Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Neonatal infection wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Sjögren syndrome wikipedia , lookup
DNA vaccination wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Infection control wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
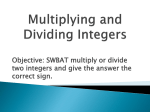
GASTROENTEROLOGY 2008;134:1470 –1481 The Characteristics of the Cell-Mediated Immune Response Identify Different Profiles of Occult Hepatitis B Virus Infection ALESSANDRO ZERBINI,* MASSIMO PILLI,* CAROLINA BONI,* PAOLA FISICARO,* AMALIA PENNA,* PAOLA DI VINCENZO,* TIZIANA GIUBERTI,* ALESSANDRA ORLANDINI,* GIUSEPPINA RAFFA,‡ TERESA POLLICINO,‡ GIOVANNI RAIMONDO,‡ CARLO FERRARI,* and GABRIELE MISSALE* *Laboratory of Viral Immunopathology, Azienda Ospedaliero-Universitaria di Parma, Parma, Italy; and the ‡Laboratory of Molecular Biology and Hepatology, Department of Internal Medicine, University of Messina, Italy BASIC–LIVER, PANCREAS, AND BILIARY TRACT Background& Aims: Hepatitis B virus (HBV) DNA detection in serum and/or in the liver of hepatitis B surface antigen (HBsAg)-negative patients with or without serologic markers of previous viral exposure is defined as occult HBV infection. Because the role of the adaptive response in keeping HBV replication under control in occult infection still is undefined, this study was performed to characterize the features of the HBV-specific T-cell response in this condition. Methods: HBV-specific T-cell frequency and function were tested ex vivo and after in vitro expansion in 32 HBsAg-negative patients undergoing diagnostic liver biopsy for chronic hepatitis C: 18 with occult HBV infection (11 anti-HBc–negative and 7 anti-HBc–positive patients) defined by the detection of intrahepatic HBV DNA by polymerase chain reaction; 14 without detectable intrahepatic HBV DNA (5 anti-HBc–positive and 9 anti-HBc–negative patients). Six patients with chronic hepatitis B and 7 HBsAg-inactive carriers were studied for comparison. Results: The presence or absence of serologic HBV markers defined 2 profiles of HBV-specific T-cell responses in occult infection. Anti-HBc–positive patients showed a T-cell response typical of protective memory, suggesting that this condition represents a resolved infection with immune-mediated virus control. In contrast, HBV-specific T cells in anti-HBc–negative patients did not readily expand and produce interferon-␥ in vitro, suggesting the possibility of a low-dose infection insufficient to allow maturation of protective memory. Conclusions: Our results suggest different mechanisms of control of viral replication in seropositive and seronegative occult infections. Additional studies aimed at understanding possible different clinical implications are needed. O ne of the fundamental steps of the hepatitis B virus (HBV) life cycle is the conversion of the 3.2-Kb relaxed circular DNA in a covalently closed-circular DNA in the nucleus of the infected hepatocyte, where it then is conjugated with nuclear proteins forming a minichromosome. Covalently closed-circular DNA is the template for transcription leading to the production of new infectious virions in the infected cell. The highly stable covalently closed-circular DNA, resistant to cell enzymes digestion, is probably the basis for life persistence of HBV infection, even after complete clinical recovery from acute hepatitis B.1 Thus, an overt HBV infection can persist in association with a chronic active or inactive disease with the presence of hepatitis B surface antigen (HBsAg) in the serum, but HBV also can persist decades after acute hepatitis along with a readily detectable memory T-cell response,2,3 despite a profound down-regulation of HBV gene expression4 – 6 under the effect of the protective antiviral immune response. This type of condition with persistence of minute amounts of virus in the liver and/or serum and with possible detection of HBV DNA also in peripheral blood mononuclear cells (PBMCs) likely can be identified with the so-called occult HBV infection and it generally is characterized by the presence of serum anti-HBV antibodies. However, occult infection with negative HBsAg can be present also in completely seronegative patients.7 The lack of HBsAg detection in occult infections may depend on mutations in the “a” determinant, but this condition only accounts for a minority of cases in the Mediterranean area and recent studies tend to exclude that HBV genetic mutations are responsible for the strong suppression of viral replication typical of occult HBV infection.8 Several other mechanisms could be involved, such as viral interference by other viruses, including hepatitis C virus (HCV), down-regulation of HBV gene expression by an undefined cellular mechanism, and virus control by the adaptive T-cell response. In the clinical setting, occult HBV infection represents not only a condition at risk of HBV reactivation, but it is also a cofactor of liver disease progression and hepatoAbbreviations used in this paper: CH-B, chronic hepatitis B; CH-C, chronic hepatitis C; ELISPOT, enzyme-linked immunosorbent spot; FITC, fluorescein isothiocyanate; IFN, interferon; IL, interleukin; PBMCs, peripheral blood mononuclear cells; PCR, polymerase chain reaction. © 2008 by the AGA Institute 0016-5085/08/$34.00 doi:10.1053/j.gastro.2008.02.017 carcinogenesis in patients with chronic HCV infection.9 –12 Moreover, outcome of interferon (IFN) treatment for chronic HCV infection could be influenced by the concomitant presence of occult HBV infection, even if definitive conclusions have not been achieved.9,10,13–17 To elucidate the possible pathogenetic mechanisms responsible for occult HBV infection, we have analyzed the features of the HBV-specific cell-mediated immune response in completely seronegative and in