Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Evolution of metal ions in biological systems wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Metabolic network modelling wikipedia , lookup
Proteolysis wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
Blood sugar level wikipedia , lookup
Glyceroneogenesis wikipedia , lookup
Basal metabolic rate wikipedia , lookup
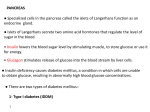
Regulation of Metabolism Nutritional Requirements • Living tissue is maintained by constant expenditure of energy (ATP). • Indirectly from glucose, fatty acids, ketones, amino acids, and other organic molecules. • Energy of food is commonly measured in kilocalories. • One kilocalorie is = 1000 calories. • One calorie = amount of heat required to raise the temperature of 1 cm3 of H20 from 14.5o to 15.5o C. • The amount of energy released as heat when food is combusted in vitro = amount of energy released within cells through aerobic respiration. Metabolic Rate and Caloric Requirements • Metabolic rate is the total rate of body metabolism. • Metabolic rate measured by the amount of oxygen consumed by the body/min. • Basal metabolic rate (BMR): • Oxygen consumption of an awake relaxed person 12–14 hours after eating and at a comfortable temperature. • Basal metabolic rate determined by: • • • • Age. Gender. Body surface area. Thyroid secretion. Anabolic Requirements • Anabolism: • Food supplies raw materials for synthesis reactions. • Synthesize: • • • • DNA and RNA. Proteins. Triglycerides. Glycogen. • Must occur constantly to replace molecules that are hydrolyzed. Aerobic Requirements (continued) • Catabolism: • Hydrolysis (break down monomers down to C02 and H20.): • • • • Hydrolysis reactions and cellular respiration. Gluconeogenesis. Glycogenolysis. Lipolysis. Turnover Rate • Rate at which a molecule is broken down and resynthesized. • Average daily turnover for carbohydrates is 250 g/day. • Some glucose is reused to form glycogen. • Only need about 150 g/day. • Average daily turnover for protein is 150 g/day. • Some protein may be reused for protein synthesis. • Only need 35 g/day. • 9 essential amino acids. • Average daily turnover for fats is 100 g/day. • Little is actually required in the diet. • Fat can be produced from excess carbohydrates. • Essential fatty acids: • Linoleic and linolenic acids. Vitamins and Minerals • Vitamins: • Small organic molecules that serve as coenzymes in metabolic reactions or have highly specific functions. • Must be obtained from the diet because the body does not produce them, or does so in insufficient amounts. • 2 classes of vitamins: • Fat-soluble: • A,D, E, and K. • Water-soluble: • B1, B2, B3, B6, B12, pantothenic acid, biotin, folic acid, and vitamin C. Vitamins • Water-soluble vitamins: • Serve as coenzymes in the metabolism of carbohydrates, lipids, and proteins. • May serve as antioxidants. • Fat-soluble vitamins: • Bind to nuclear receptors. • Serve as antioxidants. • Assist in regulation of fetal development. • Regulate Ca2+ balance. The Major Vitamins Minerals • Needed as cofactors for specific enzymes and other critical functions. • Trace elements: • Required in small amounts from 50 mg to 18 mg/day. Free Radicals and Antioxidants • Electrons are located in orbitals. • Each orbital contains a maximum of 2 electrons. • Free radical: • When an orbital has an unpaired electron. • Highly reactive in the body. • Oxidize or reduce other atoms. • Major free radicals called: • Reactive oxygen or nitrogen species: • Oxygen or nitrogen as unpaired electron. Free Radicals and Antioxidants (continued) • Functions of free radicals: • Help to destroy bacteria. • Produce vasodilation. • NO radical, superoxide radical, and hydroxy radical. • Exert oxidative stress contributing to disease states. • Excess production of free radicals can damage lipids, proteins, and DNA. • Promotes apoptosis, contributes to aging, inflammatory disease, heart disease, Cerebral Vascular Accident, hypertensive nephropathy, and degenerative disease. • Promotes malignant