Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cytokinesis wikipedia , lookup
Cell growth wikipedia , lookup
Extracellular matrix wikipedia , lookup
Tissue engineering wikipedia , lookup
Cell culture wikipedia , lookup
Cell encapsulation wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
Cellular differentiation wikipedia , lookup
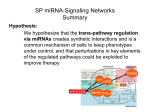
ATVB in Focus MicroRNAs: From Basic Mechanisms to Clinical Application in Cardiovascular Medicine Series Editor: Christian Weber MicroRNAs in Stem Cell Function and Regenerative Therapy of the Heart Florian H. Seeger, Andreas M. Zeiher, Stefanie Dimmeler Abstract—MicroRNAs are small noncoding RNAs that posttranscriptionally control gene expression by targeting mRNAs. Distinct microRNAs regulate stem and progenitor cell functions, thereby modulating cell survival and homing or controlling differentiation and maturation. Experimental studies additionally show that microRNAs regulate endogenous repair and might potentially be useful to enhance the regeneration of the heart. This review summarizes the current studies that address the use of microRNAs to either improve cellular therapies or that might be targeted for enhancing endogenous tissue repair and regeneration after myocardial infarction. (Arterioscler Thromb Vasc Biol. 2013;33:1739-1746.) Key Words: cardiac repair ◼ miR ◼ microRNA ◼ regenerative therapy ◼ stem cell function Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 C oronary artery disease is a progressive disease with a high morbidity and mortality worldwide. Despite improved primary prevention, as well as interventional and pharmacological therapies, the incidence of heart disease is further increasing particularly because of metabolic disorders and an extended life span. After an acute myocardial infarction, the death of cardiomyocytes, which cannot sufficiently be replaced by endogenous regeneration, renders the heart susceptible for unfavorable remodeling and heart failure. Stem/ progenitor cell therapies have been considered as promising options to compensate for the loss of cardiomyocytes. Various adult stem/progenitor cells were used in experimental and clinical trials,1,2 and bone marrow–derived proangiogenic cells and mesenchymal stromal cells were shown to augment the recovery after ischemia in experimental models. The clinical trials overall showed a modest improvement in heart function3,4; however, the results had been heterogeneous and larger scale trials are ongoing to test whether cell therapy with bone marrow–derived cells indeed can improve patient survival. In addition, cardiac stem cells recently showed promising results in phase I/II clinical trials.5,6 Embryonic or induced pluripotent stem cells so far have shown the highest capacity to replace dead myocardium; however, their clinical use is hampered by potential safety hurdles that first need to be addressed.7 and Dicer, and the mature miRNAs are incorporated into the RNA-inducing silencing complex to target mRNAs. About 2000 miRNAs have been identified in humans, and miRNAs are known to influence the expression of ≈30% of the genes. miRNAs contribute to embryonic development and tissue homeostasis but even more profoundly regulate pathophysiological processes.9–11 Tissue injury, as for example myocardial infarction, profoundly disturbs the expression of miRNAs.12 MiRNAs also have an important influence on stem cells; several miRNA families were shown to be required to maintain pluripotency of embryonic stem cells,13,14 and recent studies demonstrated that the combined overexpression of miRNAs is sufficient to induce pluripotent stem cells.13,14 Although the downregulation of pluripotency-related miRNAs is required for differentiation, the differentiation and maturation of stem cells are associated with the increased expression of lineageenriched miRNAs.13,14 Finally, stem/progenitor cell functions are controlled by miRNAs.13 Here, we review the current studies that address the use of miRNAs to either improve cellular therapies or that might be targeted for enhancing endogenous tissue repair and regeneration after myocardial infarction. MiRNAs for Cell Enhancement Various adult progenitor cells, embryonic stem cells, or reprogrammed cells were successfully used to augment heart function after ischemia.1 However, the experience in clinical trials and longer term follow-up studies in experimental models revealed several major challenges: (1) particularly, bone marrow–derived cells showed an impairment in function and survival when isolated from aged patients with chronic disease; (2) the homing and long-term integration of cells applied was poor in most studies15; and (3) a direct cardiac regeneration by replacement of cardiomyocytes was modest or absent in the majority of studies testing adult progenitor cell This article accompanies the ATVB in Focus: MicroRNAs: From Basic Mechanisms to Clinical Application in Cardiovascular Medicine series that was published in the February 2013 issue. MicroRNAs (miRNAs/miRs) are small noncoding RNAs that control gene expression by binding to target mRNAs and thereby inducing translational repression or mRNA degradation.8 MiRNAs are processed by several maturation steps mediated by protein complexes, including the RNases Drosha Received on: February 15, 2013; final version accepted on: April 25, 2013. From the Department of Cardiology, Internal Medicine III (F.H.S., A.M.Z.) and Institute for Cardiovascular Regeneration, Centre of Molecular Medicine (S.D.), Goethe University Frankfurt, Frankfurt, Germany. Correspondence to Stefanie Dimmeler, PhD, Institute for Cardiovascular Regeneration, Centre of Molecular Medicine, Goethe University, TheodorStern-Kai 7, 60590 Frankfurt, Germany. E-mail [email protected] © 2013 American Heart Association, Inc. Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org 1739 DOI: 10.1161/ATVBAHA.113.300138 1740 Arterioscler Thromb Vasc Biol August 2013 populations so far.16 Therefore, several attempts were made to improve cell therapy by interfering with cell function, homing, survival, or differentiation.15 Because miRNAs change gene expression networks and can be easily inhibited by small molecules, they might be interesting candidates to ex vivo treat cells before transplantation. Various miRNAs are modulated by cardiovascular risk factors and disease, and reversal of the deregulated miRNAs might improve the functional capacity of cells in patients with coronary artery disease17–20 (Figure 1). Improvement of Cell Survival and Function by MiRNAs Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Cell survival was affected by several miRNA families in adult progenitor cells or proangiogenic cells. For example, miR-126 was used to augment the efficiency of transplanted cells. miR126 was initially shown to be essential for angiogenic signaling in endothelial cells, but also improved cell survival and migration of mesenchymal stromal cells (MSCs) and proangiogenic bone marrow–derived cells.17,21–23 This may be particularly relevant for autologous cells because both, diabetes mellitus and heart failure, were shown to downregulate miR-126 levels in patient-derived cells.17,19,24 Ex vivo overexpression of miR-126 in MSC or proangiogenic cells improved angiogenesis and augmented the recovery in experimental myocardial infarction models.22,23 MiR-126 is known to repress inhibitors of the phosphatidylinositol 3'-kinase (PI3K)/Akt pathway, which results in the activation of the prosurvival Akt signaling pathway, which promotes cell survival and might also enhance the release of paracrine factors as previously reported for Aktoverexpressing MSC.25 Indeed, Huang et al23 showed that overexpression of miR-126 augments the release of paracrine factors from MSC, which contributes to the improvement of repair after cell transplantation. Besides Akt, miR-126 controls the expression of the Notch ligand Delta-like 4 in MSC. By controlling this pathway, miR-126 does not only improve cell survival but also promotes tubulogenesis.23 Interestingly, miR-126 seems not only to act as cell intrinsic regulator of cell functionality but is also released and acts in a paracrine manner to augment neovascularization. The cellular release of exosomes, which among other factors contain miRNAs, is known to mediate cell-to-cell communication between several cell types.26–28 For example, exosomes derived from CD34+ cells improve neovascularization after ischemia.29 A recent study now demonstrates that miR-126 is preferentially enriched in microvesicles derived from CD34+ cells compared with other cell types and contributes to the proangiogenic activity of the cell supernatants.19 In addition, Cantaluppi et al30 demonstrated that proangiogenic cells release miRNAs 126– and miR-296–containing microvesicles that induce angiogenesis in endothelial cells. An impaired expression of miR-126 was demonstrated in microvesicles isolated from supernatants of peripheral blood CD34+ cells from patients with diabetes mellitus, and overexpression of miR-126 restored the proangiogenic activity of diabetic CD34+ cells.19 These findings are consistent with the lower circulating levels of miR-126 detected in patients with diabetes mellitus or coronary artery disease31,32 and overall may contribute to the known impaired neovascularization capacity observed in patients with diabetes mellitus. MiR-34a represents a second example that is regulated during disease and affects the functional capacity and survival of cells used for cell therapy. miR-34a is profoundly induced by aging and in bone marrow–derived cells from patients with heart failure and its inhibition improved the survival of the cells in vitro.20 Ex vivo treatment of bone marrow–derived mononuclear cells with miR-34a inhibitors augments the cell transplantation–induced improved functional recovery after acute myocardial infarction.20 Vice versa, overexpression of miR-34a induced cells death20 and worsened the proangiogenic activity of proanigogenic cells by increasing senescence.33 In addition, miR-34a influenced apoptosis signaling by, for example, targeting the antiapoptotic protein B-cell lymphoma 2 (Bcl-2) and it blocked cellular proliferation by repression of cell cycle regulators, such as cyclin D2 and cyclin-dependent kinases.20,34 In proangiogenic cells the histone deacetylase silent mating type information regulation 2 homolog 1 (SIRT1) was reported to be inhibited by miR-34a, which may additionally contribute to the detrimental function of miR-34a in vascular repair.35,36 MiRNAs also augmented cell survival and in vivo functional capacity of cardiac stem/progenitor cells. An interesting study tests the effect of individual miRNAs versus combinations and showed that the combination of 3 miRNAs, namely miR-21, miR-24, and miR-221, is more efficient to improve engraftment and survival of transplanted cardiac progenitor cells.37 The above-mentioned miRNAs target the apoptotic protein Bim and thereby directly improve cell survival.37 In addition, miR-155 overexpression repressed necrosis of cardiac stem cells.38 Cellular senescence, which compromises cellular functions, can be regulated by miRNAs. Thus, miR-10a*, miR21, and miR-34a increase senescence of proangiogenic cells, whereas the inhibition of these miRs improved angiogenesis.33,36,39 Particularly, antagonizing miR-21 reduced reactive oxygen species production,18 which can contribute to cellular dysfunction and senescence. Several miRNAs modulated the migration of cells; miR-150 and miR-146 target the stromal cell-derived factor 1 (SDF-1) receptor chemokine receptor type 4 (CXCR4), which is essential for progenitor and proangiogenic cell homing to ischemic tissues,40,41 and miR-15a and miR-16 were recently shown to