Survey
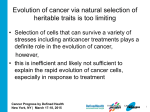
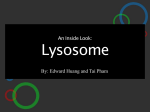
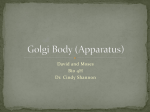
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
SPOTLIGHT REVIEW Cardiovascular Research (2014) 102, 302–311 doi:10.1093/cvr/cvu022 Microvesicles and exosomes for intracardiac communication Joost P.G. Sluijter 1,2*, Vera Verhage 1, Janine C. Deddens 1, Frederieke van den Akker1, and Pieter A. Doevendans 1,2 1 Department of Cardiology, University Medical Center Utrecht, Utrecht, The Netherlands; and 2ICIN - Netherlands Heart Institute, Utrecht, The Netherlands Received 18 November 2013; revised 16 December 2013; accepted 20 December 2014; online publish-ahead-of-print 30 January 2014 The heart is an organ with a complex mixture of well-organized interactions of different cell types that facilitate proper myocardial contractility, sufficient perfusion, balanced myocardial extracellular stiffness, and controlled functioning of the immune system. Several cell types, including cardiomyocytes, endothelial cells, smooth muscle cells, fibroblasts, immune cells, and cardiac-derived stem cells, need a well-controlled communication system to use the complex orchestra of signalling molecules. The intercellular communication includes direct cell –cell contact, cell– matrix interaction, long-range signals, and electrical and extracellular chemical molecules. In addition to the extracellular molecules that cells can use to influence their environment, more and more attention is focused on the release of extracellular membrane vesicles by cells. These vesicles were always thought to be cell debris derivatives, but it appeared that these vesicles are used for horizontal transfer of information between cells, containing proteins, peptides, several classes of RNA molecules, and sometimes DNA. The main populations of released vesicles are classified on their (intra)cellular origin and include apoptotic bodies, microvesicles, and exosomes. Here, we provide an overview on the role of vesicles in cardiac communication and their use as potential therapeutics and biomarkers. ----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords Vesicles † Exosomes † Cell communication † Biomarkers ----------------------------------------------------------------------------------------------------------------------------------------------------------- This article is part of the Spotlight Issue on: Heterocellular signalling and crosstalk in the heart in ischaemia and heart failure. 1. Cellular communication and vesicle release Communication is a key feature in biology, in which signalling of information by one organism to another is usually intended to alter the recipient’s behaviour. Whereas communication between individuals is mediated via visual, olfactory, auditory, electrical, or tactile signals, cells in multicellular organisms communicate with each other via other mechanisms, including direct cell– cell contact, cell– matrix interaction, long-range signals, electrical signals, and via extracellular chemical molecules such as proteins, nucleotides, lipids, and short peptides (see Figure 1). As with individuals, cells try to communicate warning or propagation signals to neighbouring cells to alert them or to change their behaviour for maintaining organ homeostasis or as a response to stress signals. In addition to the extracellular molecules that cells can use to influence their environment, more and more attention is focused on the release of extracellular membrane vesicles. These vesicles were once thought to be cell debris derivatives, as first identified by Wolf et al. in 1967 as procoagulant ‘dust’ from blood platelets,1 but it appears that cells can produce many different types of vesicles, thereby influencing their direct environment or using them as long-distance vehicles to cells and organs in other regions of the organism. The vesicles released by cells have a lipid bilayer and contain a cell-specific cargo of proteins, lipids, and genetic material and can influence the cells they encounter via different mechanisms to alter their function and behaviour. Vesicle uptake is mediated via direct binding with membrane surface molecules, endocytotic internalization, or fusion with the recipient plasma membrane and subsequent delivery of its cargo.2,3 A growing body of evidence demonstrates that the production of vesicles is a universal feature of cellular life. The ability of vesicles to transport different molecules and their general distribution makes them attractive candidates for horizontal cellular gene transfer.4 Although the release of vesicles to influence other cells seems to be straightforward, multiple mechanisms, size distributions, and RNA profiles5 are