Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Circulatory system wikipedia , lookup
Inflammation wikipedia , lookup
Microneurography wikipedia , lookup
Electromyography wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Haemodynamic response wikipedia , lookup
Proprioception wikipedia , lookup
Human vestigiality wikipedia , lookup
Muscle contraction wikipedia , lookup
Neurobiological effects of physical exercise wikipedia , lookup
Basal metabolic rate wikipedia , lookup
Weight training wikipedia , lookup
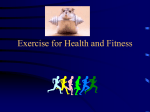
Exercise Physiology Cardiovascular System Cardiovascular Fitness The Science of Resistance Training Designing Your Clients Workouts for Maximum Muscle Hypertrophy 1 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 The Cardiovascular System The cardiovascular system is comprised of blood, blood vessels and the heart. Blood and blood vessels distribute oxygen and nutrients to the cells, carry carbon dioxide and waste products from the cells, help to regulate body temperature and prevent serious blood loss following injury through the formation of clots. The heart is at the center of the cardiovascular system (see Figure 1). It is approximately the size of a closed fist and is located behind the sternum, between the lungs. The heart is divided into four chambers that receive circulating blood: the two upper chambers are the right atrium and the left atrium the two lower chambers are the right and left ventricles. Figure 1 2 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 When the heart contracts, blood accumulates in the right atrium. When the heart relaxes, blood flows from the right atrium into the right ventricle and continues on, into the pulmonary trunk. The pulmonary trunk consists of right and left pulmonary arteries. The pulmonary arteries transport blood to the lungs, where carbon dioxide is expelled and oxygen is brought into the body. The newly oxygenated blood returns to the heart via four pulmonary veins. These veins empty the blood into the left atrium. From the left atrium the blood passes into the left ventricle. The blood is then pumped into the ascending aorta and distributed throughout the body by several large arteries. Control of Heart Rate Like skeletal muscle, cardiac muscle is striated but has the unique ability to rhythmically contract on its own, in the absence of nerve stimulation. Under normal conditions, heart rate is controlled by both the sympathetic and parasympathetic nervous systems and by certain hormones. In resting conditions, the parasympathetic system predominates. Normal resting heart rate varies between 60 and 85 beats per minute. Extended periods of endurance training (months to years) can decrease resting heart rate to 35 beats per minute or lower. It is postulated that this lower resting heart rate is the result of increased parasympathetic stimulation through the vagus nerve, with the reduction in sympathetic activity serving a lesser role. Cardiac Output Cardiac output refers to the amount of blood pumped out by each ventricle in one minute. The amount is determined by heart rate and stroke volume. Stroke volume is the volume of blood pumped out by a ventricle with each heartbeat. In general, stroke volume increases as the force of ventricular contraction increases. The normal adult blood supply is five liters and the entire blood supply passes through the body each minute. Cardiac output varies with the demands of the body, rising when the heart rate increases and dropping when the heart rate decreases. Cardiac Output During Exercise Blood flow increases in proportion to the intensity of exercise but the blood flow patterns change rather markedly. Blood is redirected, away from areas where it is not essential, to areas that are active during the exercise. Only 15 to 20 percent of resting cardiac output goes to muscle. During exhaustive exercise, muscle receives 80 to 85 percent of cardiac output. This shift is accomplished, primarily, by a decrease in blood flow to other areas of the body. When progressing from a resting state to steady rate exercise, cardiac output first increases rapidly, followed by a gradual rise, until it reaches a plateau. At this point, blood flow is sufficient to meet the metabolic requirements of exercise. Along with the shift in blood flow, several other adaptations occur. Resting heart rate decreases, due to an increase in the interior dimensions of the ventricles. Since the ventricles can fill with more blood during the relaxation phase, resting stroke volume also increases. This is beneficial to the heart, allowing it to achieve the necessary oxygen delivery with fewer beats per minute. Aerobic Capacity The complete capacity to consume oxygen at the cellular level is called maximal oxygen consumption or V0 2 max. VO2 max is regarded as the best single measurement of cardiorespiratory endurance and aerobic fitness. Since individual needs for energy are influenced by body size, age and level of fitness, V02 max is frequently expressed relative to body weight (in milliliters of oxygen per kilogram body weight per minute - ml/kg/min). The resting VO2 of 3.5 ml/kg/min is often referred to as one metabolic equivalent or I MET. To determine the MET value of any activity, multiply the MET. 3 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 value by. 3.5. When physicians prescribe cardiovascular exercise for cardiac rehabilitation, they may express the activity in METS, so a basic understanding is of benefit to the Fitness Professional. Oxygen debt refers to the difference between the volume of oxygen consumed during recovery from exercise and that consumed at rest. A quick sprint can leave you with a rapid pulse and shortness of breath. After several minutes of recovery, breathing and pulse appear to return to normal. Such post exercise oxygen consumption is needed to remove carbon dioxide that has accumulated in the body tissues and to pay the oxygen debt. There is also an oxygen debt associated with low intensity exercise. The reason is that oxygen consumption requires several minutes to reach the steady state level, even though the oxygen required to perform the exercise is constant from the very start of the exercise. The period during which oxygen consumption is below the needed level is referred to as the oxygen deficit. It is calculated as the difference between the amount of oxygen required and the amount that is actually consumed. Another measurement of aerobic capacity is the anaerobic or lactate threshold. The lactate threshold is defined as the point of increased exercise intensity at which the body starts to accumulate blood lactate. This measurement provides a means for gauging the severity of the exercise, relative to the client's physiological limits. The lactate threshold occurs at approximately 65 to 90 percent of V02 max. Aerobic Energy The body needs a constant supply of energy to function. The two primary sources of energy for the body are the aerobic and anaerobic systems. The literal definition of aerobic is "with oxygen" therefore, aerobic energy is energy produced in the presence of oxygen. Oxygen is delivered to working muscles (such as the heart, brain and skeletal muscles) through the heart, the lungs and cardiovascular system. Oxygen-depleted blood is carried back to the heart, through the veins. Once the blood reaches the heart, it is supplied with oxygen and is then re-circulated through the body. Water and carbon dioxide (CO2) are considered the "waste products" of the aerobic system. They are both eliminated through breathing and sweating, in order to allow the body to continue working. As long as the demand for oxygen does not exceed the body's ability to replace it and to release its waste products, the system will function aerobically. So, we are in an aerobic state, whether we are reading, eating or sleeping, because our body is able to provide the needed oxygen through regular inhaling and exhaling. The aerobic system uses fats and carbohydrates to produce energy. Fat is the body's primary source of energy during aerobic training because fat can be stored indefinitely. For this reason, fat