profoundly inhibit the migratory potential of proangiogenic cells isolated from patients with critical limb ischemia.42 The targets of miR-15a/16 include the proangiogenic cytokine vascular endothelial growth factor (VEGF) and the Akt isoform-3 that contribute to the defective function of proangiogenic cells from patients with limb ischemia.42 However, both miRNAs target a variety of antiapoptotic proteins that may have contributed to their detrimental effects as well. Enhancement of Differentiation of Transplanted Stem/Progenitor Cells Although embryonic stem cells can acquire a cardiac muscle cell phenotype and, therefore, might be useful to regeneration therapies, their integration, survival, and homing have been shown to be limited in some studies.43 Moreover, the generation of fully mature differentiated cells is a major challenge. Recent studies Seeger et al MicroRNAs and Cardiac Repair 1741 now suggest that overexpression of miR-1 in embryonic stem cells enhanced cardiac differentiation after transplantation,44,45 a finding which is consistent with previous in vitro reports showing an increase in cardiac lineage commitment by the overexpression of cardiac miRs, such as miR-1 or miR-499.46–48 Whether such an approach might be also useful to improve the cardiac differentiation capacities of adult progenitor cells deserves further studies. Interestingly, the miR-1–overexpressing embryonic stem cells also reduced apoptosis of the host cardiomyocytes suggesting that miRNAs can exhibit pleiotropic effects, which together may lead to a better tissue repair. In summary, ex vivo regulation of several miRNAs by antimiRs or miR mimics can improve cell survival and affects the functions of several stem/progenitor cells and proangiogenic cells that are used for therapeutic augmenting cardiac repair and regeneration. The engineering of cells by ex vivo treatment with anti-miR mimics might be a promising tool to improve the success of cell therapy. Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 MiRNAs and Postischemic Protection The recovery of heart function after ischemia is influenced by various processes and can be enhanced by blocking cardiomyocyte cell death or by improving tissue perfusion. In addition, the invasion of inflammatory cells enhances tissue damage; however, inflammation is also required for wound healing and tissue remodeling. During later stages, the replacement of dead cardiomyocytes by fibrotic tissue contributes to the impairment of heart function. Given the multiple functions of miRNAs, it does not come as a surprise that all of these processes are regulated by diverse miRNAs. Prevention of Cardiomyocyte Death The miR-15 family, which comprises 6 closely related miRs, is increased in murine and pig hearts within 24 hours after ischemia/reperfusion injury.49 Inhibition of miR-15 family members reduced hypoxia and hypoxia/reoxygenation-induced cardiomyocyte cell death49 and improved mitochondrial function and ATP levels.50 In vivo, miR-15 inhibition by short locked nucleic acid-based anti-miRs (so called tiny miRs) reduces infarct size in mice after ischemia/reperfusion injury.49 MiR-15 targets the antiapoptotic protein Bcl-2 and the mitochondrial protective protein ADP-ribosylation factor-like 2 in cardiomyocytes.49,50 A similar effect was reported for the miR-34 family, which is induced by myocardial infarction and promotes cardiomyocyte cell death.51–53 Inhibition of miR-34 family members improved cardiac function after acute myocardial infarction.53,54 Moreover, a cardioprotective effect was observed during cardiac aging.54 MiR-34a targets SIRT1, which is a vasculo- and cardioprotective deacetylase, and its derepression contributes to the antiapoptotic effects of miR-34 inhibition. In addition, the protein phosphatase 1 regulator PNUTS (or serine/threonineprotein phosphatase 1 regulatory subunit 10 [PPP1R10]), a protein involved in DNA damage response and telomere shortening, is repressed by miR-34 (Figures 1 and 2).52,54 Among the miRNAs that are upregulated after cardiac stress, miR-214 exhibits a protective function. miR-214 is downregulated during embryonic development and further decreased in adult mice, but it is reexpressed within 7 days after ischemia/ reperfusion injury.55 Genetic deletion of miR-214 aggravated ischemic/reperfusion-induced cell death and induced a further deterioration of heart function.55 This effect was at least in part mediated by a repression of the sodium/calcium exchanger Ncx1, which under stress conditions contributes to calcium overload.55 Three miR-214 targets, namely cyclophilin D—a regulator of the mitochondrial permeability transition pore— the proapoptotic protein Bim, and the hypertrophy-regulating Ca2+/calmodulin-dependent protein kinases I (CaMKIId), were identified in the hearts and all may contribute to the observed protective effect of this miRNA.55 The proapoptotic protein Bim is additionally targeted by miR-24, which is downregulated after acute myocardial infarction.56 Overexpression of miR-24 reduced cardiomyocyte apoptosis in vitro and in vivo and attenuated infarct size and improved heart function after myocardial infarction.56 Moreover, miR-20a, which is part of the miR17-92 cluster, inhibits apoptosis of cardiomyocytes.57 Improvement of Perfusion/Angiogenesis MiR-92a was the first miRNA shown to control neovascularization after acute myocardial infarction.58 Inhibition of miR-92a enhanced endothelial cell migration and sprouting in cell culture studies.58,59 In vivo, miR-92a is increased within the first days after infarction and its inhibition increased capillary density and improved heart function after myocardial infarction.58 In endothelial cells, miR-92a targets integrin a5,58 which prevents endothelial cell apoptosis and is important for vessel maturation.60 In addition, several vasculoprotective genes were repressed by