitoring of the insertion site is crucial, as is the acquisition of more experience in animal models of human genetic diseases without an evident selective growth advantage for transduced cells. Our group has worked for many years on another primary immunodeficiency, MHC II deficiency, which is also a good candidate for gene therapy protocol, as discussed below. MHC II deficiency, a disease of gene regulation MHC II antigens are cell surface molecules that play a piv0886-1714/04 5.00 © 2004 Int. Union Physiol. Sci./Am. Physiol. Soc. www.nips.org Downloaded from http://physiologyonline.physiology.org/ by 10.220.32.247 on May 6, 2017 Major histocompatibility complex (MHC) class II deficiency is a primary immunodeficiency. Lentiviral vectors are used for gene therapy in a mouse model of this disease. In addition, by a direct genetic correction approach, a diagnostic test to determine which of the four MHC II genes is defective in new MHC II-deficiency patients has been optimized. FIGURE 1. Elucidation of the molecular defects responsible for major histocompatability complex class II (MHC II) deficiency has led to the identification of four essential and specific transactivators of MHC II genes. A prototypical MHC II promoter is depicted with its conserved X, X2, and Y motifs. The four transactivators affected in MHC II deficiency are highlighted. The corresponding complementation groups, the percentage of patients in each group, and the chromosomal location of the affected genes are indicated. CIITA is a highly regulated non-DNA-binding coactivator that is responsible for cell-type specificity and induction of MHC II expression. RFX5, RFXAP, and RFXANK are the three subunits of the X box-binding regulatory factor X (RFX) complex. All four genes are essential and highly specific for MHC II expression. The other promoter-binding complexes (X2BP and NF-Y) are not specific for MHC II expression and are not affected in MHC II deficiency. genes (11). The genes that are affected in all four complementation groups have been identified (Fig. 1). The gene affected in group A encodes the class II transactivator (CIITA). CIITA is a differentially expressed coactivator protein that functions as the master control factor determining the cell type specificity and inducibility of MHC II expression (11, 14). The genes affected in groups B, C, and D, encode RFXANK (8), RFX5 (13), and RFXAP (4, 16), respectively. These three proteins are subunits of regulatory factor X (RFX), a ubiquitously expressed protein complex that binds to the X box cis-acting sequence present in MHC II promoters (Fig. 1). Defects in RFX account for the majority (>80%) of all known patients. Isolation of the genes that are defective in MHC II deficiency has provided us with tools that are of obvious clinical relevance. The availability of the genes encoding CIITA, RFX5, RFXAP, and RFXANK paves the way for the development of new approaches that will improve the diagnosis and treatment of MHC II deficiency. Rationale for envisaging gene therapy for MHC II deficiency The optimal symptomatic care currently available for MHC II deficiency consists of the prophylactic use of antibiotics, intravenous administration of immunoglobulins, and parenteral nutrition. Although these treatments can reduce the frequency and severity of the clinical problems associated with MHC II deficiency, they do not prevent progressive organ dysfunction or death at a young age. As for other combined immunodeficiency disorders, allogeneic BMT is therefore currently considered to be the treatment of choice. Unfortunately, News Physiol Sci • Vol. 19 • June 2004 • www.nips.org 155 Downloaded from http://physiologyonline.physiology.org/ by 10.220.32.247 on May 6, 2017 otal role in the control of the immune response. They shape the T cell repertoire by directing positive and negative selection in the thymus, and they initiate and regulate immune responses by presenting antigenic peptides to the receptor of CD4+ T helper lymphocytes. They also participate in the activation of the antigen-presenting cells on which they are expressed. Considering these key functions, it is not surprising that expression of MHC II molecules is tightly regulated and largely restricted to professional antigen-presenting cells, thymic epithelial cells, and cells exposed to a variety of stimuli, including immune regulators such as interferon-J. Precise regulation of this expression pattern is crucial for the immune system. This is emphasized by the fact that ectopic or abnormal MHC II expression has been implicated in the pathogenesis of autoimmune diseases, whereas the lack of MHC II expression results in a severe immunodeficiency syndrome called MHC II deficiency (11). MHC II deficiency, also referred