anti-HBc– positive patients with occult HBV infection. Results show different profiles of T-cell responses according to the serologic status of occult infection. Materials and Methods Patients A total of 78 patients with chronic HCV infection undergoing liver biopsy before IFN treatment and without evidence of chronic HBV infection (HBsAg negative) were enrolled at the Unit of Infectious Diseases and Hepatology of the Azienda Ospedaliero-Universitaria of Parma (Italy). Among these 78 patients, 18 subjects were positive for intrahepatic HBV DNA (Table 1, patients 1–18). HBVspecific HLA class I and class II restricted T-cell responses were studied in these 18 subjects and also in 5 anti-HBc– positive patients negative for intrahepatic HBV DNA (Table 1, patients 19 –23) and in 9 chronic hepatitis C (CH-C) patients negative for HBV serum markers and for intrahepatic HBV DNA (Table 1, patients 37– 45). The latter were selected randomly (first available patients) from the overall group of the 60 CH-C patients negative for intrahepatic HBV DNA. Liver histology of CH-C patients with and without occult HBV infection also is shown in Table 1. Six anti-HCV–negative, highly viremic (HBV-DNA level, ⬎105 copies/mL), anti-HBe–positive patients and 7 anti-HCV–negative, HBsAg-inactive carriers (HBV-DNA level, ⬍104 copies/mL) were studied for comparison. All patients were anti– human immunodeficiency virus negative. This study was approved by the Ethical Committee of the Azienda Ospedaliero-Universitaria of Parma, and all subjects gave written informed consent. HBV-DNA Analyses DNA was extracted from the frozen liver specimens and the PBMCs by standard procedures, as described in the supplementary material (see supplementary materials and methods online at www.gastrojournal.org). Occult HBV infection was identified as previously described with slight modification.11 All liver and PBMC DNA extracts were analyzed for the presence of HBV genomes by performing 4 different in-house single-step or nested polymerase chain reaction (PCR) amplification assays to detect preS-S, precore-core, Pol, T–CELL RESPONSE IN OCCULT HBV INFECTION 1471 and X regions. A sample was scored as HBV-DNA positive when amplification products were detected using at least 2 different sets of primers in 2 or more independent experiments. Moreover, direct sequencing of all amplified HBV products confirmed the specificity of the reactions. All negative cases were tested twice. In each PCR experiment, the following were included as negative controls: (1) serum and tissue DNA extracts from subjects known to be negative for HBV infection, (2) DNA-free reaction buffer, and (3) water. The limit of sensitivity of our single-step and nested PCR methods was in the range of 103 and 10 genome equivalents/mL, respectively, which approximately correspond to 2–200 IU/mL. Serum HBV DNA was quantified by the COBAS TaqMan Hepatitis B Virus Test (Roche Diagnostics, Mannheim, Germany). Detection of Amplification Products by Southern Blotting The PCR products were separated on a 1% agarose gel and transferred onto a nylon Hybond N⫹ membrane (Amersham, Buckinghamshire, England). The membrane was hybridized at 65°C overnight with a 32P random prime-labeled (Amersham) full-length HBV genome probe and then was washed and exposed to X-Omat film (Kodak, Rochester, NY) at ⫺80°C. Analysis of the Entire PreC-C Genomic Region of HBV DNA by PCR and Direct Sequencing Liver DNA extracts from a selected number of subjects were amplified by a nested PCR technique using oligonucleotide primers specific for HBV-DNA sequences flanking the entire preC-C genomic region and the Expand High Fidelity PCR System (Roche Diagnostics) according to the manufacturer’s instructions. Technical details are reported in the supplementary material (see supplementary materials and methods online at www.gastrojournal .org). Synthetic Peptides, Peptide-HLA Class I Tetramers, and Antibodies A panel of 315 peptides (15-mer) overlapping by 10 residues and covering the overall sequence of HBV genotype D were purchased from Chiron Mimotopes (Victoria, Australia). Fifteen-mer peptides were pooled in 16 mixtures (supplementary Table 1; see supplementary material online at www.gastrojournal.org). Recombinant S protein (Glaxo Smith Kline, Uxbridge, UK) and pre-S1 and pre-S2 polypeptides (Merck Sharp & Dohme, Whitehouse Station, NJ) also were used for the ex vivo enzyme-linked immunosorbent spot (ELISPOT) assay. Phycoerythrin-labeled tetrameric peptideHLA class I complexes, representing the HLA-A2 restricted epitopes HBV core 18 –27 (FLPSDFFPSV), BASIC–LIVER, PANCREAS, AND BILIARY TRACT May 2008 1472 ZERBINI ET AL GASTROENTEROLOGY Vol. 134, No. 5 Table 1. Patient Characteristics Patient Age Sex HBsAg BASIC–LIVER, PANCREAS, AND BILIARY TRACT HBsAg-negative/anti-HBc–negative 1 38 M Neg 2 61 M Neg 3 65 F Neg 4 63 F Neg 5 56 F Neg 6 28 M Neg 7 38 M Neg 8 52 M Neg 9 41 M Neg 10 61 M Neg 11 54 F Neg HBsAg-negative/anti-HBc–positive 12 65 F Neg 13 57 F Neg 14 52 M Neg 15 63 F Neg 16 38 M Neg 17 47 F Neg 18 39 M Neg 19 39 M Neg 20 66 F Neg 21 64 F Neg 22 49 M Neg 23 40 M Neg HBsAg-inactive carriers 24 58 F Pos 25 54 F Pos 26 48 M Pos 27 73 F Pos 28 49 M Pos 29 64 F Pos 30 40 M Pos CH-B 31 63 M Pos 32 31 F Pos 33 56 M Pos 34 45 M Pos 35 55 M Pos 36 57 F Pos CH-C 37 56 F Neg 38 49 F Neg 39 44 M Neg 40 61 F Neg 41 44 F Neg 42 57 F Neg 43 45 F Neg 44 44 M Neg 45 42 M Neg PBMCs HBV DNA Liver HBV DNA HCV antibody HLA-A2 Liver histology S/Ga ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 UI/mL UI/mL UI/mL UI/mL ND UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL Neg Neg Neg Neg ND Neg ND Neg Neg Neg Neg Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Neg Pos Pos Neg Pos Pos Neg Pos Neg Pos Pos I/I III/I III/I III/II I/I II/II II/II II/II 0/I II/II III/I Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 ⬍6 UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL UI/mL ND Neg Neg Neg Neg Neg ND Neg Neg Neg ND Neg Pos Pos Pos Pos Pos Pos Pos Neg Neg Neg Neg Neg Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Pos Neg Neg Neg Pos Pos. Neg Pos Pos Neg Neg Neg Pos II/II II/II I/I II/II I/I I/I III/II I/I II/II II/II I/I III/II Neg Neg Neg Neg Neg Neg Pos Pos Pos Pos Pos Pos Pos Pos 705 UI/mL 8740 UI/mL 1910 UI/mL 300 UI/mL 60 UI/mL 7740 UI/mL 1130 UI/mL NA NA NA NA NA NA NA NA NA NA NA NA NA NA Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Pos Neg Pos NA NA NA NA NA NA NA Neg Neg Neg Neg Neg Neg Pos Pos Pos Pos Pos Pos 597,000 UI/mL 2,700,000 UI/mL 77,100,000 UI/mL 1,180,000 UI/mL 968,000 UI/mL 1,410,000 UI/mL NA NA NA NA NA NA NA NA NA NA NA NA Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg NA NA NA NA NA NA Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg ND ND ND ND ND ND ND ND ND Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Pos Pos Pos Pos Pos Pos Pos Pos Pos Neg Pos Neg Neg Neg Pos Neg Neg Neg 0/I I/I ND/I II/II III/II I/I I/I III/II I/I HBsAb HBcAb Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Neg Pos Pos Pos Pos Neg Pos Pos Pos Pos Neg Neg Serum HBV DNA ⬍6 ⬍6 ⬍6 ⬍6 Neg, negative; Pos, positive; ND, not determined. aS/G staging and grading according to Sheuer histologic score. envelope 183–191 (FLLTRILTI), envelope 335–343 (WLSLLVPFV), envelope 348 –357 (GLSPTVWLSV), polymerase 575–583 (FLLSLGIHL), polymerase 816 – 824 (SLYADSPSV) of genotype D, and the corresponding synthetic peptides were purchased from Proimmune (Oxford, UK) and from Beckman-Coulter, Inc (Fullerton, CA). Moreover, for phenotypic and functional characterization of HBV-specific T cells, anti-CD8 peridinin chlorophyll protein-labeled (PerCP) or allophycocyanin-labeled (APC), anti-CD3 PerCP, anti-CD4 phycoerytrin-labeled (PE), anti-CD107a phycoerytrin Cy5-labeled, anti-perforin fluorescein isothiocyanate (FITC), anti–program death 1 (PD-1) FITC, anti-CD127, goat anti-mouse FITC or APC (BD Biosciences–Pharmingen, San Jose, CA), anti–IFN-␥–FITC (Sigma–Aldrich, St Louis, MO) were used. In Vitro Expansion of HBV-Specific T Cells For CD8 expansion, PBMCs of HLA-A2–positive patients were cultured with interleukin (IL)-7 (5 ng/mL) and IL-12 (100 pg/mL) at a concentration of 2 ⫻ 106/mL, seeded at 200 L/well in 96-well plates, and stimulated with HLA-A2–restricted HBV peptides at 1 mol/L final concentration. Recombinant IL-2 (50 IU/mL) was added on day 3 of culture, and the immunologic assays were performed on day 10. For PBMC stimulation with overlapping 15-mer peptides covering the overall HBV sequence, only IL-2 was added at day 3. Cell Surface and Intracellular Staining Staining with tetramers and other surface markers. PBMCs, either freshly isolated or after in vitro ex- pansion for 10 days, were stained with PE-labeled tetramers. Tetramer-positive responses are reported as a percentage of tetramer-positive T cells on total CD8 population. Frequencies of tetramer-positive CD8 cells 0.01% or greater were considered positive. This threshold was determined as the background signal plus 3 SD after staining PBMCs from 5 HLA-A2–positive healthy uninfected controls. Perforin staining. Tetramer-CD8 –stained cells were fixed and permeabilized with Fix and Perm (Caltag Laboratories, Burlington, CA) buffer in the presence of antiperforin FITC. The cells were washed and immediately analyzed by flow cytometry. IFN-␥ staining. Cells were incubated in medium alone (unstimulated control) or with viral peptides (1 mol/L) for 1 hour; brefeldin A (10 g/mL) was added for an additional 15 hours of incubation. At the end of the incubation, the cells were stained with tetramers, anti-CD8 PerCP, and CD4-PE for 30 minutes at 4°C, and then fixed and permeabilized in the presence of anti– IFN-␥ FITC. Finally, cells were washed and analyzed by flow cytometry. Degranulation experiments. For CD107a staining, the specific antibody was added to effector CD8 cells at the beginning of the incubation time with or without the relevant peptide. Staining with tetramers, anti-CD3, and anti-CD8 was performed 2 hours later. The degranulation capacity of the antigen-specific cytotoxic T lymphocytes was expressed as the frequency of CD107a-positive cells. ELISPOT Assay ELISPOT assays were performed using the panel of 315 peptides (15-mer) pooled in 16 mixtures. HBVspecific T-cell responses were analyzed after overnight incubation with individual peptide mixtures of either PBMCs (ex vivo analysis) or short-term polyclonal T-cell lines previously expanded in vitro by 10 days’ stimulation T–CELL RESPONSE IN OCCULT HBV INFECTION 1473 with the same peptide mixtures used for the ELISPOT assay (in vitro analysis). Technical details are reported in the supplementary material (see supplementary materials and methods online at www.gastrojournal.org). Statistical Analysis Statistical analysis of mean spot-forming units and frequencies of positive T-cell responses generated by ELISPOT assay were compared by t test for unpaired data and by chi-square analysis, respectively. The mean of IFN-␥ positive in vitro expanded CD4 and CD8 cells also were compared by t test for unpaired data. A P value of less than .05 was considered significant. Results Identification of Occult HBV Infection Intrahepatic HBV DNA was analyzed in 78 HBsAg-negative patients with CH-C who underwent liver biopsy for IFN/ribavirin treatment. Eighteen of them (23%) were positive for HBV DNA by nested PCR on at least 2 different HBV genomic regions and confirmed by sequencing of the amplified DNA fragments. Eleven of the 18 patients with occult HBV infection were negative for serum anti-HBV antibodies (anti-HBs and anti-HBc), whereas the remaining 7 patients were seropositive for anti-HBc and 5 of them also for anti-HBs (Table 