tissue is capable of providing the body with a continual supply of energy. On the other hand, the body is not able to store carbohydrates efficiently, therefore we rely predominantly on our fat stores for aerobic energy. The good news is that you are burning fat when you are simply sitting or sleeping. However, because the muscles aren't working very hard, the body will utilize only a small amount of its fat stores. When the body is in a resting state, it burns approximately one. calorie of fat per minute. As one pound of fat contains 3500 calories, it is easy to see why sitting is not an effective means of losing fat. Yet, sitting is still considered an aerobic state, when the body is predominantly burning fat. To use more fat calories, yet remain in an aerobic state (i.e., continuing to utilize fat as the primary source of energy), we must increase the speed at which our muscles are working. This increases the body's demand for oxygen, which consequently bums more fat. As 4 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 long as we can meet the demand for oxygen and continue to expel its by-products (CO2 and H20), we are in the aerobic state. When working with clients who want to lose body fat, the Fitness Professional should emphasize the importance of slowly increasing the client's cardiorespiratory intensity until the body arrives at its last, true "steady aerobic state." An individual's last true "steady state" occurs during cardiorespiratory activity when any increase in the activity would result in the body's inability to supply sufficient oxygen to the working muscles. When this limit is exceeded, the body turns to an alternative energy system, to attempt to meet the energy demands. This alternative system is only able to provide energy for a short period of time because it utilizes only carbohydrates for energy and is not able to rid waste products quickly. At this point the body is crossing the anaerobic threshold. The point just prior to traversing the anaerobic threshold is the body's last true "steady state." It is possible for the body to remain in this state for a long period of time. Summary 1. Functions of the cardiovascular system are : (1) transport of oxygen tissues and removal of wastes, (2) transport of nutrients to tissues, and (3) the regulation of body temperature. 2. The heart is two pumps in one. The right side of the heart pumps blood Trough the pulmonary circulation (lungs/heart) while the left side of the heart delivers blood to the systemic (body) circulation. 3. Oxygen delivery to exercising skeletal muscle increases due to: (1) increased cardiac output, and (2) redistribution of blood flow from inactive organs to the contracting skeletal muscles. 4. Changes in heart rate and blood pressure that occur during exercise are a function of the type and intensity of exercise performed, the duration of exercise and environmental conditions. Cardiorespiratory Fitness Cardiovascular and cardiorespiratory fitness are synonyms, however, cardiorespiratory fitness is the term used in most current textbooks. It is the term that that best describes the health and function of the heart, lungs and circulatory system. 5 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Benefits of Cardiorespiratory Fitness The many benefits of cardiorespiratory fitness occur as a physiological response to aerobic training. (See Table 1) Table 1 R E P OR T E D B E N E F IT S OF C A R D I OR E S P I R A T OR Y F IT N E S S Cardiovascular Health Benefits Adaptive Physiologic Response Reduction in blood pressure Decreased resting heart rate Increased HDL-cholesterol Increased heart volume Decreased total cholesterol Increased resting and maximum stroke volume Decreased body fat stores Increased maximum cardiac output Increased aerobic work capacity Increased maximum oxygen consumption Decreased clinical symptoms of anxiety, tension and depression Increased capillary density and blood flow to active muscles Reduction in glucose-stimulated insulin secretion Increased total blood volume Increased heart function Increased maximal ventilation Possible reduction in mortality in post myocardial infarction patients Increased lung diffusion capacity Increased mobilization and utilization of fat Aerobic exercise has been effective in clinical therapies such as diabetic treatment therapy, prenatal/postpartum, renal dialysis conditioning, sleep disorder treatment and cardiac and pulmonary rehabilitation. The Fitness Professional should refer clients to available clinical rehabilitation programs for help in these areas. Cardiorespiratory Fitness In Athletes Improving cardiorespiratory fitness (conditioning and health of the heart, lungs and circulatory system) contributes to the progress of nearly all sports and conditioning programs. Improved cardiorespiratory fitness increases stamina, which lessens both fatigue and risk for certain types of injuries. As one the five components necessary for altering body composition, aerobic exercise is an important tool for body fat reduction. 6 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Components of a Cardiorespiratory (Aerobic) Exercise Program Regardless of the client's goal, there are basic components of a cardiorespiratory program that the Fitness Professional must employ: 1. Warm-up and cool-down 2. Activity criteria: mode, intensity, frequency, duration 3. Supportive conditioning: strength training and flexibility 4. Client's goal 5. Progression plan 6. Safety Warm-up and Cool-down The purpose of proper warm-up is to gradually increase heart rate, blood pressure, oxygen consumption, dilation of blood vessels, elasticity and heat of the active muscles. The primary components of the warm-up are: 1. Graduated warm-up of the activity itself. For example, if running is the chosen exercise, walk first then proceed to a slow jog. Maintain this low level aerobic activity for five to eight minutes. 2. Stretching should follow the brief activity warm-up because warm muscle is more easily stretched. The muscles used in the primary conditioning activity should be stretched. Further, these muscles should be stretched in a manner that mimics the biomechanical movements of the primary activity. 3. After stretching, continue the warm-up by graduating to the proper training intensity. The duration of the warm-up depends on the primary activity, as well as the level and intensity of the activity and the client's level of fitness. The purpose of the cool-down is to slowly decrease cardiac work.(heart rate). Low level aerobic exercise that is similar to the training activity is recommended. For instance, after running, move to a slow jog and then to a walk. Cool-down helps prevent blood-pooling in the veins, which can lead to dizziness and fainting. It also ensures adequate circulation to the skeletal muscles, heart and brain. Cooldown is critical for high cardiovascular risk clients. The length of the cool-down phase is proportional to the intensity and length of the cardiorespiratory workout. A 30-to-40 minute workout at 70 percent of maximum heart rate would warrant a 5 to 10 minute cool-down. Activity Criteria / Cardiorespiratory Exercise The following criteria are for improvements in cardiorespiratory fitness and will contribute to body fat reduction. For specific cardiorespiratory activity guidelines, directly related to continuous body fat reduction, see Altering Body Composition section. 