miR-92a, such as SIRT1, which prevent endothelial NO synthase acetylation and inactivation.61 In addition, various miRNAs are meanwhile identified as regulators of angiogenesis.62 Most studies, however, did not test the function in myocardial infarction. Among the miRNAs that are tested for their potential role in regulating cardiac neovascularization, miR-24 was shown to inhibit angiogenesis in various models, and antagomirs directed against miR24 improved the recovery after acute myocardial infarction by targeting the endothelium-enriched transcription factor GATA2 and the p21-activated kinase 4.63 The improvement of cardiac function by antagomirs directed against miR-24 is counterintuitive to the above-discussed findings that miR24 overexpression attenuates infarct size and improved heart function.56 However, recent studies showed that antagomirs directed against miR-24 protected against the transition from hypertrophy to decompensated heart failure by interfering with excitation–contraction coupling after aortic constriction.64 Further studies need to clarify the role of miR-24 in neovascularization versus direct cardioprotection. One may speculate that the inhibitors target different cells and affect different pathways compared with the unphysiological overexpression of the miRNA. The miR-15 family inhibits angiogenesis after hind-limb or myocardial ischemia,49,65,66 which in combination with the induction of cardiac cell death may contribute to the profound functional effects of miR-15 inhibitors in experimental myocardial infarction discussed above. 1742 Arterioscler Thromb Vasc Biol August 2013 Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Figure 1. Effects of microRNAs (miRNAs/miRs) on cell therapy. The figure summarizes the possible use of miRNAs to improve for cell therapy (A) and shows some of the mechanisms by which miRNAs regulate the function of proangiogenic cells for cardiovascular repair (B). BIM indicates B-cell lymphoma 2 interacting mediator of cell death; CDK, cyclin dependent kinase; and Dll, delta-like protein. Prevention of Fibrosis MiR-29 is repressed by cardiac stressors, such as aortic banding, and is reduced after acute myocardial infarction.12,67 Interestingly, the miR-29 family targets multiple proteins involved in fibrosis, including multiple collagens, fibrillins, and elastin.12,68 Thus, overexpression of miR-29 might be an interesting therapeutic option to block the fibrotic response. MiR-21 was among the first miRNAs that was shown to be upregulated after acute myocardial infarction.12 Subsequent studies blocked miR-21 by antagomirs and reported that this enhanced cardiac function and prevents cardiac fibrosis.69 However, genetic deletion of miR-21 or blocking of miR-21 with shorter locked nucleic acid-based anti-miRs had no effect in other studies.70 Although ample evidence supports a direct profibrotic function of miR-21,71 it might have additional functions in other cells. For examples, miR-21 was shown to prevent H2O2-induced cardiomyocyte cell death.72 Likewise, overexpression of miR-21 via adenovirus-expressing miR21 inhibited cardiomyocyte apoptosis and decreased myocardial infarct size after acute myocardial infarction.73 These studies showed that miR-21 targets the proapoptotic gene– programmed cell death 4 and the activator protein 1 pathway, which play a crucial role in cardiomyocyte cell death.74 MiR-101 has also been implicated in cardiac fibrosis. It is downregulated after 4 weeks of acute myocardial infarction and forced overexpression of miR-101a/b, to compensate for the long-term repression of this miR, inhibited proliferation of cardiac fibroblasts, and reduced collagen production.75 Mechanistically, miR-101 was targeting the c-fos and transforming growth factor-β1 signaling pathways.75 MiRNAs and Endogenous Cardiac Regeneration Attempts to truly regenerate the heart have been challenging particularly because the strategy of exogenous cell therapy faced multiple problems, including the limited survival, integration, and differentiation capacity of various tested cell types.15,76 Although the adult mammalian heart is one of the least regenerative organs, recent studies suggest that activation of endogenous cardiac regeneration might be possible by Seeger et al MicroRNAs and Cardiac Repair 1743 Cardiomyocyte proliferation Cell death miR-15 miR-195 miR-199 miR-590 miR-15 miR-24 miR-34 miR-214 (calcium overload) Cardiac reprogramming Fibrosis miR-21 miR-29 miR-101 Angiogenesis miR-15 miR-24 miR-92a Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 augmenting cardiomyocyte proliferation or by reprogramming fibroblasts into functional cardiomyocytes. MiRNAs might be suitable to trigger or enhance both processes.9,77 Moreover, a combination of miRNAs can be used to turn fibroblasts to induced pluripotent stem cells.13 MiRNAs and Cardiomyocyte Proliferation MiRNA expression profiles in neonatal mouse hearts, which possess the capacity to regenerate at least until day 7, showed that several miRNAs are regulated during postnatal cardiac development. Among the highly regulated miRNAs are members of the miR-15 family, particularly miR-195, which is upregulated within the first days after birth.78,79 The miR-195 upregulation coincides with the postnatal transition of the heart toward cell cycle arrest, suggesting that it might contribute to the mitotic arrest of cardiomyocytes after birth. Indeed, inhibition of miR-15 family members increased the rate of proliferating cardiomyocytes up to day 12 after birth,78 whereas overexpression of miR-195 impaired cardiomyocyte proliferation and induced ventricular hypoplasia and septal defects.78 The miR-15 family members profoundly modulated the expression of proliferation-associated genes in cardiomyocytes, a finding that is consistent with the antiproliferative activity of miR-15 in other cell types.80 Specifically, checkpoint