1). Age and sex distribution within the groups of patients with and without occult HBV infection were similar. Prevalence of occult HBV infection in our cohort of CH-C was in line with previously published results on patients from similar geographic areas.9,11 Among the 60 CH-C patients negative for intrahepatic HBV DNA, 5 anti-HBc–positive and 9 seronegative subjects were studied for comparison (Table 1). The possible presence of HBV DNA in PBMC samples from 27 of the 32 patients tested for intrahepatic HBV DNA also was examined (Table 1). Nested PCR amplification and subsequent Southern blot analysis did not reveal occult HBV in any of the samples examined. Even if a sensitive methodologic approach was followed, the possibility that the lack of HBV-DNA detection was influenced by heparin traces should be considered because PBMCs were derived from heparinized blood. This possibility, however, does not cast doubts on the accuracy of patient selection because occult infection was defined by analysis of liver tissue. HBV-Specific T-Cell Responses Can Be Detected Ex Vivo in HBsAg-Negative Patients With Occult HBV Infection First, we asked whether a HBV-specific T-cell response is detectable in patients with occult HBV infection. To get a global representation of the overall T-cell response against HBV, HBV-specific T-cell responses were analyzed with a panel of 315 peptides (15-mer) covering BASIC–LIVER, PANCREAS, AND BILIARY TRACT May 2008 1474 ZERBINI ET AL GASTROENTEROLOGY Vol. 134, No. 5 BASIC–LIVER, PANCREAS, AND BILIARY TRACT Figure 1. Ex vivo IFN-␥ ELISPOT responses to individual HBV antigens in patients with and without occult HBV infection. (A) ELISPOT results obtained in the different patient populations are illustrated according to responses obtained by stimulation with HBV peptides spanning individual HBV regions (x, core, envelope, polymerase) and with recombinant envelope antigens corresponding to preS1, preS2, and S regions. (B) Comparisons of mean spots of the positive tests and frequency of positive responses (calculated on all tests) obtained in the different patients’ groups are presented: □, HBV-DNA positive and anti-HBc negative; , HBV-DNA positive and anti-HBc positive; □, HBV-DNA negative and anti-HBc positive; , CH-C. the whole HBV sequence of genotype D and also with recombinant HBV proteins expressing the preS1, preS2, and S envelope regions. Synthetic peptides were pooled in 18 mixtures, 2 of them covering the X region, 2 the core region, 4 the envelope region, and 8 the polymerase region. Peptide pools and recombinant proteins were used to stimulate PBMCs in an ELISPOT assay. By this approach, HBV-specific T cells were detected in patients with occult HBV infection at a frequency ranging between 30 and 120 specific T cells/106 PBMCs (supplementary Figure 1A and B; see supplementary material online at www.gastrojournal.org). The frequency of HBVspecific T cells did not differ between anti-HBc–positive and anti-HBc–negative subjects (Figure 1A and B). By the same methodologic approach we also tested 5 anti-HBc– positive CH-C patients negative for intrahepatic HBV DNA (supplementary Figure 1C and Figure 1A; see supplementary material online at www.gastrojournal.org) and 9 CH-C patients negative for HBV serum markers and for intrahepatic HBV DNA, as controls (Figure 1A and B). The mean values of spot-forming cells and the mean frequencies of positive responses detected in seronegative and seropositive patients with and without occult HBV infection were not significantly different, although no T-cell reactivity could be detected in the control group (Figure 1A and B). Interestingly, anti-HBc–negative patients with occult infection did not show T-cell responses to HBV core (peptide mixtures 3 and 4; supplementary Figure 1A and Figure 1A; see supplementary material online at www.gastrojournal.org), whereas 4 of 6 anti-HBc–positive subjects with occult HBV infection (supplementary Figure 1B; see supplementary material online at www.gastrojournal.org; and Figure 1A) and 2 of 5 anti-HBc–positive subjects with undetectable intrahepatic HBV-DNA (supplementary Figure 1C; see supplementary material online at www.gastrojournal.org; and Figure 1A) displayed T-cell reactivity to the peptide pools representing the HBV core region. HBV-specific T-cell responses also were confirmed by intracellular IFN-␥ staining in 2 anti-HBc–negative patients with occult infection from whom a sufficient number of frozen PBMCs was available (patients 7 and 8) (supplementary Figure 2; see supplementary material online at www.gastrojournal.org), showing a CD4-mediated T-cell response directed to envelope (patient 7) and to polymerase (patient 8) sequences. Ex Vivo Frequencies of HBV-Specific T Cells Are Comparable in Patients With Occult Infection and Inactive HBsAg Carriers The ELISPOT results obtained in patients with occult HBV infection also were compared with T-cell responses generated with the same peptides and HBV envelope antigens in 7 inactive HBsAg carriers (HBVDNA level, ⬍104 copies/mL) and in 6 anti-HBe–positive patients with chronic hepatitis B (CH-B) (viral load, ⬎105 copies/mL). Inactive carriers showed frequencies of circulating HBV-specific T cells similar to the patients with occult HBV infection (Figure 1A), whereas T-cell responses were almost undetectable in anti-HBe–positive CH-B patients (Figure 1A). HBV-Specific T-Cell Responses After In Vitro Expansion Are Different in Anti–HBcNegative and Anti–HBc-Positive Patients With Occult HBV Infection By the use of the same peptide pools, short-term T-cell lines were generated and tested in a culture ELISPOT. To confirm the positive tests, T-cell lines showing at least 1.5 times the number of spots obtained with medium were analyzed by intracellular IFN-␥ staining; this experimental approach also allowed