Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adaptive immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Molecular mimicry wikipedia , lookup
Innate immune system wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
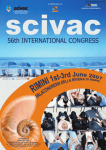
doi: 10.1111/1346-8138.12697 Journal of Dermatology 2015; 42: 11–17 REVIEW ARTICLE Immune cellular regulation on autoantibody production in pemphigus Meng PAN, Haiqin ZHU, Renchao XU Department of Dermatology, Rui Jin Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China ABSTRACT Pemphigus is an autoantibody-mediated blistering disease in the skin and mucous membranes. The autoantibodies primarily target desmoglein (Dsg)1 or/and Dsg3, transmembrane glycoproteins of skin epidermal cells, leading to loss of desmosome adhesion and acantholysis through signaling dependent and independent pathways. Thus, the pemphigus autoantibodies themselves and immune processes, particularly cellular regulation of antibody production, remain as interesting topics in probing pemphigus pathogenesis. In this review, we focus on current advances regarding how the pemphigus antibody production is highly regulated by the key immune effectors including T cells, B cells and their secreted cytokines. Specifically targeting these immune effectors involved in the pemphigus autoantibody production should provide better therapeutic options for disease treatment of pemphigus. Key words: tolerance. autoantibody production, autoreactive T and B cells, pemphigus, regulatory cells, T- and B-cell INTRODUCTION Pemphigus is an autoimmune disease, characterized by intraepidermal blistering of the skin and mucous membranes. Recent studies have suggested that this disease is mediated by pathogenic but not non-pathogenic autoantibodies in the blood from patients.1 A series of prior studies and still-accumulating data have also revealed that these antibodies mainly target desmogleins (Dsg), a critical glycoprotein found predominantly in the skin epidermis.2–4 Passive transfer of anti-Dsg3 antibody into neonatal mice could induce the disease,3,4 a milestone work in exploring the pemphigus pathophysiology. Conversely, removal of the autoantibodies from the sera prevents the induction of pemphigus in vivo. Taken together, the specific autoantibodies are necessary and sufficient for development of pemphigus. Despite the previous exciting findings, the exact mechanisms for antibody production remain largely unclear. In antibodymediated humoral immune response, B cells could break the self-tolerance and produce the antibodies, although the checkpoint by which loss of B-cell tolerance occurs requires further investigation. In systemic lupus erythematosus (SLE), the point at the level of dysfunction of the interleukin (IL)-secreting regulatory B cells has been linked to development of autoimmunity.5 In pemphigus, depletion of the CD19+ CD27+ memory B cells and presence of more regulatory interleukin (IL)-10-producing B cells have been attributed to the long-lasting complete remission of the disease,6 indicating that the checkpoint may locate at some point of B-cell maturation into memory B cells. Cell-mediated immunity and cytokines may also be essential components in the phenotypic expression of disease. For instance, in an active murine model, the Dsg3–/– mice were immunized with recombinant Dsg3, which leads to the induction of Dsg3-specific immune response, including development of autoreactive T and B cells.7 The Dsg3-primed splenocytes were then transferred into the Rag2–/– mice, an immunodeficient mouse without mature T and B cells but intact Dsg3 distribution and expression, leading to an animal pemphigus phenotype. The results showed that the anti-Dsg3 IgG antibody production and clinical phenotypes were only observed from the mice that were transferred with both T and B cells, indicating that both T and B cells were involved in the triggering phase of the disease and T cells may stimulate B-cell maturation during the process of autoantibody production.7 On the other hand, it is known that in some healthy individuals and the relatives of the patients, the low titer-specific anti-Dsg antibody could be detected. These antibodies are more likely to be non-pathogenic, given that the patients have no clinical symptom, suggesting the necessity of orchestrating multiple immune effectors to produce the pathogenic antibodies. More recently, a shared gene usage of the antibody heavy chain has been identified for the pathogenic autoantibodies cloned from different pemphigus patients,8 suggesting a common genetic and immune mechanism of autoantibody production and disease pathogenesis. In this Correspondence: Meng Pan, M.D., Ph.D., Department of Dermatology, Rui Jin Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China. Email: [email protected] Received 2 October 2014; accepted 3 October 2014. © 2015 Japanese Dermatological Association 11 M. Pan et al. review, we attempt to focus on the immune regulating network on antibody production in pemphigus, including the self-tolerance, regulatory cells and related cytokines. INITIATION OF AUTOANTIBODY PRODUCTION AND LOSS OF SELF-TOLERANCE IN B CELLS B cells serve as one of the major autoantibody-secreting cells in autoimmune diseases. Additionally, they may function as selfantigen-presenting cells. Furthermore, B cells may regulate the T-cell development and function in vivo through multiple mechanisms. In treatment of pemphigus vulgaris (PV) patients, rituximab (an anti-CD20 monoclonal antibody) has been reported to cause long-lasting remission by specifically targeting the CD20+ pre-B cells and mature B cells (memory B cells),6 supporting