7 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Exercise Mode Selecting an exercise mode for a client should be based on their goals, functional capacity, interests, available equipment and time constraints. Any activity that continuously employs larger muscle groups, is rhythmic and cardiorespiratory in nature, can be used. Table 2 lists some different exercise modes. Though some of the activities may be part-time anaerobic (e.g., soccer), they all contribute to cardiorespiratory fitness. Table 2 • walking (all speeds) • treadmill (all levels) • stairmaster • outdoor bicycling • stationary bike • spinning • versa-climber • • • • • • • sprinting jogging (indoor/outdoor) basketball aerobic classes swimming rower any different, fast, continuous, moving sports activity Exercise Intensity When beginning an exercise program, the Fitness Professional must determine what intensity level will be most appropriate and effective for their client. Exercise intensity is described as the speed and/or the workload of a workout. Intensity is considered the most important and complicated determinant of a successful cardiorespiratory program. It is also the exercise component most often incorrectly prescribed. If the client is a beginner or is currently exercising at a lower cardiorespiratory fitness level, low to moderate intensity (50 to 60% of maximum heart rate) is considered a safe, effective starting point. For clients who want to decrease body fat and begin exercising at a low to moderate intensity, the ultimate goal is to progress to a high cardiovascular intensity level (65 to 85% of maximum heart rate). If the client is currently exercising at a high level of intensity, the Fitness Professional may be able to begin the cardiorespiratory program at a Maximum Heart Rate (MHR) of 65 to 85 percent. Higher intensity cardiorespiratory exercise burns more calories and more absolute fat in a shorter period of time. 8 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Once the Fitness Professional determines the appropriate level of cardiorespiratory intensity, accurate monitoring of the intensity level will insure that the client reaches his/her fitness goals in the least amount of time. There are numerous formulas used to monitor exercise intensity. For our Fitness Professionals' purposes, we have determined the following three formulas to be the most effective: H ow t o Det er m i ne Your H e a r t Rat e : Example: Calculating Maximum Heart Rate Percentage Lower level of activity is 65% of MHR: 185 x .65 = 120.25 1. MHR is determined by subtracting age from 220. Example: A thirty-five year old person would subtract 35 from 220 220 - 35 = 185 2. Calculate the target heart rate zone by multiplying the remaining number (185) by the MHR percentages of the high and low cardiorespiratory activity levels High level of activity is 85% of MHR: 185 x .85 = 157.25 3. Multiply result by 1.10 Example: 120.25 x 1.10 = 132 157.25 x 1.10 = 173 220 – 35 = 185 185 x .65 = 120.25 120.25 x 1.10 = 132 The complete formula for a 35 year old exercising at 85 percent intensity is: 220 – 35 = 185 185 x .85 = 157.25 157.25 x 1.10 = 173 Note: 10 percent is added to the target heart rate value to indicate the percentages of functional aerobic capacity more accurately. The complete formula for a 35 year old exercising at 65 percent intensity is: The Karvonen Formula This method measures the maximum heart rate reserve. This formula is similar to the first, however the calculations include resting heart rate. Begin by determining MHR. As in the first formula, the MHR is determined by subtracting one's age from 220. Example: A thirty-five year old person subtracts 35 from 220 220-35 = 185 Example: Resting heart rate = 75 Maximum heart rate = 185 185-75 = 110 Exercising at 85 percent intensity is: 220 - 35 = 185 185 Third, multiply the result 75 = 110 110 X .85 = (110) by the desired intensity' 93.50 75 + 93.50 = level. Example: 168.50 110 X .85 = 93.50 The Karvonen Formula is one Finally, add the resting heart of the most popular methods rate to this result (93.50). of determining cardiorespiratory intensity Example: 75 + 93.50 = 168.50 levels. The only difficulty with this method is the accurate determination of The complete Karvonen resting heart rate. Formula for a 35 year old Next, subtract the resting heart rate from the MHR 9 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 The Talk Test The Talk Test is a subjective measurement of cardiorespiratory intensity level. At low to moderate intensity, an individual should be able to breath comfortably and rhythmically throughout the entire exercise session. At high levels of cardiorespiratory intensity (65 to 85 percent), breathing will be significantly more strenuous than at rest. One is still be able to talk but finds it difficult to speak in full sentences. The Talk Test measures perceived exertion and therefore is considered an accurate estimation of exercise intensity To reach fitness goals in the most effective manner, it is vitally important to exercise at the proper level of cardiorespiratory intensity. How to Take Your Pulse: 1 . Place index and middle finger around the back side of the wrist.(about one inch from the top of wrist, on the thumb side). 2. Locate the artery by, feeling for a pulse with the index and middle fingers. Apply light pressure to feel the pulse. Do not apply excessive pressure, it may distort your results. 3. When measuring the pulse during exercise, count the number of beats in sixty seconds. Some factors that affect resting heart rate are digestion, mental activity, environmental temperature, biological rhythms, body position and cardiorespiratory fitness. So resting heart rate should be measured first thing upon wakening or at the very least, after you have completely rested for five minutes. 4. When measuring the pulse during exercise, count the number of beats in a six second period and add a zero to that number. Example: Number of beats in six seconds = 17 Add a zero - 170 Pulse rate - 170 Note: Use of the carotid artery in the neck is not recommended for measuring pulse rate. Pressure on this artery reduces blood flow to the brain, which can cause dizziness and an inaccurate measurement. 10 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 How to Use a Heart Rate Monitor: A heart rate monitor is the most accurate method of measuring pulse rate. The most accurate models include a chest and wrist unit. Monitors that attach to the ear or finger react to many movements and therefore may provide inaccurate measurements. We find the Polar Heart Monitor to be an effective instrument for measuring pulse rates. It is the most reliable and means of monitoring heart rate without confusion or error. Frequency To improve both cardiorespiratory fitness and maintain body fat at healthy levels, a client should participate in cardiorespiratory activities no less than three days per week with no more than two days between sessions. The NASM recommends three to five days per week for most programs. Every other day is appropriate for most beginners, for the first six weeks. Very overweight clients or beginners who choose weight bearing exercises (jogging, aerobic dance, etc.) should rest at least 36 to 48 hours between sessions to promote adequate bone stress recovery and prevent overuse. Duration Duration refers to the span of time during which exercise is performed, not including warm-up and cool-down. To gain cardiorespiratory benefits, duration may vary from 20 and 60 minutes per session. The benefits of an exercise program result from the combination of intensity and duration of each exercise session.. As the client becomes more fit, both intensity and duration can increase. The basic duration necessary is as follows: Beginners 10-20 minutes Intermediate (average cardiorespiratory fitness) 15 to 45 minutes Advanced (high cardiorespiratory fitness) 30 to 60 minutes Supportive Conditioning Proper stretching and resistance training can enhance a cardiorespiratory fitness program by creating a foundation that can minimize musculoskeletal injuries, stave off lean body mass loss during weight reduction and contribute to the overall body fat reduction goal. The clients' goals will determine how much resistance training is involved. It could range from as little as stretching, isometric or circuit training to a complete weight training program for strength or hypertrophy. 