to as the bare lymphocyte syndrome, is an autosomal recessive disorder. The disease phenotype is due to the complete loss of MHC II expression in all cell types. As expected from the central role of MHC II molecules, the most striking and constant immunologic characteristics of MHC II deficiency are the absence of cellular and humoral immune responses to antigens. Patients are unable to mount T cell-mediated immune responses to antigens that the patients have been immunized with or sensitized to by infections. Humoral immunity is also severely impaired. Patients are panhypogammaglobulinemic, almost agammaglobulinemic, or have a decrease in one or two immunoglobulin isotypes. Antibody responses to immunizations and infections by microbial agents are generally absent or strongly reduced. Although patients have normal numbers of circulating T and B lymphocytes, CD4+ T cell counts are typically reduced and CD8+ T cell counts are proportionally increased. This presumably reflects abnormal selection and maturation of CD4+ T cells resulting from a lack of MHC II expression in the thymus (7, 11, 17). The major clinical manifestations of MHC II deficiency are the same as those associated with other severe immunodeficiency syndromes. These include septicemia and recurrent infections of the gastrointestinal, pulmonary, and upper respiratory or urinary tracts. The patients are prone to bacterial, fungal, viral, and protozoan infections. These infections start during the first year of life, and subsequent evolution of the disease is characterized by an inexorable progression of the infectious complications until death ensues. Few affected children reach puberty; the majority die between the age of 6 mo and 5 yr (7, 11, 17). Although the disease is a direct consequence of the lack of MHC II expression, the primary genetic defects do not lie in the MHC II genes themselves. Instead they reside in genes encoding transacting regulatory factors required for the expression of MHC II genes. These transacting factors activate transcription of MHC II genes by interacting with a highly conserved DNA segment present in the promoters of all MHC II genes (Fig. 1). Somatic cell fusion experiments performed with cell lines derived from MHC II deficiency patients have defined four different genetic complementation groups (A, B, C, and D), reflecting the existence of four distinct regulatory lentiviral vector expressing the mouse RFX5 gene. The lentiviral vector has been shown to be especially efficient to transduced hematopoietic stem cells (12). After transduction, the cells are injected via the tail vein into irradiated 6-wk-old RFX5/ mice. Following reintroduction of the transduced cells into RFX5/ mice, repopulation of these recipient mice by corrected bone marrow-derived stem cells is analyzed by examining cell surface MHC II expression in key cell types (B cells, dendritic cells, macrophages). The restoration of a functional immune system in the recipient mice is evaluated by analyzing their ability to mount B and T cell-dependent immune responses (specific T cell activation, production of antibodies, etc.) (Fig. 2). Genetic correction of pluripotent stem cells is one of the critical steps in gene therapy, because only these cells can initiate long-term reconstitution of the entire hematopoietic system. The phenotype of pluripotent stem cells is defined by several cell surface markers but mainly by the capacity of a few of them to reconstitute all hematopoietic lineages for the long term. Different options are possible to get pluripotent stem cells from the bone marrow, which is obtained by flushing tibial and femoral bones of donor mice. Pretreatment of the donor mice with 5’-fluorouracil is well known to enrich early progenitors of the bone marrow. Another approach is to select hematopoietic progenitors from the bone marrow. The purification of progenitors from the bone marrow of the RFX5/ mice can be obtained by cell sorting with a fluorescence-activated cell sorter (FACS) after the cells are labeled with the fluorescent markers of interest for hematopoietic stem cells. The Sca1+ protein is one of these interesting cell surface markers. It is expressed at the surface of bone marrow stem cells but also at the cell surface of more differentiated cells and in some mature bone marrow-derived cells. The selection and isolation of Sca1+ cells from bone marrow match as closely as possible the conditions currently used in the human Cellular and gene therapy in a mouse model of MHC II deficiency In contrast to CIITA, which is tightly regulated, the RFX5 gene is expressed in every cell type that has been tested. Potential problems related to ectopic transgene expression have to be avoided in the context of gene therapy. It