that B cells are central to pemphigus initiation and development. Further studies have showed that depletion of B cells by administration of rituximab could impair the T-cell function,9 thus enhancing its effect on reduction of autoantibody production. At the early phase of autoantibody production, a potential mechanism is triggered by an exogenous antigen (e.g. from viral infection) sharing similar epitope structures with human Dsg, leading to autoantibody production. When exposed to this foreign antigen, the human immune system presumably develops polyclonal antibodies against it. Because of the similarities with Dsg, the produced antibodies may also cross-react with Dsg that are specifically expressed in the skin epidermis, resulting in skin acantholysis or pemphigus. In fogo selvage (FS), known as a type of endemic pemphigus foliaceus in Brazil, immunoglobulin (Ig)G4 autoantibody against Dsg1 is believed to mediate the disease pathogenesis.10 Interestingly, the FS autoantibodies can bind to an LJM11 salivary protein isolated from the sand fly salivary gland, suggesting that molecular mimicry of the self-antigens (Dsg) and non-infectious or infectious antigens may initiate the pathogenic autoantibody production in pemphigus. This notion is further supported by the fact that mice challenged with this antigen were able to develop antibodies cross-reacting with Dsg1.10 Alternatively, B cells that produce non-pathogenic antibodies against Dsg may naturally exist in normal human individuals, as clearly demonstrated by antibody library screening using phage display1,11 and detection of low titer-specific antiDsg antibodies in healthy individuals.12 Indeed, it was estimated that as much as 75% newly generated bone marrow B cells express B-cell antigen receptors that are able to bind self-antigens.13 Yet, a vast majority of the self-binding and -destructive autoimmune reactions will be blocked possibly due to the B-cell self-tolerance by negative selection. The potential mechanisms of negative selection have been previously proposed, which include eliminating, editing or silencing the autoreactive B cells, as elegantly demonstrated in the genetically modified mouse models.14–16 However, the key question remains how the clonal expansion of activated B cells happens while ignoring the negative selection mechanism in the physiologic condition, followed by differentiation into antibody-secreting plasma cells or germinal center B cells. Chan et al. have showed that the self-reactive germinal center B 12 cells were eliminated when the self-antigen was expressed ubiquitously or specifically in cells close to the germinal center environment.17 In contrast, those cells that bind to rare antigens survived probably by “positive selection” and antibody hypersomatic mutation, and were able to differentiate into plasma cells secreting high-affinity autoantibodies. These data clearly demonstrated that the landscape or microenvironment of autoreactive B cells, including the regulatory T cells, dendritic cells, and dose and time of self-antigen exposure, may be critical in pemphigus autoimmunity (Table 1). REGULATION OF AUTOANTIBODY SECRETION BY BREG Regulatory B cells (Breg) are a relatively newly identified subset of cells that have been shown to downregulate T-cell function, which were first described by Mizoguchi and Bhan in 2006.18 Although the exact mechanism requires further investigation, the inhibitory effects of Breg were shown to depend on production of cytokines including IL-10 and transforming growth factor (TGF)-b.19,20 In both animal models and human diseases, Breg have been shown to play a critical role in the development of autoimmune diseases such as SLE and multiple sclerosis. We recently found that the Breg function has been impaired in pemphigus patients. Strikingly, we found that the number of Breg is significantly increased in the blood of pemphigus patients with active disease compared with that in the remittent patients. However, the B cells from the patients were found to be able to secrete less IL-10 and be defective in suppressing interferon (IFN)-c secretion by the T-helper (Th)1 cells. Collectively, our results have demonstrated that impaired function of Breg may contribute to pemphigus pathogenesis by relieving its suppression on the autoreactive T cells via abnormal cytokine Table 1. Loss of T cell or B cell tolerance in pemphigus Cells Central tolerance Peripheral tolerance T cell Dsg3 expression T-cell receptor signaling AIRE Low Dsg3 exposure B-cell receptor signaling Self-antigen exposure Cytokines and signaling Foxp3 Inactivated T cell Antibody hypersomatic mutation HLA class II B cell Negative selection In pemphigus, autoantibody production requires both autoreactive T and B cells. Activation T or B cells may occur in the context of loss of central or peripheral tolerance. Although the mechanism is still unclear, T-cell self-tolerance is maintained by recognition of desmoglein (Dsg)3 (the autoantigen). At a low level, Dsg3 may inactivate the “natural” autoreactive T cells, while at a high level of Dsg3 or with a high-affinity receptor autoantibody T or B cells may undergo apoptosis by negative selection through the respective antigen receptors. The Dsg3 expression level is controlled by the transcriptional factor autoimmune regulator (AIRE). Likewise, loss of tolerance may also be controlled by self-antigen expression that can be regulated by the transcriptional factor FoxP3. T-cell tolerance is regulated by the signals directly (T regulatory cells) or indirectly (special cytokines) from other T cells. By contrast, loss of B cell tolerance is highly regulated by T cells and driven by somatic