11 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Client Goals If cardiorespiratory fitness and basic weight control are the goal, the criteria presented in this section is complete (when matched with proper caloric intake). However, if body fat reduction to a specific percentage is desired, the Fitness Professional should also refer to the section, Altering Body Composition. Progression Plan The progression of intensity, duration and frequency should be determined by: 1. Health status 2. Age 3. Level of fitness 4. Goals 5. Cardiorespiratory response to the exercise Setting up the foundation: Setting up a cardiorespiratory program is basically the same for most goals. The intensity should be low-level aerobic activity and stretching. Exercise heart rate should be between 50 and 60 percent of maximum heart rate reserve (Karvonen). Depending on functional capacity and current level of fitness, beginning duration should be 10 to 20 minutes. Clients with very poor conditioning may start with 5 to 10 minutes and progress according to cardiorespiratory response. Frequency should begin with alternating exercise days. This foundation phase should last approximately four to six weeks, depending on the client's overall response, including musculoskeletal. Progression Entering, into the second phase of the cardiorespiratory program, all three variables can begin to increase, depending on the goal, cardiorespiratory and musculoskeletal response. Intensity can increase from. 50 to 90 percent of MHR, over a 15-week period. Duration can increase every 2 to 3 weeks. Frequency may also increase to 4 to 6 times per week. Progress should be measured at 3-week intervals. 12 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 High Intensity vs. Low Intensity Cardiovascular Exercise It has been debated whether more body fat is burned at higher or lower cardiovascular intensity levels. It is true that the body will burn a higher percentage of calories from fat stores when engaging in less intensive cardiovascular work. It is also true that, when participating at higher intensity levels of cardiovascular work, the body burns a greater amount of calories. A lower percentage of the burned calories will be from the body's fat stores but the body is still burning more absolute calories from fat. To explain this phenomenon, let's look at the experience of an average 130-pound woman who engages in cardiovascular activity at high and low intensities. Low intensity - 50 % of V0 2 max. or approx 60 - 65% MHR Total calories expended per min. Fat calories expended per min Total calories expended in 30 min. Total fat calories expended in 30 min. Percentage of fat calories burned High intensity - 70% of V02 Max or approx 80 - 85% MHR 4.86 6.86 2.43 2.7 146 206 73 82 50% 39.85% As the chart indicates, of the 146 calories burned at a lower intensity, 73 were burned from fat. At the higher intensity, 206 calories were burned - 82 of which were from the body's fat stores. Therefore, when exercising at higher intensity, the body not only burns more calories, it also burns more fat. Recent research has demonstrated that higher intensity exercise will result in greater weight and fat loss. Ballor, et al. investigated the effect of exercise intensity on the rate and composition of weight loss over a period of eight weeks. One group of subjects cycled for 25 minutes at-80 to 90 percent of V02 max (i.e., high intensity exercise); another group of subjects cycled for 50 minutes at 40 to 50 percent of V02 max (i.e., low intensity exercise). Both groups expended the same number of calories per session, with the group exercising at the lower intensity expending more fat calories. When the study concluded, both groups had lost the same amount of weight and fat. Therefore, regardless of the exercise intensity and the type of fuel used (i.e., calories from fat or muscle), both groups of subjects experienced the same results. Clients may be concerned about whether cardiovascular activity (at either high or low intensity) will result in a loss of lean muscle tissue. Regardless of the exercise intensity, if the client is not providing his/her body with the appropriate amount of nutrients from food and supplementation, there will be a decrease in lean muscle mass. However, if the body is supplied with the necessary nutrients, it is possible to actually gain lean muscle tissue. Protein or muscle degradation initiates protein synthesis and thus, the net result is more protein synthesis (when the proper nutrition is supplied). Additionally, if your clients are participating in the proper amount of cardiovascular work,, they will be able to increase caloric intake and continue to lose body fat. In turn, the increase in calories will allow for the building or maintenance of lean body tissue. The bottom line is this: depending on the client's goal, personal preference (i.e., exercising for a longer period of time at a low intensity or for a shorter period at a higher intensity) may determine the intensity of his/her cardiovascular workout.* High intensity exercise is an excellent way to break a fat loss plateau but your client should be in good 13 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 cardiorespiratory condition prior to beginning such a workout program. *Note: High intensity cardiovascular activity is not recommended for clients who are novice exercisers. If the client is currently taking certain prescription medication, cardiorespiratory exercise may be prohibited. Be certain the client obtains the permission of his or her physician prior to participating in a workout program. Maintenance Once the client achieves the cardiorespiratory or fat loss goal, frequency, intensity and/or duration can be slightly reduced to maintain it. The cardiorespiratory progression for continuous body fat reduction is found in the Altering Body Composition section. Safety Part of safe, effective exercise is knowing when to abstain from exercise. Ensure your clients' safety by becoming familiar with their individual health and orthopedic conditions and levels of fitness. List any concerns in your client's individual record. Be aware, and inform your clients of conditions in the exercise environment that could prove hazardous. • • • • • Hot, humid exercise areas. Refrain from exercise for at least 90 minutes after eating. Discontinue exercise in the event of dizziness, lightheadedness or chest pain. Reduce exercise intensity at high altitudes (above 5,000 ft.) or in hot or humid conditions. In the presence of an injury (such' as joint tenderness), avoid exercise, which may further aggravate the condition. • Do not engage in strenuous aerobic activity during a viral or upper respiratory tract infection. Cardiorespiratory or Weight Training: Which Should My Client Do First? When determining whether to perform cardiorespiratory (i.e., aerobic) or weight training (i.e., anaerobic) exercise first, it is important to determine if the client has the luxury of training twice daily. If this is the case and the client has eaten properly, it does not matter whether weight training or cardiorespiratory activity is performed first. However, if the client is not able to train twice daily, then it makes a significant difference whether he/she begins the workout routine with aerobic or anaerobicc exercise. The first step in the decision-making process should be to determine the client's fitness goals. If the client is attempting to build lean body mass, it may not be necessary for him/her to engage in cardiorespiratory activity. If the client's goal is to increase aerobic performance, cardiovascular activity should precede weight training. However, if the client's goal is to lose body fat and build or maintain lean body mass, the most effective training routine is one in which weight training immediately precedes cardiorespiratory exercise. The order is important because each of these activities has its own energy source. Anaerobic exercise, such as weight training, requires stored glycogen (i.e., glucose) as an energy source. Therefore, prior to engaging in anaerobic activity, it is necessary to fill the body's glycogen stores to experience 14 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 the optimal results associated with an energetic and effective weight training routine. Aerobic exercise (e.g., cycling, running) requires both glycogen and fat stores for energy. At the onset of cardiovascular activity, the body relies primarily on stored glycogen for energy. Depending on the client's level of cardiorespiratory fitness, the body will use predominantly glycogen for the first 5 to 20 