observed among different vesicles released by cells. Unfortunately, there is no clear consensus on the nomenclature and associated characteristics of different vesicle.6 Conventional analysis of the secreted membrane vesicles, including histological assessments, laser confocal microscopy, and flow cytometry, has substantial resolution limitations and therefore it was not until recently that the process of vesicle release as a universal adaptive cellular response was confirmed.7,8 The main populations of vesicles released are usually * Corresponding author. Department of Cardiology, Division Heart and Lungs, University Medical Center Utrecht, Heidelberglaan 100, room G02.523, 3584 CX Utrecht, the Netherlands. Tel: +31 88 755 7155; fax: +31 30 252 2693, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2014. For permissions please email: [email protected]. 303 Vesicles for intracardiac communication Figure 1 Cellular communication in multicellular organs is established via different mechanisms. Well-studied forms of cellular communication are (1) direct cell – cell contact for which cells are connected via gap junctions or adherent proteins to facilitate signal propagations, (2) cell – matrix interactions that is facilitated by integrin molecules that allow cell to sense stresses on the extracellular matrix and respond adequately, (3) long-range signals, which are released in the blood stream, including, for example, hormones, to control stresses and cell behaviour, and (4) electrical and chemical signals such as proteins (SDF-1, HGF, FGF/RA), nucleotides, lipids, and short peptides to control the direct environment. classified by their intracellular origin and include apoptotic bodies, microvesicles, and exosomes (see Figure 2).9 2. Vesicle biogenesis 2.1 Apoptotic bodies Apoptosis is a process that allows an efficient and immunological silent clearing of damaged cells that can be difficult to monitor in vivo. Apoptosis is normally characterized by several morphological specifications, including cell contraction, nuclear condensation, fragmentation, and release of apoptotic bodies.10 Apoptotic bodies, or vesicles, are 1–5 mm in diameter (approximately the size range of platelets) and released from the plasma membrane as blebs when cells undergo apoptosis. They are characterized by phosphatidylserine externalization, which contain several intracellular fragments and cellular organelles, including histones and fragmented DNA.9 Apoptotic bodies are closed structures, generally thought to float on a sucrose gradient at a density between 1.16 and 1.28 g/mL. Their release is dependent on Rho-associated kinase I (ROCK) and myosin ATPase activity. Whereas the activity of ROCK proteins is both necessary and sufficient for formation of membrane blebs, and for re-allocation of fragmented DNA into blebs and apoptotic bodies,11 the role of apoptotic bodies is still not clear. Body formation could provide an easier system for cellular clearance, since they are smaller than a cell and are therefore easier to phagocytose.12 Alternatively, bodies might be used as an active signal to promote cell clearance of the remaining damaged cell.13 2.2 Microvesicles Microvesicles are a class of vesicles that have been described in several areas, often called microparticles, ectosomes, and membrane particles, ranging in size between 100 and 1000 nm in diameter and generated by outward budding or blebbing of the plasma membrane. These vesicles float on different levels in a sucrose gradient, predominantly seen at a density of 1.04–1.07 g/mL, and no clear markers have been identified.7 They have been predominantly characterized as products of platelets, red blood cells, and endothelial cells. Microvesicles are generated and shed from cells during various processes and stimuli, during cellular differentiation or senescence, exposure to high shear stress, or upon pro-inflammatory or pro-thrombotic stimulations, for example.14 Enhanced microvesicle release from cells is observed upon increased intracellular calcium, thereby changing phospholipid positions, flipping phosphatidyl-serine from the inside to the outside part of the membrane.15 Calcium-sensitive proteolytic enzymes like calpain and gelsolin are subsequently activated and enable vesiculation by detaching membrane proteins from the intracellular cytoskeleton.16 Microvesicles can 304 J.P.G. Sluijter et al. Figure 2 Cells are able to release different classes of vesicles into their environment and thereby have an additional form of communication that allows them to control their actions. The main populations of vesicles are released upon different stress signals, including thrombin, DNA damage, intracellular calcium, extracellular ATP, LPS, and