mutation of B cell antigen receptors (BCR). This regulation is presumably restricted by the pemphigus-specific HLA class II. © 2015 Japanese Dermatological Association Mechanism of autoantibody production in pemphigus production such as IL-10.19–21 When treated with rituximab, pemphigus patients with complete remission had a significantly higher number of IL-10-secreting regulatory B cells and much more IL-10 compared with those with no response and incomplete remission, suggesting a critical role of Breg in pemphigus.6 LOSS OF T-CELL SELF-TOLERANCE IN PEMPHIGUS Studies of healthy individuals with the PV-associated human leukocyte antigen (HLA) class II have shown that there exist Dsg3-specific T cells, which recognize the same epitopes of Dsg3 as those detected in pemphigus patients.22,23 Thus, both PV susceptibility HLA II alleles and break of T-cell tolerance are not sufficient to cause pathogenic antibody production. Yet, previous studies using animal models have clearly revealed that loss of T-cell tolerance was necessary for pemphigus pathogenesis.7 Therefore, it may be difficult to understand how the immune system breaks the T-cell tolerance in pemphigus. It appears that loss of central T-cell tolerance may occur in the thymus, which controls central tolerance by regulating the expression levels of self-antigens. One of the key transcription factors involved in this process is named autoimmune regulator (AIRE) and has been shown to be essential in controlling expression of nearly all the self-antigens, including Dsg3.24 The expression levels of Dsg3 in the thymus define the fate of T-cell development by certain immune mechanisms such as negative selection. Yet, evidence that supports a central tolerance mechanism in pemphigus remains extremely limited, although recent studies of the population markers on the Dsg3-specific IgM+ or IgG+ B cells in the patients before and after treatment with rituximab may have provided some clues.6 Nevertheless, loss of T-cell tolerance can also occur in the peripheries, where the CD4+ CD25+ regulatory T cells (Treg) may play a critical role. These Treg cells may mediate peripheral T-cell tolerance through Foxp3, a transcription factor whose deficiency leads to proliferation of autoreactive T cells and subsequent development of autoimmune diseases.25 Current studies have supported the suggestion that multiple Treg cells that can interact with autoreactive T and B cells may play a role in pemphigus (Fig. 1). From several clinical studies, it has been found that there is also genetic susceptibility to PV, showing a significant correlation between several HLA class II alleles (such as DRB1*04, DRB1*08 and DRB1*14) and the disease.23,26–28 Numerous polymorphisms of HLA-II have been identified throughout several populations of PV patients, as this susceptibility may be variable by ethnicity.26,29–31 Following binding to the self-antigen, Dsg3 is subsequently internalized and processed in the T cells before being presented together with the related HLA molecules to activate B cells for secretion of pathogenic autoantibodies. Very recently, in the humanized HLA-DRB1*04:02-transgenic mouse model, the HLADRB1*04:02-restricted CD4+ T cells that are specifically reactive to human Dsg3 epitopes were shown to produce pathogenic pemphigus IgG antibodies.32 © 2015 Japanese Dermatological Association Figure 1. Immune regulation of autoantibody production in pemphigus. T cells including T-helper (Th)1, (Th)2, Th17 and follicular T helper cells (Tfh) are presented with desmogleins (Dsg), the autoantigen in pemphigus. This process is restricted by human leukocyte antigen (HLA) II, such as DRB1*04, DRB1*08 and DRB1*14. Upon activation, the T cells may subsequently activate the B cells by direct interaction or secretion of cytokines. These cytokines are critical in regulation of B-cell function, and can negatively (dotted arrow) or positively (solid arrow) regulate activation of autoreactive B cells. The B cells can further mature and develop into plasma cells, which secrete high-affinity autoantibodies against Dsg3. APC, antigen-presenting cells; IFN, interferon; IL, interleukin; nTreg, natural regulatory T cells. T-CELL REGULATION OF AUTOANTIBODY PRODUCTION IN PEMPHIGUS Regulation by Th1 and Th2 cells Desmoglein autoantibody production and immune-mediated regulation of T-cell subsets are two inseparable steps in pemphigus development. Th2 response has been implicated to play a critical role in the pathogenesis of pemphigus, as evidenced by the fact that in the patients, the levels of Th2 cytokines (IL-4 and IL-10) were significantly elevated and Th1 cytokines (IL-2 and IFN-c) were significantly decreased as compared with healthy controls.33 Results from our studies showed that Th2 polarization is associated with the disease activation,34 in which the ratio of Th1/Th2 was significantly lower in the active stage as compared with the remission stage. By contrast, D’Auria et al. reported that there was no significant elevation of the Th2 cytokines in pemphigus patients compared with healthy controls.35 Because B-cell activation and antibody production classically necessitate the involvement of CD4+ T cells, Dsg-reactive T cells were capable of recognizing multiple epitopes of the extracellular domain of Dsg and helping B cells to produce a specific antibody. Previous studies have shown the presence of Dsg3-reactive T cells in the peripheral blood of PV patients.22,23,36 Dsg3-reactive T-cell clones were able to commit polyclonal na€ıve B cells to produce pathogenic anti-Dsg3 antibody and induce the PV phenotype. The Th1 and Th2 cell recognition of Dsg3 peptides is restricted by HLA-DRb1*0402 