identification of the T-cell subset responsible for the antigen-specific T-cell response. AntiHBc–positive subjects with or without detectable HBV DNA in the liver and inactive HBsAg carriers showed the most intense T-cell responses (Figure 2A), whereas lower levels of T-cell expansion, which was sustained mainly by CD4 cells, was detected in anti-HBc–negative patients with occult HBV infection and in anti-HBe–positive CH-B patients (Figure 2A). In agreement with ELISPOT results generated ex vivo, HBV core was the most immunogenic antigen for all patient groups with the exception of anti-HBc–negative pa- T–CELL RESPONSE IN OCCULT HBV INFECTION 1475 tients with occult HBV infection. Envelope-specific T-cell responses were almost totally undetectable in HBsAg-positive subjects. No HBV-specific T-cell expansion was observed in the control group, confirming the antigen specificity of the T-cell responses detected in the other patient groups (Figure 2A). HBV Tetramer Analysis Reveals the Presence of Functional Memory HBV-Specific CD8 Cells in Seropositive Patients With Occult Infection To analyze phenotypic and functional features of HBV-specific CD8 cells ex vivo and after short-term in vitro expansion in the different patient groups, 6 HLA-A2 tetramers containing HBV epitopes known to be recognized frequently in HBV infection were used to identify circulating HBV-specific CD8 cells. Seven patients with occult HBV infection (4 anti-HBc–negative and 3 antiHBc–positive), 2 anti-HBc–positive subjects negative for intrahepatic HBV DNA, and 2 HBsAg-inactive carriers were tested with HBV–HLA-A2 tetramers. Ex vivo analysis showed very low frequencies of circulating HBV-specific CD8 cells in the 7 anti-HBc–negative patients with occult infection that did not efficiently expand in vitro on peptide stimulation (Figure 2B). The low frequencies of tetramer-positive cells did not allow a reliable phenotypic analysis of HBV-specific CD8 cells in this patient group. Anti-HBc–positive subjects and HBsAg-inactive carriers showed the highest frequencies of HBV-specific CD8 cells, ranging from 0.01% up to 0.185% of the total CD8 population (Figures 2B and 3). Phenotypic analysis, performed on 4 anti-HBc–positive subjects (2 positive and 2 negative for intrahepatic HBV DNA) showed a prevalent memory phenotype characterized by the co-expression of CCR7 and CD127 on the majority (from 83% up to 100%) of HBV-specific CD8 cells, whereas PD-1 was expressed on a minor fraction of them (from 21% to 29%) (Table 2). Intracellular expression of perforin and granzyme also was very low (Figure 3 and Table 2), indicating a prevalent central memory phenotype.18 In vitro stimulation with specific peptides expanded HBV-specific CD8 cells very efficiently, generating T-cell lines containing up to 70% of tetramer-positive cells. Moreover, expanded CD8 cells were functional in terms of IFN-␥ secretion and cytotoxicity analyzed as surface CD107a up-regulation (Figure 3). In contrast to HBsAg-negative/anti-HBc–positive patients, ex vivo phenotypic analysis performed in HBsAginactive carriers showed a lower frequency of doublepositive CCR7/CD127 cells and a higher intracellular perforin and granzyme content (Figure 3). HBV-specific CD8 cells also expanded efficiently in these patients. Analysis of the Entire PreC-C Genomic Region of HBV DNA Because of the lack of core-specific T-cell responses in anti-HBc–negative patients with occult infec- BASIC–LIVER, PANCREAS, AND BILIARY TRACT May 2008 1476 ZERBINI ET AL GASTROENTEROLOGY Vol. 134, No. 5 BASIC–LIVER, PANCREAS, AND BILIARY TRACT Figure 2. Intensity of the HBV-specific CD4- and CD8-mediated T-cell reactivity. After 10 days of in vitro stimulation with the same peptide pools used for ex vivo analysis, expanded T cells were tested in a culture IFN-␥ ELISPOT assay. Tests showing at least 1.5-fold the number of spot-forming colonies obtained with medium were confirmed by IFN-␥ intracellular staining (rate of confirmation of the positive ELISPOT results ranging from 75% to 82% in the different patients’ groups). (A) Mean IFN-␥ production induced by HBV peptides is illustrated for patients with occult HBV infection negative or positive for anti-HBc, for patients positive for anti-HBc and negative for intrahepatic HBV-DNA, for HBsAg-inactive carriers, for anti-HBe–positive CH-B patients, and for CH-C patients negative for HBV serum markers and intrahepatic HBV DNA. Each bar in the upper part of A represents the mean percentage ⫾ standard error of IFN-␥–positive CD4⫹ and CD8⫹ cells reactive to all peptide mixtures representing each HBV antigen. Comparisons of mean frequencies of IFN-␥–positive CD4 and CD8 cells and frequencies of positive responses obtained in the different patient groups to all peptide pools is presented at the bottom. , CD8⫹; □, CD4⫹. (B) The sum of the frequencies of tetramer-positive CD8 cells measured ex vivo and after in vitro expansion in HLA-A2–positive patients is presented. Seven patients with occult HBV infection (4 anti-HBc– negative and 3 anti-HBc–positive patients), 2 anti-HBc–positive patients with undetectable intrahepatic HBV DNA, and 2 HBsAg-inactive carriers were studied. □, Ex vivo; , T-cell line. tion, in a selected number of subjects with a sufficient amount of liver-extracted DNA, preC-C genomic region sequencing was performed. Sequences derived from 3 anti-HBc–negative patients (patients 1, 3, and 7) were compared with sequences derived from 4 anti-HBc–positive patients (patients 12, 13, 15, and 16) all with occult HBV infection (Figure 4). HBV sequences derived from 6 patients were of genotype D, whereas the HBV sequence May 2008 T–CELL RESPONSE IN OCCULT HBV INFECTION 1477 Table 2. Phenotypic and Functional Analysis of Tetramer-Positive CD8 Cells Ex vivo Patient Epitope CCR7⫹/CD127⫹ PD1 Intrahepatic HBV-DNA–positive/anti-HBc–positive 