growth. • Protective mechanism against oxidative stress. • Can react with free radicals by picking up unpaired electrons. • Glutathione, vitamin C, and vitamin E. Reactive Oxygen Species Normal physiology requires that the reactive oxygen species (those that contain oxygen with an unpaired electron) be kept in balance. Regulation of Energy Metabolism • Energy reserves: • Molecules that can be oxidized for energy are derived from storage molecules (glycogen, protein, and fat). • Circulating substrates: • Molecules absorbed through small intestine and carried to the cell for use in cell respiration. Insert fig. 19.2 Eating • Eating behaviors partially controlled by hypothalamus. • Lesions in vetromedial area produce hyperphagia (obesity). • Lesions in lateral hypothalamus produces hypophagia (weight loss). • Endorphins, norepinephrine, serotonin, and CCK affect hunger and satiety. Regulatory Functions of Adipose Tissue • Adipostat regulatory system (negative feedback loops) to defend amount of adipose tissue. • Differentiation of adipocytes require nuclear receptor protein (PPARg) which is activated when bound to prostaglandin: • Stimulates adipogenesis by promoting development of preadipocytes into mature adipocytes. • Number of adipocytes increase after birth. • Differentiation promoted by high [fatty acids]. • Adipocytes store fat within large vacuoles. • May secrete hormones involved in regulation of metabolism. Regulatory Functions of Adipose Tissue (continued) • Leptin: • Hormone that signals the hypothalamus to indicate the level of fat storage. • Involved in long-term regulation of eating. • Satiety factor in obese have decreased sensitivity to leptin in the brain. • Neuropeptide Y: • Potent stimulator of appetite. • Functions as a neurotransmitter within the hypothalamus. • These neurons are inhibited by leptin. • Tumor necrosis factor-alpha (TNFa): • Acts to reduce the sensitivity of cells to insulin. • Increased in obesity. • May contribute to insulin resistance. Regulation of Hunger • Adipose tissue secrete satiety factor: • Acts through its regulation of hunger centers in hypothalamus. • Ghrelin: • Secreted by stomach. • Secretions rise between meals and stimulate hunger. • CCK: • Secretions rise during and immediately after a meal. • Produce satiety. • Peptide tyrosine tyrosine or pancreatic peptide PYY3-36: • Acts within the hypothalamus. • Decreases neuropeptide Y. Obesity • Obesity is often diagnosed by using a body mass index (BMI). BMI = w h2 • w = weight in kilograms • h = height in meters • Healthy weight as BMI between 19 – 25. • Obesity defined as BMI > 30. • Obesity in childhood is due to an increase in both the size and the # of adipocytes. • Weight gains in adulthood is due to increase in adipocyte size in intra-abdominal fat. Calorie Expenditures • 3 components: • Basal metabolic rate (BMR): • 60% total calorie expenditure. • Adaptive thermogenesis: • 10% total calorie expenditure. • Physical activity: • Contribution variable. Hormonal Regulation of Metabolism • Absorptive state: • Absorption of energy. • 4 hour period after eating. • Increase in insulin secretion. • Postabsorptive state: • Fasting state. • At least 4 hours after the meal. • Increase in glucagon secretion. Balance Between Anabolism and Catabolism • The rate of deposit and withdrawal of energy substrates, and the conversion of 1 type of energy substrate into another; are regulated by hormones. • Antagonistic effects of insulin, glucagon, GH, T3, cortisol, and Epi balance anabolism and catabolism. Insert fig. 19.4 Energy Regulation of Pancreas • Islets of Langerhans contain 3 distinct cell types: • a cells: • Secrete glucagon. • b cells: • Secrete insulin. • D cells: • Secrete somatostatin. Regulation of Insulin and Glucagon • Mainly regulated by blood [glucose]. • Lesser effect: blood [amino acid]. • Regulated by negative feedback. • Glucose enters the brain by facilitated diffusion. • Normal fasting [glucose] is 65–105 mg/dl. Regulation of Insulin and Glucagon (continued) •When blood [glucose] increases: • Glucose binds to GLUT2 receptor protein in b cells, stimulating the production and release of insulin. •Insulin: • Stimulates skeletal muscle cells and adipocytes to incorporate GLUT4 (glucose facilitated diffusion carrier) into plasma membranes. • Promotes anabolism. Oral Glucose Tolerance Test • Measurement of the ability of b cells to secrete insulin. • Ability of insulin to lower blood glucose. • Normal person’s rise in blood [glucose] after drinking solution is reversed to normal in 2 hrs. Insert fig. 19.8 Regulation of Insulin and Glucagon • Parasympathetic nervous system: • Stimulates insulin secretion. • Sympathetic nervous system: • Stimulates glucagon secretion. • GIP: • Stimulates insulin secretion. • GLP-1: • Stimulates insulin secretion. • CCK: • Stimulates insulin secretion. Regulation of Insulin and Glucagon Secretion (continued) • The secretion from the β (beta) cells and α (alpha) cells of the pancreatic islets is regulated largely by the blood glucose concentration. • A high blood glucose concentration stimulates insulin and inhibits glucagon secretion. • A low blood glucose concentration stimulates glucagon and inhibits insulin secretion. Absorptive State • Insulin is the major hormone that promotes anabolism in the body. • When blood [insulin] increases: • Promotes cellular uptake of glucose. • Stimulates glycogen storage in the liver and muscles. • Stimulates triglyceride storage in adipose cells. • Promotes cellular uptake of amino acids and synthesis of proteins. Postabsorptive State • Maintains blood glucose concentration. • When blood [glucagon] increased: • Stimulates glycogenolysis in the liver (glucose-6phosphatase). • Stimulates gluconeogenesis. • Skeletal muscle, heart, liver, and kidneys use fatty acids as major source of fuel (hormone-sensitive lipase). • Stimulates lipolysis and ketogenesis. Effect of Feeding and Fasting on Metabolism Insert fig. 19.10 • Metabolic balance is tilted toward anabolism by feeding (absorption of a meal) and toward catabolism by fasting. • This occurs because of an inverse relationship between insulin and glucagon secretion. • Insulin secretion rises and glucagon secretion falls during food absorption, whereas the opposite occurs during fasting. Hypoglycemia • Over secretion of insulin. • Reactive hypoglycemia: • Caused by an exaggerated response to a rise in blood glucose. • Occurs in people who are genetically predisposed to type II diabetes. Insert fig. 19.13 Metabolic Regulation • Anabolic effects of insulin are antagonized by the hormones of the adrenals, thyroid, and anterior pituitary. • Insulin, T3, and GH can act synergistically to stimulate protein synthesis. Metabolic Effects of Catecholamines • Metabolic effects similar to glucagon. • Stimulate glycogenolysis. • Stimulate release of glucose from the liver. • Stimulate lipolysis and release of fatty acids. • NE stimulates b3 receptors in brown fat. • Contains uncoupling protein that dissociates electron transport from ATP production. Metabolic Effects of Catecholamines (continued) Cyclic AMP (cAMP) serves as a second messenger in the actions of epinephrine and glucagon on liver and adipose tissue metabolism. Metabolic Effects of Glucocorticoids • Glucocorticoids secreted in response to release of Adrenocorticotropic hormone (ACTH). • Support the effects of increased glucagon. • Promote lipolysis and ketogenesis. • Promote protein breakdown in the muscles. • Increases blood [amino acids]. • Promote liver gluconeogenesis. Thyroxine • Active form is T3. • Stimulates cellular respiration by: • Production of uncoupling proteins. • Stimulation of active transport Na+/K+ pumps: • Lowers cellular [ATP]. • Increases metabolic heat. • Increases metabolic rate. • Contributes to proper growth and development of CNS in children. Growth Hormone (Somatotropin) • Inhibited by somatostatin. • Stimulates growth in children and adolescents. • Stimulated by: • GHRH. • Increase in blood [amino acids]. • Decrease in blood [glucose]. • Pulsatile, increasing during sleep, decreasing during