and/or HLA-DQb1*0503, and 13 M. Pan et al. the proliferative response of the autoreactive Th cells can be blocked by anti-DR and anti-DQ antibodies, respectively.23,27,28 A majority of studies confirmed the important role of Dsg-reactive Th2 cells in pathogenesis of pemphigus. Veldman et al.37 found that there is a predominance of autoreactive Dsg3-reactive Th1 cells in healthy individuals and Dsg3-reactive Th2 cells in PV patients. However, Dsg3-reactive Th2 cells are detected at similar frequencies in acute onset, chronic active and remittent PV, while the number of autoreactive Th1 cells exceeds that of Th2 cells in chronic active PV. Furthermore, Rizzo C et al. found this Dsg3-specific Th2 activity was significantly correlated with the Dsg-3 antibody titer,38 which has previously been shown to correlate with disease activity.39,40 This underscores the notion that B cells require activation by Dsg-specific Th2 cells in order to trigger production of pemphigus autoantibodies, ultimately causing the disease (Fig. 1). The Dsg-specific antibody subclasses are considered to be more related to the disease activation. In both PV and PF, patients with active disease demonstrate Dsg-reactive IgG4 and IgG1, while patients in remission and some healthy relatives of patients can demonstrate only anti-Dsg IgG1 subclass.41 We also observed that specific IgG1 was the major component of the serum specific antibody in stable PV patients, while IgG4 anti-Dsg were dominant in the active stage and that there seemed to be a strong association between an increase in IgG4 anti-Dsg levels and the severity of clinical activity.34 This suggests that specific Dsg IgG4 is the major pathogenic antibody subclass, playing a more important role in causing acantholysis in pemphigus patients. However, there is a dichotomy of Dsg-specific antibody subclass distribution in pemphigus patients. David et al. showed that among pemphigus patients with active disease, IgG1 was found in all of them and IgG4 in 85%, while IgG2 and IgG3 were found only in 54% and 77% of the patients, respectively.42 For patients in remission, the most common subclass was IgG4, found in 79% of patients. They concluded that IgG1 and IgG4 are predominant among patients with active lesions. Because T-cell helper signals such as cytokines and co-stimulatory molecules are responsible for Ig isotype switching, such as Th1 cytokines (such as IFN-c) able to induce the secretion of IgG1 and IgG2, whereas the IgG4 and IgE subtypes are mediated by Th2 activation.43,44 The antibody profile of anti-Dsg antibodies of IgG1, IgG4 and IgE isotype is involved in the balance of Th1/Th2 polarization. Also, Dsg-IgG4, the major pathogenic subtypes of Dsg-specific IgG in PV, is thus assumed to be regulated by the Dsg-specific Th2 cells. In our previous study, we showed that Dsg3 IgG1 production in mice (similar to human IgG4) is Th2 cell dependent,34 consistent with our clinical findings about Th2-biased and IgG4-dominant anti-Dsg3 autoantibody response in an active group of PV patients. Our results support the hypothesis that Dsg3-reactive Th2 cells are responsible for providing help for pathogenic IgG4 subclass production in pemphigus patients. Given the association between specific IgG4 in active disease and IgG1 in pemphigus remission, current evidence tends to imply that active disease showed a dominant Th2 response while patients in clinical remission displayed Th1 dominance. 14 Regulation by Tfh cells Follicular T helper cells (Tfh) are a recently discovered group of CD4+ Th cells with intrinsic differences from previously characterized Th1, Th2 and Th17 cells. Localized in B-cell follicles of secondary lymphoid tissues, Tfh cells are characterized by the high-level expression of cell surface markers including CXCR5 controlling migration of Tfh cells towards the B-cell follicles, programmed cell death-1 (PD-1), and inducible T-cell co-stimulator (ICOS), as well as transcription factor B-cell lymphoma 6 (BCL-6).45 The major function of Tfh cells appears to help B-cell activation and antibody production during humoral immune responses. Tfh-cells dysregulation has been also associated with the development of autoimmune diseases, such as the systemic lupus erythematosus (SLE) model.46,47 The Tfh cells express high levels of IL-21, which was demonstrated to be important for the generation of Tfh cells and that responsiveness of Tfh cells to IL-21 drives the formation of the germinal center reaction, and it clearly impacted on the amount of antibody production.48 Moreover, IL-21 contributes to development of a number of autoimmune diseases in the animal models of SLE, experimental autoimmune encephalomyelitis and rheumatoid arthritis.49,50 At least six different Tfh-cell subsets have been indentified, according to their surface markers and/or anatomical locations.51 Significantly, Tfh memory cells reside in the lymph nodes and regulate the memory B-cell response for long-term immunity.52 In humans, most of the Tfh cells located in the light zone of germinal center are CD4+CXCR5+CD57+CD69+ cells. Recently, Simpson et al. reported a “circulating Tfh” subset with characterized phenotype of CD4+CXCR5+ICOShigh PD-1high.53 The report showed that a population resembling Tfh cells can € gren’s syndrome patients and that be detected in SLE and Sjo the presence of this population correlated with the increased diversity and titer of autoantibodies and severity of end-organ involvement. However, the role of Tfh cells in the production of anti-Dsg antibody in pemphigus has not been elucidated. In our study, we found that the ratio of circulating Tfh was significantly increased more in PV