hypoxia, and are classified based on their intracellular origin and include apoptotic bodies, microvesicles, and exosomes. Microvesicles are 100 – 1000 nm in diameter and generated by outward budding or blebbing of the plasma membrane. Exosomes are 40 – 100 nm in size and originate from the inward budding of the late endosomal membrane of multivesicular bodies (MVB), resulting in the formation of intraluminal vesicles and involves the endosomal sorting complex required for transport (ESCRT) machinery for content sorting and Alix, Tsg101, clathrin, Hsp70, rabs, and others for subsequent formation and functioning. The intraluminal vesicles are released by the cells through fusion of the MVB with the cell membrane. Apoptotic bodies or vesicles are 1 – 5 mm in diameter, released from the plasma membrane as blebs when cells undergo apoptosis, and contain several intracellular fragments and cellular organelles. Their release is dependent on Rho-associated kinase I (ROCK) and myosin ATPase activity. contain a spectrum of bioactive molecules, including several membrane receptors, adhesion structures, cytokines, chemokines, growth factors, and even different RNA species, including functional mRNA and miRNAs.17,18 Although miRNAs are found to be regularly expressed in exosomes, which are easily detectable, their effects are dose dependent in target cells and it therefore remains to be determined how effective this communication is. It is generally accepted that the nature of cell activation and the direct cellular environment determine microvesicle composition and thereby their behaviour in intercellular communication. 2.3 Exosomes Exosomes are the best characterized class of vesicles ranging between 40 and 100 nm in size, and represent a specific subset due to the intracellular origin from the endosomes. The inward budding of the late endosomal membrane of multivesicular bodies (MVB) results in the formation of intraluminal vesicles. These vesicles are the origin of exosomes, and are released by the cells through fusion of the MVB with the cell membrane. Although it was previously thought that MVB fuse with lysosomes for degradation, different sorting processes are involved in defining whether these intraluminal vesicles are released into the extracellular environment or destined for degradation. The endosomal system controls both the uptake and processing of various molecules from the extracellular environment, and exchanges proteins and lipids with the trans-Golgi network (TGN),19 thereby regulating the dynamic state of multiple receptors recycling between the cell surface, endosomes, and the TGN to maintain cell homeostasis. Therefore, exosomes likely have controlled contents that reflect the cellular origin and physiological state of the cell. Since their discovery by Harding et al. 20 30 years ago, they have only recently gained much interest. This is likely due to technical advancements and a better understanding of their functions, such as their potential to modulate the immune system,21 transfer genetic material,4 and influence cell behaviour over 305 Vesicles for intracardiac communication long distances.22 They are functionally stable in lymph nodes for at least 3 days23 and might therefore be useful as biomarkers.24 Electron microscopy (EM) is the only technique that allows visualization of exosomes. Usually, these vesicles are able to float on a sucrose gradient at a density of 1.13–1.19 g/mL. Markers that are enriched on exosomes for their identification are Alix, TSG101, flottilin, and tetraspanins, which are incorporated during their biogenesis. Exosomes contain tetraspanins (CD81, CD63, and CD9), which play an important role in cell penetration, invasion, and fusion events, as well as proteins related to MVB biogenesis (Alix, TSG101, and clathrin), heat shock protein 70 (HSP70), and RABs that regulate exosome docking and membrane fusion.25 Exosomes also contain annexins, metabolic enzymes, ribosomal proteins, signal transduction molecules, adhesion molecules, ATPases, cytoskeletal and ubiquitin molecules, growth factors, cytokines, mRNA, and microRNA (miRNA) molecules.26,4 An exosome protein and RNA database (Exo-Carta) is available at http://www.exocarta.org/. In addition to molecules shared between exosomes from multiple cell types, exosomes carry specific proteins from their parental cell type. It has been shown that mRNAs, carried by exosomes, can be translated into proteins in the target cell. In addition, miRNAs can be functionally transferred to recipient cells and subsequently silence gene expression,27 which indicates that exosomes can act as a vector of genetic information. The biogenesis of exosomes is regulated via many signalling pathways, which is reflected