was therefore logical to choose the RFX5 knockout (RFX5/) mouse as a model system to develop gene therapy for MHC II deficiency (3). In MHC II deficiency, the key cellular compartments in which MHC II expression should be restored by gene therapy are bone marrow-derived antigen-presenting cells including dendritic cells, B cells, and macrophages. To achieve this in the RFX5/ mouse, we are using an ex vivo approach similar to those that have been successful in other mouse immunodeficiency models, such as those for Jak3 deficiency, RAG-2 deficiency, Jc deficiency, or E-thalassemia. In the RFX5/ mouse model, bone marrow cells are isolated from a RFX5/ donor mouse. These cells are transduced ex vivo with the supernatant of a retroviral vector that contains the mouse wild-type RFX5 gene. For this model, the retroviral vector is a 156 News Physiol Sci • Vol. 19 • June 2004 • www.nips.org FIGURE 2. Experimental procedure for cellular and gene therapy in a mouse model of MHC II deficiency. RFX5/ bone marrow stem cells are enriched with 5’-fluorouracil (5-FU) or purified by cell sorting [fluorescence-activated cell sorter (FACS) analysis]. The cells are then transduced with a lentiviral vector that contains the mouse RFX5 gene in the presence of cytokines such as interleukin (IL)-1D, IL-3, stem cell factor (SCF), or thrombopoietin (TPO) for a few hours. The transduced cells are then reinfused in lethally irradiated RFX5/ mice to reconstitute all hematopoietic lineages. MHC II expression and immune function and are analyzed after bone marrow reconstitution. Downloaded from http://physiologyonline.physiology.org/ by 10.220.32.247 on May 6, 2017 the success rate of BMT for MHC II deficiency remains lower than in other immunodeficiency syndromes. This does not appear to be typical for MHC II-deficient patients. Instead, it is likely due to other criteria such as diagnosis at a late age. The two main obstacles are intractable persistent viral infections and graft failure or rejection. The difficulty of finding allogeneic and human leukocyte antigen (HLA)-compatible donors also represents a major problem (7). Given the poor success rate of BMT for MHC II deficiency, the development of an alternative curative therapy represents a major goal. Now that four genes affected in MHC II deficiency have been identified, treatment by cellular and gene therapy of all four complementation groups can be envisaged. Approaches relying on introduction of the wild-type CIITA, RFX5, RFXANK, or RFXAP genes into hematopoietic stem cells from patients in complementation group A, B, C, or D, respectively, would represent a logical therapeutic strategy. The validity and strength of this type of approach has recently been emphasized by its resounding success in curing SCID-X1 infants carrying mutations in the Jc gene (1). In addition, many features render MHC II deficiency an excellent candidate disease for the development of somatic gene therapy. First, thanks to the isolation of all four affected genes, the molecular genetics of the disease is very well defined. Second, the genes implicated in the majority of patients (RFXAP, RFXANK, and RFX5) are constitutively expressed. Third, RFX5- and CIITAdeficient mice are available and both represent excellent animal models for the human disease (2, 3). They reproduce all of the major features typical of MHC II deficiency, including a severely disturbed pattern of MHC II expression and a profound deficiency in CD4+ T cell-dependent immune responses. Fourth, pluripotent hematopoietic stem cells are the relevant target cells that need to be corrected: the ability of BMT to cure the disease has demonstrated that the correction of non-bone-marrow-derived cells, such as thymic epithelial cells, is not essential. of the reporter molecule (GFP) by FACS in >50% of the transduced cells has been observed (Fig. 3A). Subsequently, the lentiviral vectors encoding CIITA, RFXANK, RFX5, and RFXAP have been used to correct primary cells derived from MHC IIdeficiency patients (Fig. 3B). This approach permits the classification of several new MHC II-deficiency patients. Representative data for a group D patient is shown in Fig. 3. PBL from this patient were cultured and transduced with lentiviral vectors containing the four genes. After 7 days of culture, 48% of the cells were MHC II positive in the RFXAP well only (Fig. 3B) (9). The direct genetic correction is a novel diagnostic tool that could certainly be extended to other primary immunodeficiencies or to other disorders characterized by a genetic heterogeneity. Conclusions Direct genetic correction for diagnosis and molecular characterization of MHC II deficiency However, the correction of a genetic defect can also be useful for other purposes than gene