kinase 1 was identified as a direct target of miR-15 in cardiomyocytes.78 A functional miRNA screen recently confirmed that miR-15 inhibits cardiomyocyte proliferation.81 Furthermore, various additional miRNAs were identified that control cardiomyocyte proliferation. Two of these miRNAs, namely miR-590 and miR-199a, were further validated and the study shows that overexpression of each of these miRNAs promotes cardiomyocyte proliferation in neonatal and adult mice.81 Interestingly, viral overexpression of the miRNAs enhanced cardiomyocyte proliferation and preserved long-term cardiac function after permanent ligation of the coronary artery.81 Together, at least in mouse models, miRNAs may be useful to reverse the cell cycle blockade of adult cardiomyocytes. Further studies have to evaluate the function in adult human cardiomyocytes. Fibroblast miRNAs? Figure 2. MicroRNAs (MiRNAs) in postinfarction repair. miR-1 miR-208 miR-499 Induced Cardiomyocyte MiRNAs and Direct Reprogramming Besides inducing cardiomyocyte proliferation, miRNAs may be also useful to augment direct cardiac reprogramming. Direct cardiac reprogramming of fibroblasts has first been achieved by combined overexpression of cardiac transcription factors, such as GATA4, myocyte-specific enhancer factor 2C (MEF2C), and T-box transcription factor (TBX5),82,83 or the 3 factors with the addition of Hand2.84 As discussed above, cardiac-enriched miRNAs were shown to facilitate cardiac differentiation of stem cells.44,46,47,85 Therefore, Jayawardena et al86 tested whether miRNAs might be helpful to convert fibroblasts into cardiomyocyte-like cells. Indeed, the combination of several miRNAs, namely miR-1, miR-133, miR-208, and miR499, augmented cardiac marker gene expression in fibroblasts in vitro. Overexpression of the miR cocktail also increased the reprogramming of cardiac fibroblasts into cardiomyocytes in vivo as shown by using lineage tracing.86 Although the extent of converting fibroblasts into cardiomyocytes in principle is rather low and even more challenging in human cells, further studies may overcome these hurdles by combining transcription factors with miRNAs and small molecules to optimize this promising therapeutic strategy. Outlook Various experimental studies provide convincing evidence that miRNAs might be targeted to improving cell therapy or enhancing endogenous repair processes. Despite these encouraging data, the development of miRNA therapeutics faces several challenges and questions; although miRNA inhibition is very efficient,87 overexpression of miRNAs is not yet established with small molecules and requires the use of vectors. Gene therapy recently gained back attention with the first gene therapy being approved in Europe88 and promising results being reported for cardiac gene therapy with the adenoassociated virus-vectors89; however, it is still not at a stage that would allow easy clinical translation. Second, the biology of miRNAs is far from being understood and the moderate repression of multiple targets by miRNAs requires a system 1744 Arterioscler Thromb Vasc Biol August 2013 biology approach to identify the full impact on the gene expression networks. Some miRNAs target patterns of genes with a common biological function (eg, miR-29 targeting various matrix proteins); however, other miRNAs target genes with antagonistic functions (eg, pro- and antiapoptotic genes) making it even more complicated to understand the biological activities. Finally, targeting ubiquitously expressed miRNAs may face challenges with respect to unwanted side effects in other cells or tissue. Therefore, cell type–specific delivery strategies may be required in some cases. However, the promising results from recent phase II clinical trials documenting not only the safety and feasibility but also the biological function of anti-miRs for the treatment of hepatitis encourage the development of miRNA therapeutics for the treatment of cardiovascular diseases. Acknowledgments We thank Susanne Heydt for the artwork. Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Disclosures S. Dimmeler is supported by the European Research Council advance grant Angiomir. S. Dimmeler and A.M. Zeiher are founders of t2cure GmbH. The other author reports no conflicts. References 1. Dimmeler S, Burchfield J, Zeiher AM. Cell-based therapy of myocardial infarction. Arterioscler Thromb Vasc Biol. 2008;28:208–216. 2. van der Bogt KE, Sheikh AY, Schrepfer S, Hoyt G, Cao F, Ransohoff KJ, Swijnenburg RJ, Pearl J, Lee A, Fischbein M, Contag CH, Robbins RC, Wu JC. Comparison of different adult stem cell types for treatment of myocardial ischemia. Circulation. 2008;118:S121–S129. 3.Jeevanantham V, Butler M, Saad A, Abdel-Latif A, Zuba-Surma EK, Dawn B. Adult bone marrow cell therapy improves survival and induces long-term improvement in cardiac parameters: a systematic review and meta-analysis. Circulation. 2012;126:551–568. 4. Martin-Rendon E, Brunskill SJ, Hyde CJ, Stanworth SJ, Mathur A, Watt SM. Autologous bone marrow stem cells to treat acute myocardial infarction: a systematic review. Eur Heart J. 2008;29:1807–1818. 5. Chugh AR, Beache GM, Loughran JH, Mewton N, Elmore JB, Kajstura J, Pappas P, Tatooles A, Stoddard MF, Lima JA, Slaughter MS, Anversa P, Bolli R. Administration of cardiac stem cells in patients with ischemic cardiomyopathy: the SCIPIO trial: surgical aspects and interim analysis of myocardial function and viability by magnetic resonance. Circulation. 2012;126:S54–S64. 6. Bolli R, Chugh AR, D’Amario D, et al. Cardiac stem cells in patients with ischaemic cardiomyopathy (SCIPIO): initial results of a randomised phase 1 trial. Lancet. 2011;378:1847–1857. 7. Sun N, Longaker MT, Wu JC. Human iPS cell-based therapy: considerations before clinical applications. Cell Cycle. 2010;9:880–885. 8. Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116:281–297. 