patients than that in healthy controls (data not shown), but further studies are needed to determine whether Tfh cells initiate autoantibody production in PV and to clarify the mechanisms involved (Fig. 1). Dysregulation of Th17/Treg balance T-helper 17 cells are a recently discovered T-cell group with intrinsic differences from previously characterized Th1 and Th2 cells. They are characterized by the production of cytokines such as IL-17A (also called IL-17), IL-17F and IL-22 and require a network of inflammatory cytokines for their own differentiation.54 In mice, TGF-b and IL-6 initiate the differentiation of Th17 cells and activate the key transcription factor, retinoidrelated orphan receptor (ROR)ct. Then, they are amplified by IL-21 and expanded and maintained by IL-23. In humans, the differentiation is initiated by TGF-b and IL-21 that induce the transcription factor RORc. IL-1b and IL-6 are important to enhance the amplification of Th17 cells and IL-23 to maintain the Th17 cell population.55 Th17 cells protect against fungal © 2015 Japanese Dermatological Association Mechanism of autoantibody production in pemphigus and extracellular bacterial infections and participate in inflammatory reactions and autoimmunity. They can produce large quantities of IL-17A, and most Th17-mediated effects are attributed to this cytokine. In addition to IL-17A, Th17 cells coproduce IL-17F. They have similar effects on inducing the production of pro-inflammatory cytokines, chemokines and metalloproteinases from various tissues and cell types.56 Accumulating data suggest that Th17 cells play a significant role in infectious diseases, autoimmune conditions, adoptive immune response and mucosal immunity.57–59 Recent published work suggests that Th17 cells may be involved in the pathogenesis of PV. In 2009, Arakawa et al. found that the skin lesions from pemphigus patients expressed increased IL-17+ cells (Th17) by immunohistochemical staining.60 However, they failed to find a significant correlation between the Th17 cells and disease activity or anti-Dsg3 antibody titers, but proposed that perhaps increase of Th17 cells may not be a cause of the disease, rather a protective feedback in an attempt at maintaining homeostasis of the epithelial barrier. Cerrene et al. found that the serum IL-17 level was also elevated in pemphigus patients.61 Some researchers also found that serum IL-17 and IL-6 levels were elevated and serum IL-23 level was decreased.62 Recently, our group found that the Th17 cell population in pemphigus patients was significantly increased, when compared with the healthy controls. We also found that the Th17 cell was significantly elevated in patients of acute stage, suggesting that Th17 cells and IL-17 cytokines may have a certain correlation with disease activity.63 Researchers from Mexico reported a case of PV treated with ustekinumab (a human monoclonal antibody against IL-23).64 After one month of treatment, good clinical improvement was observed and serum IL-12, IL-17, IFN-c and IL-6 levels showed significant decrease. Joshi et al. examined the serum IL-17 and TGF-b levels of PV patients by enzyme-linked immunoassay and found that all the PV patients had elevated serum IL-17 levels, whereas it was not detectable in any healthy controls.65 The mean serum TGF-b concentration was also lower in patient sera as compared with healthy control, and the TGF-b/ IL-17 ratio was drastically reduced in patients. It was also reported that IL-17 cytokine secreted from Th17 cells can stimulate B-cell survival and activation, further facilitating antibody secretion in SLE patients.66 Some other reports showed that Th17 may need the help from B-cell activating factor (BAFF) for their functions on B cells.55,67 However, the correlation between the IL-17 population and anti-Dsg autoantibodies in pemphigus patients has not been found.63 The exact function of IL-17-producing Th cells in pemphigus is still unclear. However, it can be speculated that peripheral blood Th17 cells can migrate to the lesional sites where large amounts of inflammatory cytokines such as IL-17 and tumor necrosis factor-a were secreted. It is not clear if Th17 cells are the cause of the autoimmune mechanism or have a complimentary effect on pathogenic antibodies (Fig. 1). In addition, the elevated Th17 cells in pemphigus may simply be a result of disease activity, serving as a protective response to maintain the homeostasis of the epithelial barrier. More studies are needed to demonstrate the real importance of Th17/IL-17 as a new therapeutic target in PV. © 2015 Japanese Dermatological Association Regulatory T cells, as we mentioned above, belong to a subclass of lymphocytes that mediate negative regulatory mechanisms. They play a key role in the maintenance of self-tolerance and in the modulation of overall immune responses against infections and tumor cells. Treg secrete TGF-b and IL-10 and require the specific cytokine TGF-b and the transcription factor Foxp3 for differentiation. The suppression function of Treg is mediated by various mechanisms including cell–cell dependent; for example by expressing CTLA4 that is important to inhibit immune activation by competing for co-stimulatory ligands on T cells; and cell–cell independent mechanisms, such as secretion of inhibitory cytokines, IL-10 or TGF-b.68 Treg can be divided into two subgroups, natural Treg and inducible Treg according to the sites of their maturation. CD4+CD25+Foxp3+ natural Treg suppress the proliferation of naive T cells and their differentiation to effector T cells in vivo. They can also suppress effector activities of differentiated CD4+ and CD8+ T cells and the function of