Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
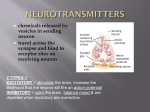
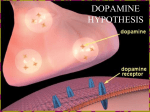
Network interactions in schizophrenia — therapeutic implications Arvid Carlsson (2000) reviews current understanding of the interactions between different neurotransmitters “dramatic synergism between a variety of monoaminergic agonists and MK-801 or other NMDA receptor antagonists” may provide a more advanced neurochemical explanation of schizophrenia” PET Scanning evidence until recently the dopamine hypothesis was only ever supported by “indirect” evidence, e.g. metabolite levels in CSF PET imaging has now revealed abnormal dopaminergic activity in certain brain regions in people with schizophrenia dopamine antagonists) bring the person down to atypically low levels in between psychotic episodes we urgently need to develop drugs that prevent relapse without these side effects Treating schizophrenia Research into dopamine… PET and SPECT scans using radio-labelled dopa to measure how the brain uses dopamine in areas such as the basal ganglia drug-naïve people with SZ are compared with age matched controls when the Pps were given amphetamines, this enhanced release of dopamine significantly more in the SZ group and was more likely to induce SZ symptoms Problems with the dopamine research some people with schizophrenia show dopamine levels that are within the normal range some research suggests that people with ‘catatonic’ symptoms have hypodopaminergic activity the stress of the brain imaging procedures may interfere with dopamine levels Problems cont’d Pps are usually in acute episodes, may not the same for chronic symptoms amphetamine-induced release of dopamine in schizophrenic patients in remission is within the normal range just because radiolabelled dopamine is synthesised more rapidly in Pps with SZ this does mean that endogenous dopamine synthesis is equally abnormal. Carlsson hypothesises that… excess dopamine may be a by-product of dysfunction of some other neurotransmitter an excess in one area may be compensating for a deficiency in some other area to understand schizophrenia we must… examine other neurotransmitters to see whether there are abnormalities in people with schizophrenia Studying neurotransmitters the trouble is not all neurotransmitters are so easy to study in a living brain as dopamine. the easiest is SEROTONIN use a radiolabelled precursor (5hydroxytryptophan) in order to see how quickly serotonin is synthesised similar research has been done with people with depression and the expected abnormalities revealed. The glutamate hypothesis… PCP or ‘angel dust’ is a street drug and like amphetamines it also induces schizophrenic-like symptoms PCP is a powerful antagonist on the NMDA, glutamate receptor PCP has the effect of reducing glutamate levels could hypoglutamatergic activity be a causal factor in schizophrenia? If so is this because glutamate regulates levels of dopamine and/or serotonin? Evidence SPECT imaging studies have found that the NMDA antagonist ketamine (effect: reduces glutamate levels) enhances amphetamine-induced dopamine release in human experiments with rats have also looked at the role of NMDA antagonists slight impact on dopamine release, replicated in other labs. some NMDA antagonists, however, seem to inhibit dopamine release; suggesting that decreased glutamate may bring about schizophrenic symptoms via some route other than increased dopamine release NMDA receptor antagonists appear to stimulate 5-HT (serotonin) turnover and release more consistently than dopaminergic activity high levels of serotonin may also be linked to reduced levels of glutamate. post mortem studies suggest hyperserotonergic function in people with paranoid schizophrenia PCP research seems contradictory, sometimes PCP seems to enhance rather than reduce the release of glutamate Carlsson and Carlsson (1989) mice given drugs to reduce motor activity motor activity was induced again by blocking glutamate receptors in the nucleus accumbens, using a drug called MK-801; this may be seen as a good thing BUT… systemic treatment with MK-801 caused a highly abnormal motor activity low glutamate levels could also lead to negative symptoms, e.g. hypofrontality glutamatergic failure in the … cerebral cortex may lead to negative symptoms basal ganglia could be responsible for the positive symptoms. Glutamate and dopamine SZ can be explained by an interplay between dopamine and glutamate pathways Pathways leading to the striatum from the lower brainstem (mesolimbic) and cortex (mesocortical) Glutamate can control dopamine in two ways, ‘brake’ and ‘accelerator’ The Accelerator; the cortex When everything is working well… glutamate pathways can acts as an accelerator (speed up) the meso-cortical dopamine pathway controlling higher brain centres in the cortex When things go wrong… e.g. NMDA receptors in the midbrain are dysfunctional, dopamine misfiring may contribute to cognitive impairments and symptoms of schizophrenia The brake; limbic system When everything is working well… glutamate neurons that connect to dopamine neurons in the limbic system have a GABA interneuron in-between GABA inhibits the release of dopamine, acting as a brake on dopamine pathways When things go wrong… less glutamatergic activity, means GABA doesn’t put the brakes on! Too much dopamine is released and leads to positive symptoms of psychosis Treatment options Experiments have compared Haloperidol (blocks D2 dopamine receptors ) and M100907 (blocks 5HT serotonin receptors) to see which is best able to overcome amphetamine-induced hyperactivity Haloperidol was more effective They then brought about hyperactivity by lowering glutamate levels with MK-801 (NMDA blocker) This time the serotonin blocker was more effective than the dopamine blocker in reversing the problems! So can M100907 (serotonin antagonist) be used as an antipsychotic may be that it works for some patients more than others possibly due to different causes of their symptoms Advances in drug treatment using both types of drug together may be more effective than either on its own For example clozapine and other ‘atypical’ antipsychotics are both anti-dopaminergic and antiserotonergic clozapine is often effective for treatment resistant schizophrenics for whom decreasing dopamine levels has not worked More on drug treatments this may be because their symptoms are being caused by low glutamate levels which are in turn affecting serotonin levels. drugs that affect glutamate levels could provide relief for people with schizophrenia who have not experienced relief from other medications, e.g. glutamate agonists AJW says, for more information see: Seeman and Guan, (2009) In conclusion, Carlsson suggests … subpopulations with different pathogenesis may exist among patients with schizophrenia a mechanism involving a glutamatergic deficiency appears to deserve special attention. this deficiency may well be secondary to, for example, a failure of connectivity arising at an early developmental stage A glutamatergic deficiency linked to.. the meso-cortical pathways could be responsible for a variety of cognitive and negative symptoms in subcortical, meso-limbic pathways could lead to elevated dopamine levels, potentially triggering a compensatory reduction of presynaptic dopaminergic activity Final thoughts elevated serotonergic activity, pre- and post-synaptically probably contributes to positive and negative symptomatology we need further research into the development of the disease over time, e.g. why psychotic episodes appear to lead to further deterioration other neurotransmitters, such as acetylcholine, gaba and neuropeptides, should also be explored