minutes of physical activity. This is the first stage of cardiorespiratory activity. The body begins to burn the greatest amount of fat when it enters the second stage of cardiorespiratory activity but the body also continues to use stored glycogen. It is not possible to bum fat efficiently without the presence of glucose. Weight training workouts use only glycogen for energy, therefore, the client's glycogen stores should be as full as possible prior to beginning anaerobic activity. Both glycogen and fat stores are significantly depleted during cardiorespiratory activity. If clients begin their workouts with cardiorespiratory training, they will have exhausted a substantial amount of their glycogen stores. As a result, when they begin their weight training routine they will not have the energy necessary for an optimally productive workout It is also important that clients eat properly prior to beginning the workout routine. The exception to the aforementioned are those clients who are only interested in losing fat. These individuals may begin their workout routine with cardiorespiratory activity (when preferred or their schedule allows) and then proceed directly to a circuit or weight training routine. Weight training should take place at a brisk pace in order to keep the heart rate elevated and remain, partially, in a fat burning stage. This type of workout will not build a significant amount of lean body tissue but it can be an effective method for losing fat. 15 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Summary • Increasing cardiorespiratory fitness contributes to the progress of nearly all sports and conditioning programs. Components of the program are: 1. Warm-up and cool-down 2. Activity criteria: mode, intensity, frequency, duration 3. Supportive conditioning: strength training and flexibility 4. Client's goal 5. Progression plan 6. Safety • High intensity cardiorespiratory activity burns more calories and more absolute fat than low intensity. • If the client's goal is continuous body fat reduction, see Altering Body Composition section. • Monitor intensity, cardiorespiratory fitness and body fat reduction according to guidelines and make appropriate adjustments. • Use the appropriate progression outline as cardiorespiratory fitness improves and/or body fat decreases. • Pay attention to safety rules. 16 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 References American College of Sports Medicine, Guidelines for exercise testing and prescription, Lea & Febiger, Phil., PA, 1991. American College of Sports Medicine, The recommended quantity and quality of exercise fro developing and maintaining fitness in healthy adults. ACSM position statement Medicine and Science in Sports and Exercise, 22, 1990. Borg, G.V., Psychological basis of perceived exertion. Medicine and Science in Sports and Exercise, 14,377381, 1982. Carlton, R., & Rhodes, E., A critical review of the literature on the ratings scales of perceived exertion. Sports Medicine, 2 , 198-222, 1985. Durstine, L., & Pate, R., Cardiorepiratory responses to acute exercise. In American Painter, P., & Haskell, W., Decision making in programming exercise. In American College of Sports Medicine, Resource manual for guidelines for exercise testing and prescription (pp. 256 - 262).Lea & Febiger, Phil., PA, 1988. Parker, S., Hurley, B., Hanlon, D., & Vaccaro, P., Failure of target heart rate to accurately College of Sports Medicine, Resource manual for guidelines for exercise testing and prescription, Lea & Febiger, Phil., PA, 1988. Folinsbee, L., Exercise and the environment. In C. Brochard, R. Shepard, T. Stephens, J. Sutton, & B. McPherson (Eds.), Exercise fitness and health (pp.429-453). Champaign, 11, 1990. Giese, M., Organization of an exercise session. In American College of Sports Medicine, Resource manual for guidelines for exercise testing and prescription (pp. 244-247). Lea & Febiger, Phil., PA. McArdle, W., Katch, F., Katch, V., Exercise physiology, Lea & Febiger, Phil., PA, 1986. Nieman, D., Fitness and sports medicine: an introduction. Bull Pub., Palo Alto, CA, 1990. monitor intensity during aerobic dance. Medicine and Science in Sports and Exercise, 21, 230, 1989. Pollack, M., The quantification of endurance training programs, Exercise and Sport Science Reviews, 1, 155 188, 1973. 17 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 The Science of Resistance Training It is the role of an Apex Fitness Professional to have vast knowledge of nutrition and supplementation for the goal of altering body composition (i.e., muscle hypertrophy and fat loss) but this is only part of the equation. To be successful, the Fitness Professional must also understand the manipulation of both aerobic and anaerobic exercise components. Aerobic exercise is discussed elsewhere in this manual. This section provides information the Fitness Professional needs to be successful when working with trainers on recommending and/or scrutinizing resistance training programs. Before discussing the physiological factors necessary to continuously spur the hypertrophic response, a basic understanding of biomechanics and muscular and nervous system physiology is needed. Biomechanics is defined as the study of motion and the effect of forces on biological systems. In college courses, biomechanics is usually applied to comprehensive sport specific movements. In this course, we discuss biomechanics as it relates to target muscles and their motion. This approach is rarely taken but is extremely beneficial to a Fitness Professional, since it is a significant part of creating the greatest stimulus for muscle hypertrophy. Tom Purvis, co-owner of Focus On Fitness® and head Fitness Professional for the National Academy of Sports Medicine, has developed six steps that are necessary to create and monitor any resistance training exercise. These six steps can be used to ensure that the exercise is being performed safely and effectively for the goal of working the target muscle(s). The six steps are: Six Steps Necessary To Perform Any Exercise I. Muscle/Motion: What motion is being performed? a. b. c. d. II. III. IV. What muscle are we working? Name muscle and goal. The muscles attachments. Origin and insertion. The muscles fiber direction. The motion the muscle performs. Where is the direction of resistance coming from? a. Gravity b. Cables c. Tubing d. Machines What position should the body be in to allow the motion to directly oppose the resistance? a. Position the body against resistance. Stabilization a. Explain joints involved in proper stabilization of the body: i. Ankle, knee, hip, spine, scapula, shoulder, elbow, wrist, head. b. Stabilize all joints except the joints moving. 18 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 V. Path of Motion a. Where you start is where you stay. b. Path must be resisted. Example: A standing dumbbell chest press is not effective, the dumbbell chest press becomes effective in the supine position c. You cannot have resistance in two planes of motion. VI. Example: A front pulldown that is pulled down to the point where the elbows begin to move to the posterior of the body. Range of Motion a. Definition - Full range of motion is the distance a joint can move before the body hits a structural barrier. b. Method the body uses to limit range of motion: i. Neurological ii. Physiological iii. Anatomical c. Full concentric and eccentric contraction determined by touching the muscle or by what the body is doing. i. Was stabilization maintained? The first three steps are questions we must answer to help create the perfect exercise. The first question addresses the motion that will be performed. This is determined by the client's goal. If the goal is to work a specific muscle, knowledge of what motion that muscle performs, its attachments and fiber direction, will be helpf l. The second step is to determine from what direction the resistance will come. This can usually be narrowed down to one of four directions: gravity, cables, tubing, machines. Answering the question in the second step tells us how to answer the question posed by the third step, how to position the body to directly oppose the resistance. When all three of these questions are addressed and correctly answered, we can be relatively sure the exercise is being created properly. The next three steps are used to monitor the exercise for safety and effectiveness. Step four, stabilization, is essential in this process. A good rule of thumb is to position the uninvolved extremity first, then the spine, and then monitor and maintain these positions without fail. Step five is to monitor and maintain the proper path of motion, determined by the goal. Allowing any other motion may be unsafe and decrease effectiveness of the exercise. Finally, we must use the proper range of motion, or how far you move concentrically and eccentrically. Range of motion is determined by the joint/muscle involved, not how far the weight was moved. Having discussed basic biomechanics for muscles and motion, we will review nervous and muscular system physiology. 