therapy. The hallmark of MHC II deficiency is the absence of MHC II molecules on the surface of all cells, and the demonstration of this lack of expression currently remains the mainstay of diagnosis. However, this approach does not identify the precise genetic defect that is responsible for the absence of MHC II expression. Until now, classification of the patients into the genetic complementation groups has been done by isolating stable cell lines from the patients and performing tedious and time-consuming cell fusion experiments. In addition, the availability of a simple and rapid approach for determining which regulatory genes are affected in newly identified patients will be a crucial step for the success of cellular and gene therapy in this disease. Now that the genes affected in all four complementation groups have been identified, a rapid and straightforward approach relying on direct correction of the genetic defect has been developed. We have set up a system in which cells derived from newly identified MHC II-deficiency patients are transduced with lentiviral vectors expressing the four regulatory genes (CIITA, RFXANK, RFX5, or RFXAP). This has been done with readily accessible cell types, such as peripheral blood lymphocytes (PBL). Complementation of the genetic defect in the transduced cells can be scored very simply by FACS analysis of cell surface MHC II expression a few days after transduction of the cells. The procedure is thus designed to provide a very reliable, rapid, and simple means of determining which of the four regulatory genes is defective. Transduction and gene delivery with lentiviral vectors encoding CIITA, RFXANK, RFX5, and RFXAP were first optimized to restore MHC II expression in cell lines established from patients having defects in the corresponding genes (complementation groups, A, B, C, and D, respectively) (9, 10, 18). Once the system had been optimized with cell lines, experiments were initiated with primary cell isolates (PBL). Since MHC II deficiency patients are rare and not always readily available, the transduction efficacy of primary cells isolated from healthy individuals can be first evaluated with green fluorescent protein (GFP) lentiviral vectors. A strong expression MHC II deficiency, like other primary immunodeficiencies, FIGURE 3. Complementation of peripheral blood lymphocytes (PBL) from an MHC II-deficiency patient in complementation group D. A: efficient transduction of PBL with lentiviral vectors. PBL from a normal donor or from a patient were transduced with a control lentiviral vector encoding green fluorescenct protein (GFP). Expression of GFP was analyzed by FACS. Open profiles, untransduced cells; closed profiles, transduced cells. B: PBL are complemented by the RFXAP vector. PBL from the patient were transduced with the four lentiviral vectors. The RFXAP vector restores cell surface MHC II expression on 48% of the cells. Open profiles, untransduced cells from the patient; closed profiles, transduced cells; shaded profile, PBL from a wildtype donor. HLA DR, human leukocyte antigen class II. News Physiol Sci • Vol. 19 • June 2004 • www.nips.org 157 Downloaded from http://physiologyonline.physiology.org/ by 10.220.32.247 on May 6, 2017 setting, because no 5’-Fu can be used before bone marrow harvesting and Sca1+ purification is a procedure partially comparable with CD34+ human bone marrow purification. In addition, the reconstitution of all bone marrow lineages (especially mature T lymphocytes) is faster with Sca1+ cells compared with the reconstitution with more highly purified stem cells. Finally, highly purified transduced murine bone marrow progenitors (defined by the surface markers Sca1+c-Kit+Lin expressed by bone marrow stem cells ) are able to reconstitute normal, multilineage specification (15) with very few cells. This is certainly the best option for ex vivo gene therapy approaches. The transduction of these cells with vectors that contain the wild-type gene is the only way to obtain long-term expression of the transgene and prolonged the correction of the defect. References 1. Cavazzana-Calvo M, Hacein-Bey S, de Saint Basile G, Gross F, Yvon E, Nusbaum P, Selz F, Hue C, Certain S, Casanova JL, Bousso P, Deist FL, and Fischer A. Gene therapy of human severe combined immunodeficiency (SCID)-X1 disease. Science 288: 669672, 2000. 2. Chang CH, Guerder S, Hong SC, van Ewijk W, and Flavell RA. Mice lacking the MHC class II transactivator (CIITA) show tissue-specific impairment of MHC class II expression. Immunity 4: 167178, 1996. 3. Clausen B, Waldburger J, Schwenk F, Barras E, Mach B, Rajewski K, Förster I, and Reith W. Residual MHC class II expression on mature dendritic cells and activated B cells in RFX5-deficient mice. Immunity 8: 143155, 1998. 