16 ENV. 335–43 83% 21% ENV 183–191 ND ND Core 18–27 ND ND 18 Core 18–27 ND ND ENV 183–191 100% ND ENV. 335–43 100% 24% POL 816–24 ND ND Intrahepatic HBV-DNA–negative/anti-HBc–positive 19 ENV. 335–43 91% 26% 23 Core 18–27 93% 29% ENV. 335–43 ND ND HBsAg-positive inactive carriers 28 Core 18–27 69% 76% 30 Core 18–27 20% ND ENV. 335–43 ND ND POL 816–24 ND ND Short-term T-cell line Perforin⫹ granzyme B⫹ IFN-␥ ⫹ CD107a IFN-␥ ⫹ CD107a Perforin⫹ ND ND ND ND ND 0% ND ND ND ND ND ND 26% ND 65% 88% ND ND ND ND ND 89% 95% 96% 71% 95% 62% 53% 57% 33% ND 58.20% 88.10% 21.30% 52.30% 71% 64% ND 9% 21% 15% 53% 5% 0% ND ND 28% ND ND ND ND 73% 52% 80% ND ND ND ND 89% 95% 9% 26% ND ND 23% 5% ND ND ND ND ND ND 96% 98% 63% 27% ND ND ND ND 76.8% 98% 72% 78% BASIC–LIVER, PANCREAS, AND BILIARY TRACT NOTE. Percentages indicate the frequencies of tetramer-positive CD8 cells expressing the indicated phenotypic and functional parameters. ND, not determined. Figure 3. Phenotypic and functional profiles of tetramer-positive CD8 cells. Top panels illustrate percentages of HBV tetramer-positive CD8 lymphocytes with different specificities, analyzed ex vivo and after 10 days in vitro expansion in representative HBsAg-negative patients with and without occult HBV infection and in a HBsAg-inactive carrier. Lower panels illustrate the phenotypic and functional analysis of 3 representative patients (patient 18, occult⫹ anti-HBc⫹; patient 23, occult- anti-HBc⫹; patient 28, HBsAg⫹-inactive carrier). CD127, PD1, CCR7, perforin, and granzyme-B were tested ex vivo, whereas intracellular IFN-␥ and IL-2 expression as well as CD107a were tested after in vitro expansion. 1478 ZERBINI ET AL GASTROENTEROLOGY Vol. 134, No. 5 BASIC–LIVER, PANCREAS, AND BILIARY TRACT Figure 4. Sequencing of the entire preC-C genomic region in patients with occult HBV infection. Sequencing was performed in 3 anti-HBc–negative (patients 1, 3, and 7) and 4 anti-HBc–positive patients (patients 12, 13, 15, and 16). HBV sequences derived from 6 patients were aligned to a representative genotype D (GenBank accession number: V01460),19 whereas the HBV sequence derived from patient 12 was aligned to a representative genotype A (GenBank accession number: X02763).27 The number of variations over the 212 aligned amino acid residues is shown in parentheses for each patient. derived from patient 17 aligned to genotype A (Figure 4); none of the sequenced patients showed the G1896A mutation that determines a stop codon at position 28. AntiHBc–negative patient 3 with occult infection presented the highest number of AA variations (Figure 4). Overall, there was no dramatic increase in sequence variation in the pre-CC region that could explain the reduced T-cell reactivity to the core antigen in anti-HBc–negative patients. Discussion Occult HBV infection is defined by the persistence of HBV in the serum and/or within the liver in the absence of serum HBsAg. In this study, occult HBV infection was defined when at least 2 different HBV regions among preS-S, precore-core, Pol, and X were amplified by PCR on liver tissue. Although the prevalence of occult HBV infection in CH-C has been reported to be around 30%,7 the prevalence among the general population still is unknown. The natural history is partially understood because occult infection can represent the final outcome of a past resolved infection with persistence of viral sequences, which have not been cleared completely from the liver, or the result of a low-dose infection without liver cell injury and a partial induction or a total lack of humoral immunity. In the former scenario of occult infection in the context of a resolved hepatitis, initial priming of efficient HBV-specific T-cell responses, followed by generation of protective memory, is expected to occur. In the latter scenario of occult HBV resulting from a low-dose infection, whether a cell-mediated antiviral response is primed successfully and what type of response is mounted is totally undefined. To shed further light on the natural history and pathogenesis of occult HBV infection, we compared HBV-specific T-cell responses detected in patients with occult HBV infection with or without anti-HBc antibodies with those displayed by HBV-immune subjects (anti-HBc–positive without HBV DNA in the liver) and chronic HBV patients. In line with the possibility that in occult infection HBV replication is controlled by the cell-mediated immune response, our study shows the existence of an HBV-specific T-cell response in patients with occult HBV infection, even when serum HBV markers are completely negative. Several viruses, in particular DNA viruses and retroviruses, can be confined to different compartments most likely controlled by virus-specific T cells.20,21 In occult HBV infection, 2 different profiles of HBVspecific T-cell responses were displayed by patients with and without anti-HBc antibodies. Even if in seronegative patients with cryptic infection circulating HBV-specific T cells were detected at frequencies comparable with inactive HBsAg carriers and immune subjects (HBsAg negative, anti-HBc positive), in vitro expansion and IFN-␥ production by HBV-specific T cells was much weaker than in anti-HBc–positive patients with or without intrahepatic HBV DNA. Moreover, T-cell expansion almost completely was limited to the CD4 cell subset. The length of the peptides, although not optimal for CD8 cells, was suitable for CD8 recognition because CD8 cells were expanded readily in HBsAg-positive inactive carriers and in patients with acute HBV infection tested for comparison (data not shown). Thus, predominance of CD4mediated responses seems to be a feature of the immune response in these patients, rather than a technical artifact. In addition, the core antigen, which was the most immunogenic HBV antigen for the other groups of