19 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Nervous System The nervous system is composed of the Central Nervous System (CNS), and the Peripheral Nervous System (PNS). The CNS includes the brain and spinal cord. The PNS includes an efferent (or motor) division and an afferent (or sensory) division.The neuron is the basic functional unit of the nervous system and is composed of a cell body (or soma), dendrites, which act as receivers for incoming signals from adjacent neurons, and an axon, which is the fiber like extension of the nerve cell. Figure 1 Information enters the spinal cord and brain, from sensory receptors, where it is processed and relayed back to the periphery via efferent or motor neurons. When an impulse reaches a specific motor neuron, it is passed along to each muscle fiber innervated by that motor neuron. The motor neuron and the muscle fibers it innervates are referred to as a motor unit. Neuromuscular activity is graded on the basis of a fixed order of recruitment from the available pool of motor units. The more force needed to execute a certain movement, 20 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 the more motor units are recruited. Figure 2 Muscular System: Skeletal Muscle Skeletal muscle is composed of several kinds of tissue including muscle cells, nerve tissue, blood and various types of connective tissue. Each muscle fiber is a thin, elongated cylinder that generally extends the full length of the muscle. The cell membrane in muscle is called the sarcolemma. Beneath the sarcolemma lies the sarcoplasm, which contains the cellular proteins, organelles and myofibrils. Myofibrils are numerous, thread=like structures that contain the contractile proteins, actin and myosin. Myofibrils are also divided into individual segments called sarcomeres. Sarcomeres are divided from each other by a thin sheet of connective tissue called a Z line. Muscular Contraction Muscular contraction is a complex process involving a number of cellular proteins and energy production systems. The final result is the sliding of actin over myosin, which causes the muscle to shorten and therefore, develop tension. The process of muscular contraction is best explained by the sliding filament theory of contraction, which states that simultaneous sliding of many thousands of sarcomeres, in series, creates a change in length and force in muscle. The amount of force that can be developed in the muscle is proportional to the number of cross-bridges formed. Shortening of many sarcomeres, myofibrils and fibers develops tension in the muscle. An actual movement is created by this tension, applied at both ends of the muscle to the bone. When the cross-bridges in the sarcomere are active and cycling, the change in length of the sarcomere depends on the amount of force exerted by the cross-bridges, relative to the size of the load acting on the sarcomere. If sarcomere force and the magnitude of the load are the same, the sarcomere length and the joint angle remain constant. This results is an isometric contraction. When the two forces are not equal, sarcomere length will change. If a muscle generates tension actively, with visible shortening in the length of the muscle, 21 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 the muscle action is a concentric contraction. When a muscle is subjected to an external torque that is greater than the muscle's internal torque, there is lengthening in the muscle. This is known as an eccentric contraction. Muscle Fiber Types The primary fiber types are classified by their particular mechanical and biomechanical characteristics. Type I muscle fibers contain a high concentration of myoglobin, glycogen and triglycerides. These red, slow-twitch fibers have relatively high concentrations of mitochondria and aerobic enzymes and are densely surrounded by capillaries. They have a very high aerobic or oxidative capacity and are involved predominantly in lower intensity, prolonged, endurance activities. At present, no research exists to confirm that Type I fibers exhibit significant hypertrophic responses to weight training exercises. In contrast, Type II muscle fibers have a low concentration of myoglobin, glycogen and triglycerides. These white, fast-twitch fibers have a low capillary to fiber ratio and fewer mitochondria and aerobic enzymes. Type II fibers are low in oxidative capacity but high in anaerobic or glycolytic potential. Utilization of Type II muscle fibers occurs primarily during high intensity activities. Fast-twitch, Type II fibers can be classified further into two common subgroups; Type Ha (fast-twitch oxidative/glycolytic [FOG] fibers) and Type IIb (fast-twitch [FG]) fibers). Both types of fast-twitch Type II fibers are recruited during weight lifting exercises and are involved in adaptive responses to resistance training. Controlling Eccentric Movement to Spur Growth Resistance training must include exercises that employ both concentric and eccentric components. Eccentric loading is defined as the lengthening of the activated muscle (lowering of the weight) or the lengthening of contractions. To induce significant stimulus for muscle hypertrophy, the client must control both the lifting and the lowering of the weight. With equivalent loads, the stress incurred by individual fibers involved an eccentric contraction is 50 to 100 percent greater than the stress incurred by muscle fibers during concentric or isometric movements. Detachment of the cross-bridges during the eccentric movement involves a mechanical disruption of the chemical bond. This is in contrast to the more orderly binding adenosine triphosphate (ATP) and cross-bridge detachment that occurs during a normal cross-bridge cycle. Because of this, eccentric exercise may provide an effective stimulus for hypertrophy. Muscle Damage Overloading the muscle with resistance results in cellular damage at the muscle's weakest link, the sarcomere. The sarcomere's weak link is the point where the filaments are attached to the Z lines. When significant stimulus is introduced, the structure of the sarcomere is physically disrupted by pulling of the filaments, off and away from the Z lines. During weight training, this occurs mostly within Type II fibers. Nervous System Adaptation Scientific study of the relationship between short duration training and increases in strength show that strength gains are influenced by neural adaptations related to learning, coordination and the ability to recruit prime movers. Prior to muscular hypertrophy, changes in the central nervous system enhance motor unit synchronization during particular movement patterns. Changes in the central nervous system 22 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 also increase the number of motor units recruited and the firing rate of the motor neurons. These adaptations result in an increase in the amount of muscular force generated. Generally, increases in strength have been reported to occur within a few weeks of beginning a strength training program. The body must learn to perform the movement properly and complete the necessary muscle fiber and other cellular adjustments. Once these adaptations are completed, even before experiencing significant growth, the