day. Growth Hormone (continued) • IGF-1: • Liver produces and secretes IGF-1 in response to GH. • Stimulates cell division and growth of cartilage. • IGF-2: • Has more insulin-like actions. • Promotes anabolism and catabolism. • Stimulates cellular uptake of amino acids and protein synthesis. • Decreases glucose utilization by the tissues. • Raises blood [glucose]. Effects of Growth Hormone on Body Growth • Gigantism: • Excess GH secretion in children. • Maintain normal body proportions. • Acromegaly: • Excess GH secretion in adults after the epiphyseal discs are sealed. • No increase in height. • Growth of soft tissue. • Elongation of jaw, deformities in hands, feet, and bones of face. • Dwarfism: • Inadequate secretion of GH during childhood. Progression of Acromegaly Bone Deposition and Resorption • Ca2+ and phosphate concentrations are affected by: • Bone formation and resorption. • Intestinal absorption of Ca2+ and P043-. • Urinary excretion. • Osteoblasts: • Secrete an organic matrix of collagen proteins. • Deposit hydroxyapatite crystals. • Osteoclasts: • Secrete enzymes to dissolve hydroxyapatite. • Formation and resorption of bone occur constantly at rates determined by osteoblasts and osteoclasts. Bone Deposition and Resorption (continued) • Bone resorption occurs when an osteoclast attaches to the bone matrix and forms ruffled membrane. • Osteoclast secretes products that dissolve both Ca2+ and P043- ; and digest the matrix. • Transport of H+ by H+ ATPase pump in ruffled border. • Cl- channel allows Cl- to flow to H+ to maintain electrical neutrality. • Protein matrix digested by cathepsin K. • Cytoplasm prevented from becoming to basic by a Cl-/HC03- pump. Bone Deposition and Resorption (continued) • Figure depicting the mechanism of bone resorption. • Notice that the bone is first demineralized by the dissolution of calcium phosphate (CaPO4) from the matrix due to acid secretion by the osteoclast. • After that, the organic component of the matrix (mainly collagen) is digested by the secretion of enzyme molecules (an enzyme called cathepsin K) from the osteoclast. Parathyroid Hormone (PTH) • Single most important hormone in the control of blood [Ca2+]. • Stimulated by decreased blood [Ca2+]. • Stimulates osteoclasts to reabsorb bone. • Stimulates kidneys to reabsorb Ca2+ from glomerular filtrate, and inhibit reabsorption of P043-. • Promotes formation of 1,25 vitamin D3. • Many cancers secrete PTH-related protein that interacts with PTH receptors. • Produce hypercalcemia. Calcitonin • Works with PTH and 1,25 vitamin D3 to regulate blood [Ca2+]. • Stimulated by increased plasma [Ca2+]. • Inhibits the activity of osteoclasts. • Stimulates urinary excretion of Ca2+ and P043- by inhibiting reabsorption. • Physiological significance in adults is questionable. Vitamin D3 • Pre-vitamin D3 is synthesized in the skin when exposed to midultraviolet waves. • Pre-vitamin D3 isomerized to vitamin D3 (cholecalciferol). • Cholecalciferol is hydroxylated in liver to form 25 hydroxycholecalciferol. • In proximal convoluted tubule is hydroxylated to 1,25 dihydroxycholecalciferol (active vitamin D3). • Stimulated by PTH. Production of dihydroxyvitamin D3 Insert fig. 19.20 • This hormone is produced in the kidneys from the inactive precursor 25hydroxyvitamin D3 (formed in the liver). • The latter molecule is produced from vitamin D3 secreted by the skin. dihydroxyvitamin D3 (continued) • Directly stimulates intestinal absorption of Ca2+ and P043-. • When Ca2+ intake is inadequate, directly stimulates bone reabsorption. • Stimulates reabsorption of Ca2+ and P043- by the kidney. • Simultaneously raising Ca2+ and P043- results in increased tendency of these 2 ions to precipitate as hydroxyapatite crystals. • Stimulated by Parathyroid hormone (PTH). Negative Feedback Control A negative feedback loop returns low blood Ca2+ concentrations to normal without simultaneously raising blood phosphate levels above normal. Negative Feedback Control • The action of calcitonin is antagonistic to that of parathyroid hormone.