patients, was not recognized by T cells derived from seronegative occult patients. Even if sequencing was performed in only 3 anti-HBc–negative patients with occult T–CELL RESPONSE IN OCCULT HBV INFECTION 1479 HBV infection, this lack of recognition does not seem to be the result of mutations of the preC-C region. In contrast to seronegative occult patients, HBV-specific T cells were able to expand and to produce IFN-␥ efficiently in vitro in anti-HBc–positive subjects, either positive or negative for intrahepatic HBV DNA, with a phenotypic and functional profile of fully competent memory T cells, as confirmed also ex vivo by the high level of CD127 and CCR7 expression and the low rate of PD-1–positive cells. Trace amounts of virus have been reported in previous studies to persist even years after resolution of acute HBV infection,2,3 showing that clinical recovery does not imply complete HBV clearance but rather reflects the capacity of the immune system to keep under tight control minute amounts of virus that are expected to remain after clinical resolution of disease. If this is the case, the likelihood of detecting HBV DNA in liver and serum thus may vary over time in individual resolved acute infections in relation to the level of efficiency of immune control. These distinct behaviors of cell-mediated immune responses in seropositive and seronegative occult HBV infections may reflect different modalities of HBV transmission. As shown for the woodchuck HBV, exposure to low woodchuck HB doses (⬍103 virions) may give rise to a persistent infection without serum markers. Interestingly, this woodchuck primary occult infection does not confer protective immunity, suggesting that also in this animal model a functional memory T-cell response is generated only after infection with a higher dose of inoculum.22 Unfortunately, only a single study tried to characterize this type of HBV transmission in the chimpanzee model of infection. Human sera derived from subjects negative for serum HBV markers caused acute hepatitis when inoculated into 2 chimpanzees, one of which developed HBsAg and anti-HBc and the second one developed only anti-HBs.23 Immune responses, however, were not characterized and additional studies have not been reported in this animal model. Long-lasting memory CD4 and CD8 cell responses detectable several years after recovery from acute hepatitis B have been reported previously in anti-HBc–positive patients, with HBV-DNA traces in PBMCs and serum.2,3 In our study, ex vivo and in vitro T-cell responses in anti-HBc–positive subjects with or without HBV DNA in the liver were comparable. This supports the possibility that anti-HBc–positive occult infections represent the resolution phase of infections with high doses of virus that the immune system has been able to control efficiently with successful maturation of protective T-cell memory. The finding of a poor in vitro T-cell expansion in seronegative patients with occult infection raises questions about the mechanisms of control of HBV replication in this condition. Even if experimental data in support of this interpretation are lacking, we are tempted to BASIC–LIVER, PANCREAS, AND BILIARY TRACT May 2008 1480 ZERBINI ET AL BASIC–LIVER, PANCREAS, AND BILIARY TRACT speculate that control of the virus principally is the result of the innate immune response. This would limit liver cell damage and the release of inflammatory signals normally involved in activation and maturation of dendritic cells needed for massive expansion of CD4 and CD8 cell clones. In particular, the lack of CD8 cell expansion in seronegative patients could be the result of a dysfunctional CD4 response unable to expand and maintain memory CD8 cells. Moreover, a dysfunctional core-specific CD4 cell response also could provide insufficient T-cell help to core-specific B cells with a lack of detectable anti-HBc in the serum. An alternative hypothesis to explain virus control in these patients, which does not exclude the previous one, is that co-infection with HCV or other undefined hepatotropic viruses can interfere with HBV replication, as shown for HCV core protein,24 –26 and that T-cell responses specific for HCV or the other viruses can inhibit HBV replication through local release of cytokines, such as IFN-␥ and tumor necrosis factor-␣, able to affect virus replication by a nonspecific antiviral effect. In conclusion, in occult HBV infection different mechanisms have been proposed to explain why HBV remains mainly confined to the liver with only transient low levels of viremia. These include interference with HBV replication of concomitant viral infections, regulation of HBV gene transcription by cellular mechanisms, impaired replicative competence of HBV as a result of specific virus mutations, and control of HBV replication by the immune response. Our study supports this latter mechanism in anti-HBc–positive patients with occult infection who display features of HBV-specific T cells that are typical of protective memory. These HBV-specific T-cell responses are similar to those observed in resolved HBV infections, supporting the interpretation that anti-HBc– positive patients with or without detectable intrahepatic HBV DNA actually represent the same biological entity corresponding to patients with a prior resolved infection with variable efficiency of virus control. In contrast, the type of cell-mediated immune response in patients with occult infection associated with negative serum HBV markers suggests the possibility of a low-dose infection insufficient to allow maturation of an antiviral protective memory response. Additional studies are needed to understand whether the different immune responses and natural histories associated with the 2 types of occult infections suggested by our studies also have different clinical implications with respect to the development of hepatocellular carcinoma and responsiveness to antiviral therapy. Moreover, the new emerging protocols of immunosuppressive treatments for neoplastic, rheumatic, and hematologic disorders may have a different impact on HBV reactivation in seronegative and seropositive occult infections. GASTROENTEROLOGY Vol. 134, No. 5 Supplementary Data Note: To access the supplementary material accompanying this article, visit the online version of Gastroenterology at www.gastrojournal.org, and at doi: 10.1053/j.gastro.2008.02.017 References 1. Zoulim F. New insight on hepatitis B virus persistence from the study of intrahepatic viral cccDNA. J Hepatol 2005;42:302–308. 