muscle will be able to work at a greater capacity. Skeletal Muscle Adaptation Recent research also indicates that the body responds to progressive weight training by converting the Type IIb (least oxidative) fibers to Type IIa (higher oxidative) fibers, in order to meet its increased energy (ATP) needs. This adaptive response explains why a person experiences muscle strength gains prior to an increase in muscle size. The body's adaptation to the change in cellular environment, its ability to produce ATP faster and longer, increases the oxidative capability of the fibers. Muscle fibers are able to increase their oxidative capability more rapidly than size. Current researchers believe this process helps prepare the muscle for hypertrophy. Muscle Remodeling - Repair and Hypertrophy In addition to the muscle fiber's ability to convert from Type IIb to Type IIa fibers, the damaged muscle cells eventually rebuild and increase in diameter. This contributes significantly to the fiber's cross23 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 sectional growth area and results in muscle hypertrophy. As there is no direct correlation between muscle size and strength, there must be another type of protein exchange that leads to muscle hypertrophy. Although strength does increase with resistance training, it is possible to make significant gains in strength without a notable increase in muscle size. On the other hand, it is. also possible to experience muscle hypertrophy without increasing the strength of the muscle The Contribution of Satellite Cells to Muscle Hypertrophy We have discussed how increased fiber diameter and transformation of muscle fibers from Type IIb to Type Ha contribute to the process of muscle hypertrophy. Recent research reveals that simultaneous activation of various proteins has been identified by researchers as a contributing element in the process of muscle repair. This additional response to resistance exercise is due to the presence of a satellite cell population, adjacent to mature muscle fibers. With continued weight training and the resulting muscle damage, the dormant satellite cells become activated by specific proteins. A combination of proper resistance training and the passage of time results in the growth of these smaller, less mature fibers and their eventual fusion to the more mature, hypertrophied muscle fibers. This fusion may increase the muscle's ability to repair itself after damage has occurred. Summary Proper weight training of adult skeletal muscle provides significant stimulus to increase muscle size. If the muscle is to continue to grow to its genetic potential, the eccentric contraction and continual muscle overload are necessary. Enlargement of the muscle is primarily the result of an increase in the fiber cross-sectional area. To a lesser degree, muscle size increases can be attributed to the increase in non-contractile proteins, such as those found within the sarcoplasm and connective tissue 24 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 References Alway, S. E., Gonyea, W.J. and Davis, M.E., Muscle fiber formation and fiber hypertrophy during the onset of stretch-overload. Am. J. Physiol. (Cell Physiol.) 1990. Antonio, J. and Gonyea, W.J., Branched muscle fibers in stretch-enlarged avian muscle. Med. Sci. Sports Exer. 25:51, 1993. Bischoff, R., Cell cycle commitment of rat muscle satellite cells. J. Cell Biol. 111:201-207, 1990. Bischoff, R., Interaction between satellite cells and skeletal muscle fibers. Development 109:943952,1990. Carlson, B.M., The regeneration of skeletal muscle. Am. J. Anat. 137:119-150, 1973. Cote, C., Simoneau, P., and Lagasse, P. et al. Isokinetic strength training protocols: do they induce skeletal muscle fiber hypertrophy? Arch. Phys. Med. Rehabil. 69:281285,1988, the American College of Sport Medicine. 26,: S25,1993. Staron, R. et al. 1989. Muscle hypertrophy and fast fiber type conversions in heavy resistancetrained women. European Journal of Applied Physiology. 60:71-79. Vracko, R and Benditt, E.P., Basal lamina: The scaffold for orderly cell replacement. J. Cell. Biol. 55:406-419,1972. Winchester, P.K., Davis, M.E., Alway, S.E., and Gonyea, W.J. Satellite cell activation of the stretch-enlarged anterior latissimus dorsi muscle of the adult quail. Am. J. Physiol. 260: C206-C212,1991. Giddings, C.J., Neaves, W.B., and Gonyea, W.J., Muscle fiber necrosis and regeneration induced by prolonged weight-lifting exercise in the cat. Anat. Rec. 211:133141, 1985. Hather, B.M., Tesch,P.A., Buchanan, P. and Dudley, G.A., Influences of eccentric actions on skeletal muscle adaptations to resistance training. Acta Physiol. Scand. 143:177 - 185, 1991. Lieber, RL., Patel, T.J., Ahsan, T. and Friden, J., Effects of intermittent stimulation on eccentric contraction induced muscle injury, Official Journal of the American College of Sport Medicine. 26,: S25, 1993. Mauro, A., Satellite cell of skeletal muscle fibers. J. Biophys. Biochem. Cytol. 9:493-494,1961. Schwane, J.A., Delayed muscle soreness (DMS), plasma creatine kinase activity (PCK) and rate of oxygen consumption (VO2) during downhill walking (DH). Official Journal of Winchester P.K. and Gonyea, W.J., Regional injury and terminal differentiation of satellite cells in stretched avian slow tonic muscle. Dev Biol. 151:459-472, 1992. Wong, T.S. and Booth, F.W., Protein metabolism in rat gastrocnemius muscle sfter stimulated chronic concentric exercise. J. Appl. Physiol. 69: 1709-1717, 1990. Wong, T.S. and Booth, F.W., Protein metabolism in rat tibialis anterior muscle after stimulated chronic eccentric exercise. J Appl. Physiol. 69: 1718-1724,1990. 25 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Designing Your Client's Workout For Muscle Hypertrophy This article presents the training factors necessary to produce the greatest possible stimulus for muscle hypertrophy. Hypertrophy results from an increase in the number and size of myofibrils. It is best to accomplish this goal with the least amount of specific work needed to initiate a change. This ensures that, when progress reaches a plateau, the Fitness Professional has room to alter the workouts, so clients remain unaccustomed to them. It is also important for the Fitness Professional to realize the differences between training novice level clients and training intermediate to advanced level clients. To begin, we will outline the needs of a novice level client during the initial stages of a resistance training program. The remainder of the article explains each training factor and the manipulation techniques required to create continuous, unaccustomed stimulus for muscle hypertrophy for intermediate to advanced level clients. Novice Client As stated, novice level clients experience strength increases before size increases. This is due to neuromuscular learning and coordination that takes place at the onset of a resistance training program. The body must establish these patterns before it can recruit sufficient motor units needed to create adequate tension for muscle hypertrophy. Because of this, the Fitness Professional must focus early education on proper movement patterns (proper biomechanics), using the six steps necessary to create safe and effective exercise. This takes precedence over what the client "feels" during an exercise. Once the neuromuscular patterns are established (after approximately 16 workouts, studies show), the Fitness Professional can add new movements and increase the intensity of the stimulus. At this point, the novice becomes an intermediate level client. Intermediate to Advanced Level Clients It is important to keep the workouts unaccustomed when attempting to create the greatest stimulus for muscle hypertrophy for intermediate to advanced level clients.. Fitness Professionals should understand the effects of the following training factors and the ranges recommended for muscle hypertrophy. Also, be aware that training for strength, muscle endurance and muscle hypertrophy may each. require a separate stimulus for appropriate adaptation. Training Factors 1. Number of repetitions 2. Number of sets per body part 3. Amount of rest needed between sets 4. Speed of contraction 5. Amount of rest needed between body parts 6. Training to muscular failure 7. Effects of lifestyle 26 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 The Number of Repetitions to Perform The goal for muscle hypertrophy is to achieve true muscular failure. This requires raising the level of tension in the muscle for a specific amount of time, so the number of repetitions to perform is of vital importance. The amount of time needed can be measured in repetitions. Empirical and anecdotal evidence have shown that 6 to 15 repetitions provide the amount of time necessary for muscle hypertrophy. It is also essential to continuously alter the repetition scheme, within this range, to create an unaccustomed stimulus. The Number of Sets to Perform Per Body Part The number of sets devoted to training each body part is a complex matter. As stated, hypertrophy is simply the muscle's adaptive response to an unaccustomed stimulus. The recommended number of sets for each body part will vary depending on the client's ability to: 1. Concentrate on the target muscle. 