Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Atrial fibrillation wikipedia , lookup
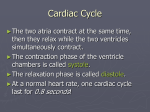
Hind Leys Biology F211 Transport in animals 5.4 Control of the cardiac cycle Objectives Describe how heart action is coordinated with reference to the sinoatrial node, the atrioventricular node and the Purkyne tissue. Interpret and explain the electrocardiogram (ECG) traces with reference to normal and abnormal heart activity. Coordination of contraction Cardiac muscle is unique in that it can initiate its own contraction. Heart muscle is described as myogenic. This means that the muscle will contract and relax rhythmically even if it is not connected to the body. The muscles from the atria and ventricles each have their own natural frequency of contraction. The atrial muscle tends to contract at a higher frequency than the ventricular muscle. The property of the muscle could cause inefficient pumping (a condition known as fibrillation) if the contractions of the chambers are not synchronised. So the heart needs a mechanism that can coordinate the contractions of all four chambers. Initiation of heartbeat At the top of the right atrium, near the vena cava, is the sinoatrial node (SAN) (1). This is a small patch of tissue that generates electrical activity, and is known as the heart’s pacemaker. The SAN initiates a wave of excitation at regular intervals. In a human, this occurs between 55-80 times a minute. Contraction of the atria The wave of contraction quickly spreads over the walls of both atria, travelling along the membranes of the muscle tissue. As the wave of excitation passes, it causes the cardiac muscle cells to contract. This is atrial systole. At the base of the atria is a disc of non-conducting tissue which prevents the wave of excitation passing directly to the ventricles. At the top of the septum is another node, the atrioventricular node (AVN) (2). This is the only route through the non-conducting tissue. The wave of excitation is delayed in the node. This allows time for the atria to finish contracting and for blood to flow into the ventricles before they begin to contract. Figure 1 The wave of contraction over the heart. 1 Hind Leys Biology F211 Transport in animals 5.4 http://www.pennmedicine.org/encyclopedia/em_DisplayAnimation.aspx?gcid=000001&ptid=57 cardiac conduction system Contraction of the ventricles Following this delay, the wave excitation is carried away from the AVN and down specialised conducting tissue called the Purkyne/Purkinje tissue. These form the bundle of His, (3) which runs down the interventricular septum. At the base of the septum the wave of excitation spreads outwards and upwards causing the ventricles to contract. This means that the ventricles contract from the base upwards, pushing blood up to the major arteries at the top of the heart. It is the pattern of electrical conduction or electrical wave that is picked up on the electrocardiogram or the ECG; the tracing of the heart's electrical activity. Electrocardiograms During an ECG a number of sensors are attached to the skin of the thorax. Some of the electrical activity generated by the heart spreads through the tissues and onwards to the skin. The sensors pick up the electrical excitation and convert this to a trace. The trace of a healthy person has a particular shape. It consists of a series of waves, labelled P, Q, R, S and T. The events these represent are shown in Figure 2. Figure 2 The events represented by an ECG trace, together with a normal trace and some abnormal traces. The shape of an ECG trace can sometimes indicate when part of the heart muscle is not healthy. It can show if the heart is beating irregularly (arrhythmia), if it is in fibrillation (the heartbeat is not coordinated), or if it has suffered a heart attack (myocardial 2 Hind Leys Biology F211 Transport in animals 5.4 infarction). ECG traces can also show if the heart has enlarged or if the Purkinje fibres are not conducting properly. Regular evenly spaced trace Irregular distances between waves. No obvious P-wave. Ventricular hypertrophy (increase in muscle thickness) Deep S-wave Figure 3 Comparison of normal and abnormal ECG traces 1. 2. 3. 4. 5. a) Explain why the SAN is called the pacemaker. Explain why atrial fibrillation decreases the efficiency of the heart. Explain why the ventricles contract from the apex upwards. Explain why the QRS complex has a larger peak than the P-wave. Each one of the figures represents an ECG pattern displaying three types of abnormal rhythms: tachycardia, bradycardia, and arrhymthmia. Identify each. b) c) 3 Hind Leys Biology F211 Transport in animals 5.4 6. The features of the heart ensure that blood is pumped efficiently and in the right direction. Explain how each of the following is important, referring to the advantages of each. a) The spread of electrical activity across the atria from the SAN. The muscles of the atria contract rom the top downwards. This pushes blood down through the AV valves in to the ventricles. b) The insulating fibrous tissue between the atria and the ventricles. This stops the wave of atrial muscle contraction continuing through to the ventricles. If contractions started at the top of the ventricles blood would just be forced towards the bottom of the heart. c) The short delay in the transmission of electrical activity through the AVN. The delay allows the atria to complete contraction and empty blood into the ventricles before they then contract. d) Passing impulses down the bundle of His to the lower end of the heart. This makes the muscles contract from the bottom of the ventricles so that eh blood is forced upwards towards the arteries. e) The rapid spread of the impulses through the fibres to the muscles of the ventricles. The contraction of the muscles spreads quickly up the ventricles. Pressure builds up rapidly and the blood is forced out at speed Artificial pacemakers The natural conducting systems of the heart (SAN, AVN and bundle of His) can become damaged by disease or ageing. As a result the coordination of the heartbeat can be disrupted- known as a heart block. An artificial pacemaker overcomes this by generating electrical impulses and conducting them to the heart muscle. This stimulates contraction of the heart chambers. Pacemakers consist of a pulse generator and one or two electrodes. It is powered by a lithium battery. Modern pacemakers can sense changes in the body, e.g. exercise, and adjust the heart rate accordingly. http://www.pennmedicine.org/health_info/animationplayer/ loads of animations This work can be reinforced using pages 70-72 of your textbook. 4