9. Small EM, Olson EN. Pervasive roles of microRNAs in cardiovascular biology. Nature. 2011;469:336–342. 10.Iorio MV, Croce CM. MicroRNA dysregulation in cancer: diagnostics, monitoring and therapeutics. A comprehensive review. EMBO Mol Med. 2012;4:143–159. 11.Di Leva G, Calin GA, Croce CM. MicroRNAs: fundamental facts and involvement in human diseases. Birth Defects Res C Embryo Today. 2006;78:180–189. 12.van Rooij E, Sutherland LB, Thatcher JE, DiMaio JM, Naseem RH, Marshall WS, Hill JA, Olson EN. Dysregulation of microRNAs after myocardial infarction reveals a role of miR-29 in cardiac fibrosis. Proc Natl Acad Sci USA. 2008;105:13027–13032. 13.Heinrich EM, Dimmeler S. MicroRNAs and stem cells: control of pluripotency, reprogramming, and lineage commitment. Circ Res. 2012;110:1014–1022. 14.Leonardo TR, Schultheisz HL, Loring JF, Laurent LC. The functions of microRNAs in pluripotency and reprogramming. Nat Cell Biol. 2012;14:1114–1121. 15. Chavakis E, Dimmeler S. Homing of progenitor cells to ischemic tissues. Antioxid Redox Signal. 2011;15:967–980. 16. Mummery CL, Davis RP, Krieger JE. Challenges in using stem cells for cardiac repair. Sci Transl Med. 2010;2:27ps17. 17. Jakob P, Doerries C, Briand S, et al. Loss of angiomiR-126 and 130a in angiogenic early outgrowth cells from patients with chronic heart failure: role for impaired in vivo neovascularization and cardiac repair capacity. Circulation. 2012;126:2962–2975. 18. Fleissner F, Jazbutyte V, Fiedler J, Gupta SK, Yin X, Xu Q, Galuppo P, Kneitz S, Mayr M, Ertl G, Bauersachs J, Thum T. Short communication: asymmetric dimethylarginine impairs angiogenic progenitor cell function in patients with coronary artery disease through a microRNA-21- dependent mechanism. Circ Res. 2010;107:138–143. 19. Mocharla P, Briand S, Giannotti G, Dörries C, Jakob P, Paneni F, Lüscher T, Landmesser U. AngiomiR-126 expression and secretion from circulating CD34(+) and CD14(+) PBMCs: role for proangiogenic effects and alterations in type 2 diabetics. Blood. 2013;121:226–236. 20. Xu Q, Seeger FH, Castillo J, Iekushi K, Boon RA, Farcas R, Manavski Y, Li YG, Assmus B, Zeiher AM, Dimmeler S. Micro-RNA-34a contributes to the impaired function of bone marrow-derived mononuclear cells from patients with cardiovascular disease. J Am Coll Cardiol. 2012;59:2107–2117. 21. Meng S, Cao JT, Zhang B, Zhou Q, Shen CX, Wang CQ. Downregulation of microRNA-126 in endothelial progenitor cells from diabetes patients, impairs their functional properties, via target gene Spred-1. J Mol Cell Cardiol. 2012;53:64–72. 22.Chen JJ, Zhou SH. Mesenchymal stem cells overexpressing MiR-126 enhance ischemic angiogenesis via the AKT/ERK-related pathway. Cardiol J. 2011;18:675–681. 23. Huang F, Zhu X, Hu XQ, Fang ZF, Tang L, Lu XL, Zhou SH. Mesenchymal stem cells modified with miR-126 release angiogenic factors and activate Notch ligand Delta-like-4, enhancing ischemic angiogenesis and cell survival. Int J Mol Med. 2013;31:484–492. 24.Zhang Q, Kandic I, Kutryk MJ. Dysregulation of angiogenesis-related microRNAs in endothelial progenitor cells from patients with coronary artery disease. Biochem Biophys Res Commun. 2011;405:42–46. 25. Mirotsou M, Zhang Z, Deb A, Zhang L, Gnecchi M, Noiseux N, Mu H, Pachori A, Dzau V. Secreted frizzled related protein 2 (Sfrp2) is the key Akt-mesenchymal stem cell-released paracrine factor mediating myocardial survival and repair. Proc Natl Acad Sci USA. 2007;104:1643–1648. 26. Hergenreider E, Heydt S, Tréguer K, Boettger T, Horrevoets AJ, Zeiher AM, Scheffer MP, Frangakis AS, Yin X, Mayr M, Braun T, Urbich C, Boon RA, Dimmeler S. Atheroprotective communication between endothelial cells and smooth muscle cells through miRNAs. Nat Cell Biol. 2012;14:249–256. 27.Ranghino A, Cantaluppi V, Grange C, Vitillo L, Fop F, Biancone L, Deregibus MC, Tetta C, Segoloni GP, Camussi G. Endothelial progenitor cell-derived microvesicles improve neovascularization in a murine model of hindlimb ischemia. Int J Immunopathol Pharmacol. 2012;25:75–85. 28.Camussi G, Deregibus MC, Bruno S, Grange C, Fonsato V, Tetta C. Exosome/microvesicle-mediated epigenetic reprogramming of cells. Am J Cancer Res. 2011;1:98–110. 29. Sahoo S, Klychko E, Thorne T, Misener S, Schultz KM, Millay M, Ito A, Liu T, Kamide C, Agrawal H, Perlman H, Qin G, Kishore R, Losordo DW. Exosomes from human CD34(+) stem cells mediate their proangiogenic paracrine activity. Circ Res. 2011;109:724–728. 30. Cantaluppi V, Biancone L, Figliolini F, Beltramo S, Medica D, Deregibus MC, Galimi F, Romagnoli R, Salizzoni M, Tetta C, Segoloni GP, Camussi G. Microvesicles derived from endothelial progenitor cells enhance neoangiogenesis of human pancreatic islets. Cell Transplant. 2012;21:1305–1320. 31. Fichtlscherer S, De Rosa S, Fox H, Schwietz T, Fischer A, Liebetrau C, Weber M, Hamm CW, Röxe T, Müller-Ardogan M, Bonauer A, Zeiher AM, Dimmeler S. Circulating microRNAs in patients with coronary artery disease. Circ Res. 2010;107:677–684. 32. Zampetaki A, Kiechl S, Drozdov I, Willeit P, Mayr U, Prokopi M, Mayr A, Weger S, Oberhollenzer F, Bonora E, Shah A, Willeit J, Mayr M. Plasma microRNA profiling reveals loss of endothelial miR-126 and other microRNAs in type 2 diabetes. Circ Res. 2010;107:810–817. 33. Zhao T, Li J, Chen AF. MicroRNA-34a induces endothelial progenitor cell senescence and impedes its angiogenesis via suppressing silent information regulator 1. Am J Physiol Endocrinol Metab. 2010;299:E110–E116. Seeger et al MicroRNAs and Cardiac Repair 1745 Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 34.Hermeking H. The miR-34 family in cancer and apoptosis. Cell Death Differ. 2010;17:193–199. 35.Tabuchi T, Satoh M, Itoh T, Nakamura M. MicroRNA-34a regulates the longevity-associated protein SIRT1 in coronary artery disease: effect of statins on SIRT1 and microRNA-34a expression. Clin Sci (Lond). 2012;123:161–171. 