2. Focus on and maintain the proper biomechanics of the movement. 3. Control the contraction through both the concentric and eccentric components. 4. Use proper form regardless of the amount of weight lifted or the number of repetitions. Recent research indicates that, if the client adheres strictly to these four principles, the . stimulus necessary for the growth response can be initiated with 6 to 10 sets. Unfortunately, most Fitness Professionals find it difficult to properly instruct their clients to adhere to these principles. This forces many Fitness Professionals to increase the number of sets to achieve muscular failure. This may be due to the fact that the target muscle is only performing a portion of the work. When the training factors are not properly applied, much of the work performed can be dispersed and absorbed by adjacent muscle groups. This results in the target muscle not receiving the proper stimulus. Taking this into account, the basic recommended range of sets per body part groups is: 6 to 12 sets for large muscle groups (e.g., chest, back, shoulders, quadriceps), 8 to 10 sets for smaller muscle groups (e.g., biceps, triceps, hamstrings, calves) and 4 to 6 sets for miscellaneous muscle groups (e.g., traps, lower back, abdominals). If the number of sets the client requires exceeds these recommendations, the client is not performing safe and effective exercise and is in danger of overtraining. Remember, more is not better. The Amount of Time Spent Resting Between Sets The amount of time spent resting between sets is an often overlooked variable. We can be relatively sure that the end of a set is the result of muscular fatigue, rather than nervous system fatigue, if we follow the factors outlined here. Our goal is to rest long enough to replenish the nervous system but leave the muscle fibers slightly fatigued. Therefore, the amount of rest needed will range from 30 seconds to 2 minutes. For example, if the client achieves muscular fatigue in 6 to 8 repetitions, he/she should rest for 1.5 to 2 minutes. If the client achieves muscular fatigue in 10 to 12 repetitions, he/she may only require 30 seconds to 1 minute of rest. As with all other factors, the amount of rest time should be continuously altered to create an unaccustomed stimulus. 27 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 The Speed of Contraction Numerous studies have examined the effect of contraction speed on strength increases. Most of these studies advocate a faster contraction speed for this specific goal. Because of the belief that any increase in strength will lead to an increase in size, many Fitness Professionals feel that a faster contraction speed is best. However, if the goal is to achieve muscle hypertrophy with the safest, most effective stimulus, the speed of the concentric contraction should equal the speed of the eccentric contraction, with the major emphasis on controlling the resistance. If the client concentrates on the target muscle and.. its motion, rather than how far he/she moves the weight, this goal is easily accomplished.. Resting Between Body Parts Most research regarding tissue damage and the repair process initiated from unaccustomed stimulus indicates that the body requires from four to seven days to recover completely. Many factors contribute to determining the amount of rest necessary between body parts including: goals, the client's genetic predisposition to repair,. the intensity of the workout and indications of overtraining. Although it is difficult, if not impossible, to accurately assess these factors and establish the exact amount of rest needed, four to seven days is sufficient recovery time for most intermediate to advanced. level clients. Training to Muscular Failure We know that, to create the greatest stimulus for muscle hypertrophy, the target muscle must be trained to failure. This can be accomplished by fatiguing the muscle for a number of sets, until true muscular failure is achieved. Muscle fatigue is best defined as the inability to maintain tension in the target muscle, demonstrated by the inability to perform the exercise properly. The Effect of Lifestyle The client's chosen lifestyle is the most important factor to consider because it determines the recommended training regime. For example, you may decide that the client should workout for four consecutive days, take a day off, then repeat the cycle. If the client does not wish to workout on weekends, this regime will not be effective. The Fitness Professional must know the amount and type of time the client will devote to training before recommending a regime that is conducive to the client's goals. Summary We have reviewed the training factors necessary to create the greatest stimulus for the goal of muscle hypertrophy The Fitness Professional should now be able to design a safe, effective training regime that is tailored to the client's individual requirements. Most Fitness Professionals manipulate only the amount of weight lifted, in hopes of achieving an unaccustomed effect. This approach is less effective and, if excessive loads are used, could cause unwanted injury. The information presented illustrates how muscular hypertrophy can result from the manipulation of many different variables. The safest, most effective way of creating the greatest stimulus for muscle hypertrophy is to continuously manipulate all these training factors. It is also important to realize that unaccustomed exercise is only the triggering mechanism for growth. Adequate rest, proper nutrition and proper supplementation create the ideal environment for repair. Establishing an enjoyable workout. routine that complements the client's lifestyle and incorporates his/her ability to recover, concentrate and avoid injury, will facilitate maximum muscular growth. References 28 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004 Bischoff, R., Cell cycle commitment of rat muslce satellite cells. J Cell Biol. 111:201 - 207, 1990. Giddings, C.J., Neaves, W.B., and Gonyea, WJ., Muscle fiber necrosis and regeneration induced by prolonged weightlifting exercise in the cat. Anal. Rec. 211:133 - 141, 1985. Higbie, E.L., Cureton, K.J., Warren, G.L., and Prior, B.M., Effects of concentric and eccentric isokinetic training of muslce strength, crosss-sectional area and neural activation. Official Journal of the American College of Sports Med. 26, S31, 1993. Mikesky, A.E., Matthews, W., Giddings, C.J. and Gonyea, W.J., Muscle enlargement and exercise performance in the cat. J. Appl. Sport Sce. Res. 3: 85 - 92, 1989. Starkey, D.B., Welsch, M.L., Pollack, M.L., Graves, J.E. and Brechue, W.F., Equivalent improvement in strength following high intensity, low and high volume training. Official Journal of the American College of Sports Med 26, S 116, 1993. Touey, P.R, Sforzo, G.A., and McManis, B.G., Effects of manipulating rest periods of isokinetic performance. Official Journal of the American College of Sports Med. 26. S26, 1993. 29 All Contents Copyright International Association of Certified Professional Fitness Trainers, 2004