natural killer cells, natural killer T cells, B cells, macrophages, osteoclasts and dendritic cells. In several autoimmune diseases with aberrant antibody production, the function or number of Treg is impaired. Depletion of Treg can lead to abnormal antibody production. Furthermore, administration of Treg into autoimmune animals significantly reduced the autoantibody response.69 By far, a potential imbalance of CD4+CD25hi Treg has not been extensively investigated in pemphigus. Sugiyama et al. have revealed that the proportion of CD4+CD25hi Treg among total CD4+ T cells in the blood of PV patients was markedly reduced approximately 10-times less than that in the controls.70 They have also observed strikingly reduced gene expression as well as protein expression of Foxp3 in the blood CD4+CD25hi Tcell population of PV patients, which contain more CD4+CD25hi Treg, compared with that in normal controls. Severe reduction of Treg may be involved in breaking self-tolerance against Dsg in PV. However, Arakawa et al.60 found that in pemphigus patient’s skin lesion and normal human skin there are no Treg. Therefore, the authors speculated that reduction of Treg may be due to accumulation in skin or in lymph node drainage. Our group found that almost all the pemphigus patients have a lower number of Treg.63 Interestingly we found in the acute stage that the number of Treg was even lower. Therefore, we concluded that the Treg population was defective in pemphigus patients and thus cannot effectively inhibit function of effector T cells, resulting in a large amount of effector T-cell activation and proliferation, which may further activate B cells to produce autoantibodies in pemphigus (Fig. 1). The developmental pathways of Th17 and Treg are closely related. They may differentiate from the same precursor T cells, depending on the relative amount of cytokines present in their environment. TGF-b is a critical differentiation factor for the generation of Treg. Using mice with a reporter introduced into the endogenous Foxp3 locus, Bettelli et al. found that IL-6 completely inhibits the generation of Foxp3+ Treg induced by TGF-b.55 Also, combination of IL-6 and TGF-b promotes the generation of Th17 cells. The data suggest that there is not only a functional antagonism between Th17 and Treg but that there is a dichotomy in their generation as well. Therefore, Treg and Th17 effectors arise in a mutually exclusive fashion, depending 15 M. Pan et al. on whether they are activated in the presence of TGF-b or TGFb plus IL-6. At the steady-state level or in the absence of any inflammatory insult, TGF-b produced in the immune system will suppress the generation of effective T cells and induce Foxp3+ Treg, and thereby maintain self-tolerance. However, with infection or inflammation, IL-6 produced by the activated innate immune system will suppress the generation of TGF-b-induced Treg and induce a pro-inflammatory T-cell response predominated by Th17 cells.69 Therefore, the regulation of the Th17/ Treg balance appears critical in the development of autoimmune and inflammatory diseases. In pemphigus patients, the imbalanced expression of Th17 and Treg was observed and there was a significantly negative correlation between them.63 SUMMARY Pemphigus is a disease model of autoimmunity with identified autoantigen and autoantibodies. B cells break the self-tolerance to develop the pathogenic antibodies. During this utmost immune process, autoreactive T cells provide the activation signal for B-cell proliferation and maturation. Th2-biased cellular response was dominant in the disease development, especially in the acute stage, correlated with the antibody production and disease activity. Tfh cells could directly help B-cell activation, showing elevated ratio in the peripheral blood from the patients. However, the functional difference between circulating Tfh and marginal zone localized Tfh still needs to be further addressed. The balance of Th17/Treg was disrupted in pemphigus, sharing a significantly negative correlation. Besides these immunoreactive and regulatory cells, the cytokines, such as IL-10, IL-21, IL17 and TGF-b, comprise the microenvironmental regulatory network in the disease and are variable during the different disease stages. The combination of treatment by modulating the homeostasis of the key cytokines or active immune cells may lead to novel and effective immunotherapies for pemphigus and other autoimmune and inflammatory diseases. ACKNOWLEDGMENTS: We thank the National Natural Science Foundation of China for grant support (no. 81171499, 81472875) and the Milstein Medical Asian American Partnership Foundation for the Fellowship Award in Skin Disease. We thank Dr Xuming Mao (University of Pennsylvania) for critical reading and valuable suggestions during our manuscript preparation. CONFLICT OF INTEREST: None. REFERENCES 1 Payne AS, Ishii K, Kacir S et al. Genetic and functional characterization of human pemphigus vulgaris monoclonal autoantibodies isolated by phage display. J Clin Invest 2005; 115: 888–899. 2 Amagai M, Klaus-Kovtun V, Stanley JR. Autoantibodies against a novel epithelial cadherin in pemphigus vulgaris, a disease of cell adhesion. Cell 1991; 67: 869–877. 3 Amagai M, Karpati S, Prussick R et al. Autoantibodies against the amino-terminal cadherin-like binding domain of pemphigus vulgaris antigen are pathogenic. J Clin Invest 1992; 90: 919–926. 16 4 Amagai M, Hashimoto T, Shimizu N et al. Absorption of pathogenic autoantibodies by the extracellular domain of pemphigus vulgaris antigen (Dsg3) produced by baculovirus. Amagai M, Hashimoto T, Shimizu N, Nishikawa T. J Clin Invest 1994; 94(1): 59–67. ~a LY, Flores-Borja F et al. CD19(+)CD24(hi)CD38(hi) 5 Blair PA, Noren B cells exhibit regulatory capacity in healthy individuals but are functionally impaired in systemic Lupus Erythematosus patients. Immunity 2010; 32(1): 129–140. 