2. Penna A, Artini M, Cavalli A, et al. Long-lasting memory T-cell responses following self-limited acute hepatitis B. J Clin Invest 1996;98:1185–1194. 3. Rehermann B, Ferrari C, Pasquinelli C, et al. The hepatitis B virus persists for decades after patients’ recovery from acute viral hepatitis despite active maintenance of a cytotoxic T-lymphocyte response. Nat Med 1996;2:1104 –1108. 4. Chisari FV, Ferrari C. Hepatitis B virus immunopathology. Springer Semin Immunopathol 1995;17:261–281. 5. Guidotti LG, Ishikawa T, Hobbs MV, et al. Intracellular inactivation of the hepatitis B virus by cytotoxic T lymphocytes. Immunity 1996;4:25–36. 6. McClary H, Koch R, Chisari FV, et al. Relative sensitivity of hepatitis B virus and other hepatotropic viruses to the antiviral effects of cytokines. J Virol 2000;74:2255–2264. 7. Torbenson M, Thomas DL. Occult hepatitis B. Lancet Infect Dis 2002;2:479 – 486. 8. Pollicino T, Raffa G, Costantino L, et al. Molecular and functional analysis of occult hepatitis B virus isolates from patients with hepatocellular carcinoma. Hepatology 2007;45:277–285. 9. Cacciola I, Pollicino T, Squadrito G, et al. Occult hepatitis B virus infection in patients with chronic hepatitis C liver disease. N Engl J Med 1999;341:22–26. 10. De Maria N, Colantoni A, Friedlander L, et al. The impact of previous HBV infection on the course of chronic hepatitis C. Am J Gastroenterol 2000;95:3529 –3536. 11. Pollicino T, Squadrito G, Cerenzia G, et al. Hepatitis B virus maintains its pro-oncogenic properties in the case of occult HBV infection. Gastroenterology 2004;126:102–110. 12. Momosaki S, Nakashima Y, Kojiro M, et al. HBsAg-negative hepatitis B virus infections in hepatitis C virus-associated hepatocellular carcinoma. J Viral Hepat 2005;12:325–329. 13. Mrani S, Chemin I, Menouar K, et al. Occult HBV infection may represent a major risk factor of non-response to antiviral therapy of chronic hepatitis C. J Med Virol 2007;79:1075–1081. 14. Fukuda R, Ishimura N, Niigaki M, et al. Serologically silent hepatitis B virus coinfection in patients with hepatitis C virus-associated chronic liver disease: clinical and virological significance. J Med Virol 1999;58:201–207. 15. Sagnelli E, Coppola N, Scolastico C, et al. Isolated anti-HBc in chronic hepatitis C predicts a poor response to interferon treatment. J Med Virol 2001;65:681– 687. 16. Fabris P, Brown D, Tositti G, et al. Occult hepatitis B virus infection does not affect liver histology or response to therapy with interferon alpha and ribavirin in intravenous drug users with chronic hepatitis C. J Clin Virol 2004;29:160 –166. 17. Khattab E, Chemin I, Vuillermoz I, et al. Analysis of HCV coinfection with occult hepatitis B virus in patients undergoing IFN therapy. J Clin Virol 2005;33:150 –157. 18. Wherry EJ, Ahmed R. Memory CD8 T-cell differentiation during viral infection. J Virol 2004;78:5535–5545. 19. Galibert F, Mandart E, Fitoussi F, et al. Nucleotide sequence of the hepatitis B virus genome (subtype ayw) cloned in E. coli. Nature 1979;281:646 – 650. 20. Soderberg-Naucler C, Nelson JY. Human cytomegalovirus latency and reactivation—a delicate balance between the virus and its host’s immune system. Intervirology 1999;42:314 –321. 21. Fauci AS, Desrosiers RC. Pathogenesis of HIV and SIV. In: Coffin JM, Hughes SH, Varmus HE, eds. Retroviruses. Plainview, NY: Cold Spring Harbor Laboratory Press, 1997. 22. Michalak TI, Mulrooney PM, Coffin CS. Low doses of hepadnavirus induce infection of the lymphatic system that does not engage the liver. J Virol 2004;78:1730 –1738. 23. Thiers V, Nakajima E, Kremsdorf D, et al. Transmission of hepatitis B from hepatitis-B-seronegative subjects. Lancet 1988;2: 1273–1276. 24. Schuttler CG, Fiedler N, Schmidt K, et al. Suppression of hepatitis B virus enhancer 1 and 2 by hepatitis C virus core protein. J Hepatol 2002;37:855– 862. 25. Chen SY, Kao CF, Chen CM, et al. Mechanisms for inhibition of hepatitis B virus gene expression and replication by hepatitis C virus core protein. J Biol Chem 2003;278:591– 607. T–CELL RESPONSE IN OCCULT HBV INFECTION 1481 26. Shih CM, Lo SJ, Miyamura T, et al. Suppression of hepatitis B virus expression and replication by hepatitis C virus core protein in HuH-7 cells. J Virol 1993;67:5823–5832. 27. Valenzuela P, Quiroga M, Zalvidar J, et al. The nucleotide sequence of the hepatitis B viral genome and the identification of the major viral genes. In: Fields BN, Jaenisch R, Fox CF, eds. Animal virus genetics. New York: Academic Press, 1980:57–70. Received August 6, 2007. Accepted January 31, 2008. Address requests for reprints to: Gabriele Missale, MD, Divisione Malattie Infettive ed Epatologia, Azienda Ospedaliera e Universitaria di Parma, Via Gramsci 14, 43100 Parma, Italy. e-mail: [email protected]; fax: (39) 0521-703857. This study was supported by Schering-Plough S.p.A. (Milan, Italy), grant RBNE013PMJ_006 from the Fondo per gli Investimenti della Ricerca di Base, Ministry of Education, University and Research, by the VIRGIL EC grant QLK2-CT-2002-00700, and by the Fondazione Cassa Risparmio di Parma (Parma, Italy). BASIC–LIVER, PANCREAS, AND BILIARY TRACT May 2008