36.Ito T, Yagi S, Yamakuchi M. MicroRNA-34a regulation of endothelial senescence. Biochem Biophys Res Commun. 2010;398:735–740. 37. Hu S, Huang M, Nguyen PK, Gong Y, Li Z, Jia F, Lan F, Liu J, Nag D, Robbins RC, Wu JC. Novel microRNA prosurvival cocktail for improving engraftment and function of cardiac progenitor cell transplantation. Circulation. 2011;124:S27–S34. 38.Liu J, van Mil A, Vrijsen K, Zhao J, Gao L, Metz CH, Goumans MJ, Doevendans PA, Sluijter JP. MicroRNA-155 prevents necrotic cell death in human cardiomyocyte progenitor cells via targeting RIP1. J Cell Mol Med. 2011;15:1474–1482. 39.Zhu S, Deng S, Ma Q, Zhang T, Jia C, Zhuo D, Yang F, Wei J, Wang L, Dykxhoorn DM, Hare JM, Goldschmidt PJ, Dong C. Microrna-10a* and microrna-21 modulate endothelial progenitor cell senescence via suppressing hmga2. Circ Res. 2012;112: 152–64 40. Tano N, Kim HW, Ashraf M. microRNA-150 regulates mobilization and migration of bone marrow-derived mononuclear cells by targeting Cxcr4. PLoS One. 2011;6:e23114. 41. Labbaye C, Spinello I, Quaranta MT, Pelosi E, Pasquini L, Petrucci E, Biffoni M, Nuzzolo ER, Billi M, Foà R, Brunetti E, Grignani F, Testa U, Peschle C. A three-step pathway comprising PLZF/miR-146a/CXCR4 controls megakaryopoiesis. Nat Cell Biol. 2008;10:788–801. 42. Spinetti G, Fortunato O, Caporali A, Shantikumar S, Marchetti M, Meloni M, Descamps B, Floris I, Sangalli E, Vono R, Faglia E, Specchia C, Pintus G, Madeddu P, Emanueli C. MicroRNA-15a and microRNA-16 impair human circulating proangiogenic cell functions and are increased in the proangiogenic cells and serum of patients with critical limb ischemia. Circ Res. 2013;112:335–346. 43.Mummery CL, Zhang J, Ng ES, Elliott DA, Elefanty AG, Kamp TJ. Differentiation of human embryonic stem cells and induced pluripotent stem cells to cardiomyocytes: a methods overview. Circ Res. 2012;111:344–358. 44.Glass C, Singla DK. MicroRNA-1 transfected embryonic stem cells enhance cardiac myocyte differentiation and inhibit apoptosis by modulating the PTEN/Akt pathway in the infarcted heart. Am J Physiol Heart Circ Physiol. 2011;301:H2038–H2049. 45. Glass C, Singla DK. ES cells overexpressing microRNA-1 attenuate apoptosis in the injured myocardium. Mol Cell Biochem. 2011;357:135–141. 46.Sluijter JP, van Mil A, van Vliet P, Metz CH, Liu J, Doevendans PA, Goumans MJ. MicroRNA-1 and -499 regulate differentiation and proliferation in human-derived cardiomyocyte progenitor cells. Arterioscler Thromb Vasc Biol. 2010;30:859–868. 47.Wilson KD, Hu S, Venkatasubrahmanyam S, Fu JD, Sun N, Abilez OJ, Baugh JJ, Jia F, Ghosh Z, Li RA, Butte AJ, Wu JC. Dynamic microRNA expression programs during cardiac differentiation of human embryonic stem cells: role for miR-499. Circ Cardiovasc Genet. 2010;3:426–435. 48.Ivey KN, Muth A, Arnold J, King FW, Yeh RF, Fish JE, Hsiao EC, Schwartz RJ, Conklin BR, Bernstein HS, Srivastava D. MicroRNA regulation of cell lineages in mouse and human embryonic stem cells. Cell Stem Cell. 2008;2:219–229. 49.Hullinger TG, Montgomery RL, Seto AG, Dickinson BA, Semus HM, Lynch JM, Dalby CM, Robinson K, Stack C, Latimer PA, Hare JM, Olson EN, van Rooij E. Inhibition of miR-15 protects against cardiac ischemic injury. Circ Res. 2012;110:71–81. 50. Nishi H, Ono K, Iwanaga Y, Horie T, Nagao K, Takemura G, Kinoshita M, Kuwabara Y, Mori RT, Hasegawa K, Kita T, Kimura T. MicroRNA-15b modulates cellular ATP levels and degenerates mitochondria via Arl2 in neonatal rat cardiac myocytes. J Biol Chem. 2010;285:4920–4930. 51. Iekushi K, Seeger F, Assmus B, Zeiher AM, Dimmeler S. Regulation of cardiac microRNAs by bone marrow mononuclear cell therapy in myocardial infarction. Circulation. 2012;125:1765–73, S1. 52. Yamakuchi M, Ferlito M, Lowenstein CJ. miR-34a repression of SIRT1 regulates apoptosis. Proc Natl Acad Sci U S A. 2008;105:13421–13426. 53.Bernardo BC, Gao XM, Winbanks CE, Boey EJ, Tham YK, Kiriazis H, Gregorevic P, Obad S, Kauppinen S, Du XJ, Lin RC, McMullen JR. Therapeutic inhibition of the miR-34 family attenuates pathological cardiac remodeling and improves heart function. Proc Natl Acad Sci U S A. 2012;109:17615–17620. 54. Boon RA, Iekushi K, Lechner S, et al. MicroRNA-34a regulates cardiac ageing and function. Nature. 2013;495:107–110. 55. Aurora AB, Mahmoud AI, Luo X, Johnson BA, van Rooij E, Matsuzaki S, Humphries KM, Hill JA, Bassel-Duby R, Sadek HA, Olson EN. MicroRNA-214 protects the mouse heart from ischemic injury by controlling Ca²+ overload and cell death. J Clin Invest. 2012;122:1222–1232. 56. Qian L, Van Laake LW, Huang Y, Liu S, Wendland MF, Srivastava D. miR24 inhibits apoptosis and represses Bim in mouse cardiomyocytes. J Exp Med. 2011;208:549–560. 57. Frank D, Gantenberg J, Boomgaarden I, Kuhn C, Will R, Jarr KU, Eden M, Kramer K, Luedde M, Mairbäurl H, Katus HA, Frey N. MicroRNA20a inhibits stress-induced cardiomyocyte apoptosis involving its novel target Egln3/PHD3. J Mol Cell Cardiol. 2012;52:711–717. 58. Bonauer A, Carmona G, Iwasaki M, et al. MicroRNA-92a controls angiogenesis and functional recovery of ischemic tissues in mice. Science. 2009;324:1710–1713. 59. Iaconetti C, Polimeni A, Sorrentino S, Sabatino J, Pironti G, Esposito G, Curcio A, Indolfi C. Inhibition of miR-92a increases endothelial proliferation and migration in vitro as well as reduces neointimal proliferation in vivo after vascular injury. Basic Res Cardiol. 2012;107:296. 60.Urbich C, Walter DH, Zeiher AM, Dimmeler S. Laminar shear stress upregulates integrin expression: role in endothelial cell adhesion and apoptosis. Circ Res. 2000;87:683–689. 61. Wu W, Xiao H, Laguna-Fernandez A, Villarreal G Jr, Wang KC, Geary GG, Zhang Y, Wang WC, Huang HD, Zhou J, Li YS, Chien S, GarciaCardena G, Shyy JY. Flow-Dependent Regulation of Kruppel-Like Factor 2 Is Mediated by MicroRNA-92a. Circulation. 2011;124:633–641. 62.Bonauer A, Boon RA, Dimmeler S. Vascular microRNAs. Curr Drug Targets. 2010;11:943–949. 