6 Colliou N, Picard D, Caillot F et al. Long-term remissions of severe pemphigus after rituximab therapy are associated with prolonged failure of desmoglein B cell response. Sci Transl Med 2013; 5: 175ra30. 7 Amagai M, Tsunoda K, Suzuki H et al. Use of autoantigen-knockout mice in developing an active autoimmune disease model for pemphigus. J Clin Invest 2000; 105: 625–631. 8 Cho MJ, Lo AS, Mao X et al. Shared VH1-46 gene usage by pemphigus vulgaris autoantibodies indicates common humoral immune responses among patients. Nat Commun 2014; 5: 4167. 9 Eming R, Nagel A, Wolff-Franke S et al. Rituximab exerts a dual effect in pemphigus vulgaris. J Invest Dermatol 2008; 128: 2850–2858. 10 Qian Y, Jeong JS, Maldonado M et al. Brazilian pemphigus foliaceus anti-desmoglein 1 autoantibodies cross-react with sand fly salivary LJM11 antigen. J Immunol 2012; 189: 1535–1539. 11 Yamagami J, Payne AS, Kacir S et al. Homologous regions of autoantibody heavy chain complementarity-determining region 3 (H-CDR3) in patients with pemphigus cause pathogenicity. J Clin Invest 2010; 120: 4111–4117. 12 Toumi A, Saleh MA, Yamagami J et al. Autoimmune reactivity against precursor form of desmogelin 1 in healthy Tunisians in the area of endemic pemphigus foliaceus. J Dermatol Sci 2013; 70(1): 19–25. 13 Wardemann H, Yurasov S, Scharfer A et al. Predominant autoantibody production by early human B cell precursors. Science 2003; 301: 1374–1377. 14 Goodnow CC. Transgenic mice and analysis of B-cell tolerance. Annu Rev Immunol 1992; 10: 489–518. 15 Nemazee D. Promotion and prevention of autoimmunity by B lymphocytes. Curr Opin Immunol 1993; 5: 866–872. 16 Nossal GJ. Negative selection of lymphocytes. Cell 1994; 76: 229– 239. 17 Chan TD, Wood K, Hermes JR et al. Elimination of germinal-centerderived self-reactive B cells is governed by the location and concentration of self-antigen. Immunity 2012; 37: 893–904. 18 Mizoguchi A, Bhan AK. A case for regulatory B cells. J Immunol 2006; 176: 705–710. 19 Noh J, Lee JH, Noh G et al. Characterisation of allergen-specific responses of IL-10-producing regulatory B cells (Br 1) in Cow Milk Allergy. Cell Immunol 2010; 264: 143–149. 20 Lee JH, Noh J, Noh G et al. Allergen-specific transforming growth factor-b-producing CD19+CD5+ regulatory B-cell (Br 3) responses in human late eczematous allergic reactions to cow’s milk. J Interferon Cytokine Res 2011; 31: 441–449. 21 Zhu HQ, Xu RC, Chen YY et al. Impaired function of CD19+ CD24hi CD38hi regulatory B cells in patients with pemphigus. Br J Dermatol 2014. doi: 10.1111/bjd.13192. 22 Hertl M, Amagai M, Sundaram H et al. Recognition of desmoglein 3 by autoreactive T cells in pemphigus vulgaris patients and normals. J Invest Dermatol 1998; 110: 62–66. 23 Veldman C, Eming R, Wolff-Franke S et al. Detection of low avidity desmoglein 3-reactive T cells in pemphigus vulgaris using HLA-DR beta 1*0402 tetramers. Clin Immunol 2007; 122: 330–337. 24 Wada N, Nishifuji K, Yamada T et al. Aire-dependent thymic expression of desmoglein 3, the autoantigen in pemphigus vulgaris, and its role in T-cell tolerance. J Invest Dermatol 2011; 131: 410–417. 25 Kim JM, Rasmussen JP, Rudensky AY. Regulatory T cells prevent catastrophic autoimmunity throughout the lifespan of mice. Nat Immunol 2007; 8: 191–197. 26 Yan L, Wang JM, Zeng K. Association between HLA-DRB1 polymorphisms and pemphigus vulgaris: a meta-analysis. Br J Dermatol 2012; 167: 768–777. © 2015 Japanese Dermatological Association Mechanism of autoantibody production in pemphigus € tzinger J, Hertl M. HLA class II restriction of autore27 Riechers R, Gro active T cell responses in pemphigus vulgaris: review of the literature and potential applications for the development of a specific immunotherapy. Autoimmunity 1999; 30: 183–196. 28 Gebhard KL, Veldman CM, Wassmuth R et al. Ex vivo analysis of desmoglein 1-responsive T-helper (Th) 1 and Th2 cells in patients with pemphigus foliaceus and healthy individuals. Exp Dermatol 2005; 14: 586–592. 29 Mortazavi H, Amirzargar AA, Esmaili N et al. Association of human leukocyte antigen class I antigens in Iranian patients with pemphigus vulgaris. J Dermatol 2013; 40: 244–248. 30 Orouji E, Tavakkol Afshari J, Schmieder A, Layegh P. HLA-DQB1 gene and pemphigus vulgaris in patients with Mid-East origin. J Dermatol Sci 2014; 76(2): 153–155. 31 Bhanusali DG, Sachdev A, Rahmanian A et al. HLA-E*0103X is associated with susceptibility to Pemphigus vulgaris. Exp Dermatol 2013; 22: 108–112. €cklund J et al. Pathogenic IgG antibodies 32 Eming R, Hennerici T, Ba against Desmoglein 3 in pemphigus vulgaris are regulated by HLADRB1*04:02-restricted T Cells. J Immunol 2014; 193(9): 4391–4399. 33 Satyam A, Khandpur S, Sharma VK et al. Involvement of T(H)1/T(H)2 cytokines in the pathogenesis of autoimmune skin disease-Pemphigus vulgaris. Immunol Invest 2009; 38: 498–509. 34 Zhu H, Chen Y, Zhou Y et al. Cognate Th2-B cell interaction is essential for the autoantibody production in pemphigus vulgaris. J Clin Immunol 2012; 32: 114–123. 35 D’Auria L, Bonifati C, Mussi A et al. Cytokines in the sera of patients with pemphigus vulgaris: interleukin-6 and tumour necrosis factoralpha levels are significantly increased as compared to healthy subjects and correlate with disease activity. Eur Cytokine Netw 1997; 8: 383–387. 36 Takahashi H, Kuwana M, Amagai M. A single heiper T cell clone is sufficient to commit polyclonal naive B cells to produce pathogenic IgG in experimental pemphogus vulgaris. J Immunol 2009; 182: 1740–1745. 