4. Durand B, Sperisen P, Emery P, Barras E, Zufferey M, Mach B, and Reith W. RFXAP, a novel subunit of the RFX DNA binding complex is mutated in MHC class II deficiency. EMBO J 16: 10451055, 1997. 5. Fischer A. Primary immunodeficiency diseases: an experimental model for molecular medicine. Lancet 357: 18631869, 2001. 158 News Physiol Sci • Vol. 19 • June 2004 • www.nips.org 6. Hacein BA, von Kalle C, Schmidt M, Le Deist F, Wulffraat N, McIntyre E, Radford I, Villeval JL, Fraser CC, Cavazzana-Calvo M, and Fischer A. A serious adverse event after successful gene therapy for X-linked severe combined immunodeficiency. N Engl J Med 348: 255256, 2003. 7. Klein C, Cavazzana-Calvo M, Le Deist F, Jabado N, Benkerrou M, Blanche S, Lisowska-Grospierre B, and Griscelli C. Bone marrow transplantation in major histocompatibility complex class II deficiency: a single-center study of 19 patients. Blood 85: 580587, 1995. 8. Masternak K, Barras E, Zufferey M, Conrad B, Corthals G, Aebersold R, Sanchez JC, Hochstrasser DF, Mach B, and Reith W. A gene encoding a novel RFX-associated transactivator is mutated in the majority of MHC class II deficiency patients. Nat Genet 20: 273277, 1998. 9. Matheux F, Ikinciogullari A, Zapata DA, Barras E, Zufferey M, Dogu F, Regueiro JR, Reith W, and Villard J. Direct genetic correction as a new method for diagnosis and molecular characterization of MHC class II deficiency. Mol Ther 6: 824829, 2002. 10. Peretti M, Villard J, Barras E, Zufferey M, and Reith W. Expression of the three human major histocompatibility complex class II isotypes exhibits a differential dependence on the transcription factor RFXAP. Mol Cell Biol 21: 56995709, 2001. 11. Reith W and Mach B. The bare lymphocyte syndrome and the regulation of MHC expression. Annu Rev Immunol 19: 331373, 2001. 12. Salmon P, Kindler V, Ducrey O, Chapuis B, Zubler RH, and Trono D. High-level transgene expression in human hematopoietic progenitors and differentiated blood lineages after transduction with improved lentiviral vectors. Blood 96: 33923398, 2000. 13. Steimle V, Durand B, Barras E, Zufferey M, Hadam MR, Mach B, and Reith W. A novel DNA binding regulatory factor is mutated in primary MHC class II deficiency (bare lymphocyte syndrome). Genes Dev 9: 1021 1032, 1995. 14. Steimle V, Otten LA, Zufferey M, and Mach B. Complementation cloning of an MHC class II transactivator mutated in hereditary MHC class II deficiency (or bare lymphocyte syndrome). Cell 75: 135146, 1993. 15. Uchida N, Tsukamoto A, He D, Friera AM, Scollay R, and Weissman IL. High doses of purified stem cells cause early hematopoietic recovery in syngeneic and allogeneic hosts. J Clin Invest 101: 961966, 1998. 16. Villard J, Lisowska-Grospierre B, Van den Elsen P, Fischer A, Reith W, and Mach B. Mutation of RFXAP, a regulator of MHC class II genes, in primary MHC class II deficiency. N Engl J Med 337: 748753, 1997. 17. Villard J, Masternak K, Lisowska-Grospierre B, Fischer A, and Reith W. MHC class II deficiency: a disease of gene regulation. Medicine (Baltimore) 80: 405418, 2001. 18. Villard J, Peretti M, Masternak K, Barras E, Caretti G, Mantovani R, and Reith W. A functionally essential domain of RFX5 mediates activation of major histocompatibility complex class II promoters by promoting cooperative binding between RFX and NF-Y. Mol Cell Biol 20: 33643376, 2001. Downloaded from http://physiologyonline.physiology.org/ by 10.220.32.247 on May 6, 2017 is a good model for molecular medicine studies because the disorder represents simple models that can be used in the future for more complex multifactorial diseases such as autoimmune diseases, allergy, and many other diseases. Although disease manifestations cannot in all cases be explained by single molecular events, their analysis shows that a constant interplay between clinical and basic immunology can bring about fruitful results of mutual benefit. Following the successful treatment of X-linked SCID, and despite the dramatic complications for two patients, cellular gene therapy remains a promising strategy, and encouraging results have been demonstrated both in vitro and in vivo. Several obstacles remain to be overcome, such as the level of expression of the transgene and the site of integration. Several strategies are being applied to improve these problems. The proof of concept that cellular and gene therapy can be a valid alternative for untreatable human diseases has been demonstrated. Animal models that closely mimic human diseases represent an invaluable tool and one of the key steps of the approach. The principle of gene therapy is the correction of a genetic defect. This approach can also be used as a very useful tool for the diagnosis of heterogeneous human genetic diseases.