63. Fiedler J, Jazbutyte V, Kirchmaier BC, et al. MicroRNA-24 regulates vascularity after myocardial infarction. Circulation. 2011;124:720–730. 64. Li RC, Tao J, Guo YB, et al. In vivo suppression of microRNA-24 prevents the transition toward decompensated hypertrophy in aortic-constricted mice. Circ Res. 2013;112:601–605. 65.Yin KJ, Olsen K, Hamblin M, Zhang J, Schwendeman SP, Chen YE. Vascular endothelial cell-specific microRNA-15a inhibits angiogenesis in hindlimb ischemia. J Biol Chem. 2012;287:27055–27064. 66.Liu LF, Liang Z, Lv ZR, Liu XH, Bai J, Chen J, Chen C, Wang Y. MicroRNA-15a/b are up-regulated in response to myocardial ischemia/ reperfusion injury. J Geriatr Cardiol. 2012;9:28–32. 67. van Rooij E, Sutherland LB, Liu N, Williams AH, McAnally J, Gerard RD, Richardson JA, Olson EN. A signature pattern of stress-responsive microRNAs that can evoke cardiac hypertrophy and heart failure. Proc Natl Acad Sci U S A. 2006;103:18255–18260. 68.Boon RA, Seeger T, Heydt S, Fischer A, Hergenreider E, Horrevoets AJ, Vinciguerra M, Rosenthal N, Sciacca S, Pilato M, van Heijningen P, Essers J, Brandes RP, Zeiher AM, Dimmeler S. MicroRNA-29 in aortic dilation: implications for aneurysm formation. Circ Res. 2011;109:1115–1119. 69. Thum T, Gross C, Fiedler J, et al. MicroRNA-21 contributes to myocardial disease by stimulating MAP kinase signalling in fibroblasts. Nature. 2008;456:980–984. 70.Patrick DM, Montgomery RL, Qi X, Obad S, Kauppinen S, Hill JA, van Rooij E, Olson EN. Stress-dependent cardiac remodeling occurs in the absence of microRNA-21 in mice. J Clin Invest. 2010;120:3912–3916. 71. Bauersachs J. miR-21: a central regulator of fibrosis not only in the broken heart. Cardiovasc Res. 2012;96:227–229; discussion 230. 72. Cheng Y, Liu X, Zhang S, Lin Y, Yang J, Zhang C. MicroRNA-21 protects against the H(2)O(2)-induced injury on cardiac myocytes via its target gene PDCD4. J Mol Cell Cardiol. 2009;47:5–14. 73.Dong S, Cheng Y, Yang J, Li J, Liu X, Wang X, Wang D, Krall TJ, Delphin ES, Zhang C. MicroRNA expression signature and the role of microRNA-21 in the early phase of acute myocardial infarction. J Biol Chem. 2009;284:29514–29525. 74.Cheng Y, Zhu P, Yang J, Liu X, Dong S, Wang X, Chun B, Zhuang J, Zhang C. Ischaemic preconditioning-regulated miR-21 protects heart against ischaemia/reperfusion injury via anti-apoptosis through its target PDCD4. Cardiovasc Res. 2010;87:431–439. 75. Pan Z, Sun X, Shan H, Wang N, Wang J, Ren J, Feng S, Xie L, Lu C, Yuan Y, Zhang Y, Wang Y, Lu Y, Yang B. MicroRNA-101 inhibited postinfarct cardiac fibrosis and improved left ventricular compliance via the FBJ osteosarcoma oncogene/transforming growth factor-β1 pathway. Circulation. 2012;126:840–850. 1746 Arterioscler Thromb Vasc Biol August 2013 76.Chavakis E, Urbich C, Dimmeler S. Homing and engraftment of progenitor cells: a prerequisite for cell therapy. J Mol Cell Cardiol. 2008;45:514–522. 77. Mercola M, Ruiz-Lozano P, Schneider MD. Cardiac muscle regeneration: lessons from development. Genes Dev. 2011;25:299–309. 78. Porrello ER, Johnson BA, Aurora AB, Simpson E, Nam YJ, Matkovich SJ, Dorn GW 2nd, van Rooij E, Olson EN. MiR-15 family regulates postnatal mitotic arrest of cardiomyocytes. Circ Res. 2011;109:670–679. 79. Porrello ER, Mahmoud AI, Simpson E, Hill JA, Richardson JA, Olson EN, Sadek HA. Transient regenerative potential of the neonatal mouse heart. Science. 2011;331:1078–1080. 80. Dai L, Wang W, Zhang S, Jiang Q, Wang R, Dai L, Cheng L, Yang Y, Wei YQ, Deng HX. Vector-based miR-15a/16-1 plasmid inhibits colon cancer growth in vivo. Cell Biol Int. 2012;36:765–770. 81. Eulalio A, Mano M, Dal Ferro M, Zentilin L, Sinagra G, Zacchigna S, Giacca M. Functional screening identifies miRNAs inducing cardiac regeneration. Nature. 2012;492:376–381. 82. Ieda M, Fu JD, Delgado-Olguin P, Vedantham V, Hayashi Y, Bruneau BG, Srivastava D. Direct reprogramming of fibroblasts into functional cardiomyocytes by defined factors. Cell. 2010;142:375–386. 83. Qian L, Huang Y, Spencer CI, Foley A, Vedantham V, Liu L, Conway SJ, Fu JD, Srivastava D. In vivo reprogramming of murine cardiac fibroblasts into induced cardiomyocytes. Nature. 2012;485:593–598. 84. Song K, Nam YJ, Luo X, Qi X, Tan W, Huang GN, Acharya A, Smith CL, Tallquist MD, Neilson EG, Hill JA, Bassel-Duby R, Olson EN. Heart repair by reprogramming non-myocytes with cardiac transcription factors. Nature. 2012;485:599–604. 85. Cai B, Li J, Wang J, et al. microRNA-124 regulates cardiomyocyte differentiation of bone marrow-derived mesenchymal stem cells via targeting STAT3 signaling. Stem Cells. 2012;30:1746–1755. 86. Jayawardena TM, Egemnazarov B, Finch EA, Zhang L, Payne JA, Pandya K, Zhang Z, Rosenberg P, Mirotsou M, Dzau VJ. MicroRNA-mediated in vitro and in vivo direct reprogramming of cardiac fibroblasts to cardiomyocytes. Circ Res. 2012;110:1465–1473. 87.Stenvang J, Petri A, Lindow M, Obad S, Kauppinen S. Inhibition of microRNA function by antimiR oligonucleotides. Silence. 2012;3:1. 88. Büning H. Gene therapy enters the pharma market: the short story of a long journey. EMBO Mol Med. 2013;5:1–3. 89. Shah SJ, Wasserstrom JA. SERCA2a gene therapy for the prevention of sudden cardiac death: a future theranostic for heart failure? Circulation. 2012;126:2047–2050. Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 MicroRNAs in Stem Cell Function and Regenerative Therapy of the Heart Florian H. Seeger, Andreas M. Zeiher and Stefanie Dimmeler Arterioscler Thromb Vasc Biol. 2013;33:1739-1746 doi: 10.1161/ATVBAHA.113.300138 Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2013 American Heart Association, Inc. All rights reserved. Print ISSN: 1079-5642. Online ISSN: 1524-4636 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://atvb.ahajournals.org/content/33/8/1739 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online at: http://atvb.ahajournals.org//subscriptions/