37 Veldman C, Stauber A, Wassmuth R et al. Dichotomy of autoreactive Th1 and Th2 cell responses to desmoglein 3 in patients with pemphigus vulgaris (PV) and healthy carriers of PV-associated HLA class II alleles. J Immunol 2003; 170: 635–642. 38 Rizzo C, Fotino M, Zhang Y et al. Direct characterization of human T cells in pemphigus vulgaris reveals elevated autoantigen-specific Th2 activity in association with active disease. Clin Exp Dermatol 2005; 30: 535–540. 39 Daneshpazhooh M, Chams-Davatchi C, Khamesipour A et al. Desmoglein 1 and 3 enzyme-linked immunosorbent assay in Iranian patients with pemphigus vul garis: correlation with phenotype, severity, and disease activity. J Eur Acad Dermatol Venereol 2007; 21: 1319–1324. 40 Belloni-Fortina A, Faggion D, Pigozzi B et al. Detection of autoantibodies against recombinant desmoglein 1 and 3 molecules in patients with pemphigus vulgaris: correlation with disease extent at the time of diagnosis and during follow-up. Clin Dev Immunol 2009; 2009: 1–6. 41 Bhol K, Natarajan K, Nagarwalla N et al. Correlation of peptide specificity and IgG subclass with pathogenic and nonpathogenic autoantibodies in pemphigus vulgaris: a model for autoimmunity. Proc Natl Acad Sci U S A 1995; 92: 5239–5243. 42 David M, Katzenelson V, Hazaz B et al. Determination of IgG subclasses in patients with pemphigus with active disease and in remission. Arch Dermatol 1989; 125: 787–790. 43 Finkelman FD, Holmes J, Katona IM et al. Lymphokine control of in vivo immunoglobulin isotype selection. Annu Rev Immunol 1990; 8: 303–333. 44 Kotowicz K, Callard RE. Human immunoglobulin class and IgG subclass regulation: dual action of interleukin-4. Eur J Immunol 1993; 23: 2250–2256. mez-Martın D, Dıaz-Zamudio M, Romo-Tena J et al. Follicular 45 Go helper T cells poise immune responses to the development of autoimmune pathology. Autoimmun Rev 2011; 10: 325–330. © 2015 Japanese Dermatological Association 46 Dong W, Zhu P, Wang Y et al. Follicular helper T cells in systemic lupus erythematosus: a potential therapeutic target. Autoimmun Rev 2011; 10: 299–304. 47 Tsuji M, Komatsu N, Kawamoto S et al. Preferential generation of follicular B helper T cells from Foxp3+ T cells in gut Peyer’s patches. Science 2009; 323: 1488–1492. 48 Vogelzang A, McGuire HM, Yu D et al. A fundamental role for interleukin-21 in the generation of T follicular helper cells. Immunity 2008; 29(1): 127–137. 49 Leonard WJ, Spolski R. Interleukin-21: a modulator of lymphoid proliferation, apoptosis and differentiation. Nat Rev Immunol 2005; 5: 688–698. 50 Spolski R, Leonard WJ. Interleukin-21: basic biology and implications for cancer and autoimmunity. Annu Rev Immunol 2008; 26: 57–79. 51 Vinuesa CG, Cook MC, Angelucci C et al. A RING-type ubiquitin ligase family member required to repress follicular helper T cells and autoimmunity. Nature 2005; 435: 452–458. 52 Fazilleau N, Eisenbraun MD, Malherbe L et al. Lymphoid reservoirs of antigen-specific memory T helper cells. Nat Immunol 2007; 8: 753–761. 53 Simpson N, Gatenby PA, Wilson A et al. Expansion of circulating T cells resembling follicular helper T cells is a fixed phenotype that identifies a subset of severe systemic lupus erythematosus. Arthritis Rheum 2010; 62(1): 234–244. 54 Bettelli E, Korn T, Oukka M, Kuchroo VK. Induction and effector functions of T(H)17 cells. Nature 2008; 453: 1051–1057. 55 Bettelli E, Carrier Y, Gao W et al. Reciprocal developmental pathways for the generation of pathogenic effector TH17 and regulatory T cells. Nature 2006; 441: 235–238. 56 Miossec P, Korn T, Kuchroo VK. Interleukin-17 and type 17 helper T cells. N Engl J Med 2009; 361: 888–898. 57 Wilson NJ, Boniface K, Chan JR et al. Development, cytokine profile and function of human interleukin 17-producing helper T cells. Nat Immunol 2007; 8: 950–957. 58 Korn T, Bettelli E, Oukka M, Kuchroo VK. IL-17 and Th17 Cells. Annu Rev Immunol 2009; 27: 485–517. 59 Littman DR, Rudensky AY. Th17 and regulatory T cells in mediating and restraining inflammation. Cell 2010; 140: 845–858. 60 Arakawa M, Dainichi T, Yasumoto S, Hashimoto T. Lesional Th17 cells in pemphigus vulgaris and pemphigus foliaceus. J Dermatol Sci 2009; 53: 228–231. 61 Giordano CN, Sinha AA. Cytokine networks in Pemphigus vulgaris: An integrated viewpoint. Autoimmunity 2012; 45: 427–439. 62 Chen XD, Chen H, Su WT. Role of Th17 cells in patients with pemphigus vulgaris. J Tongji Univ. 2009; 30: 106–109. 63 Xu RC, Zhu HQ, Li WP et al. The imbalance of Th17 and regulatory T cells in pemphigus patients. Eur J Dermatol 2013; 23: 795–802. 64 Tirado-Sanchez A, Ponce-Olivera RM, Vazquez-Gonzalez D, Bonifaz A. Th-17 and the lack of efficacy of ustekinumab in pemphigus vulgaris. Dermatol Online J 2013; 19: 15. 65 Joshi N, Minz RW, Anand S, Parmar NV, Kanwar AJ. Vitamin D deficiency and lower TGF-beta/IL-17 ratio in a North Indian cohort of pemphigus vulgaris. BMC Res Notes 2014; 7: 536. 66 Harrington LE, Hatton RD, Mangan PR et al. Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat Immunol 2005; 6: 1123–1132. 67 Hickman-Brecks CL, Racz JL, Meyer DM, LaBranche TP, Allen PM. Th17 cells can provide B cell help in autoantibody induced arthritis. J Autoimmun 2011; 36: 65–75. 68 Wan YY, Flavell RA. TGF-beta and regulatory T cell in immunity and autoimmunity. J Clin Immunol 2008; 28: 647–659. 69 Lim HW, Hillsamer P, Banham AH, Kim CH. Cutting edge: direct suppression of B cells by CD4+ CD25+ regulatory T cells. J Immunol 2005; 175: 4180–4183. 70 Sugiyama H, Matsue H, Nagasaka A et al. CD4+CD25high regulatory T cells are markedly decreased in blood of patients with pemphigus vulgaris. Dermatology 2007; 214: 210–220. 17