in the complex architecture of exosomes in terms of content, composition, and specialized sorted proteins. Although the exact mechanisms are not well understood, different sorting processes have been identified. One of the processes involves the endosomal sorting complex required for transport (ESCRT) machinery, which regulates protein sorting into the endosomal membrane and its inward budding.28 Alternatively, ESCRT-independent exosome formation has also been suggested based on lipid microdomains,29 lipid rafts,30 and tetraspanins.31 Exosomes are released from cells via two mechanisms; constitutive or inducible, depending on the cell type of origin.7 The constitutive secretion pathways are mediated by specific RAB GTPases,25,32 hetrotrimeric G-protein, and protein kinase D,33 while inducible secretion is regulated by various cell activation processes. These include several stimuli such as increased intracellular Ca2+,34,35 DNA damage,36,37 thrombin, extracellular ATP,38 hypoxia, and LPS39 stimulation. Cardiomyocytes in vitro nearly doubled their exosome release after 2 h of mild hypoxia.40 Interestingly, several of these inducers were shown to have cardioprotective effects as well.41,42 Exosome production is a tightly controlled process, which in some cells is partly dependent on p53 transcription genes,36 but also on lipid mediators, e.g. diacylglycerol. Currently, no clear characterizations and markers are available to mark and identify all these different extracellular vesicle populations during different experimental procedures. It is therefore important to report as much detail as possible on methodology and to obtain vesicle fractions. Next, we provide an overview of the current status of the role of extracellular vesicles in the intercellular communication of cardiac cells, thereby not only exploring their biological role but also future potential as therapeutics and biomarkers. This overview is far from complete due to the complex nature of vesicle release, and a relatively recent appreciation for the detailed level of study required for these processes and the technical advancements necessary to start exploring their role. The question of their necessity, since many of the processes described could be mediated through gap junctions, or how far these vesicle populations travel in vivo, and why it might be crucial to communicate with cells at a distance, remain unanswered. 3. Cardiac cell communication: a role in physiology and disease Effective myocardial function is a complex mixture of well-organized interactions of different cell types that facilitate proper myocardial contractility, sufficient perfusion, balanced myocardial extracellular stiffness, and controlled functioning of the immune system. The heart contains 3 billion cardiac muscle cells, which represents only a third of the total cell numbers in the heart. It further consists of endothelial cells, smooth muscle cells, fibroblasts, immune-system-related cells, sympathetic and parasympathetic neuronal cells, and recently discovered cardiac-derived stem cells.43 All these cells are organized in a complex structure and, as a consequence, a tight balance exists between these cell types to maintain the integrity of the heart. To guarantee this balance, intra- and intercellular communication are essential features. Several forms of haemodynamic stress, either physiological or pathological, including hypertension, myocardial infarction (MI), valvular irregularities, but also pregnancy,44 lead to increased intracardiac pressures and/or volumes, resulting in myocardial cellular responses, e.g. a hypertrophic response. The cardiac responses to specific (patho-) physiological stimuli is mediated by intrinsic signalling pathways within cardiomyocytes, but is also due to crosstalk between these myocytes and other cell types in the heart. As mentioned above, many routes of communication exist to cope with the changing environmental cues, including autocrine factors, cell –cell propagations, gap-junctional communication, and adhesion complex interactions (see Figure 1). Several factors that are well studied for their interactions during cardiac responses include leptin, TGF-beta family members, hepatocyte growth factor, endothelin-1 (ET-1), and SDF-1, but their vesicle-bound contributions are not known. The heart requires a lot of oxygen, even more so than skeletal muscle at rest, and the vasomotor control of the coronary arteries illustrates in particular the efficient communication and maintenance of the oxygen supply to the heart in response to exercise. Endothelial cells release vasodilating and vasoconstricting factors, including nitric oxide (NO), ET-1, ANG-II, and VEGF,45 under the influence of neurohormonal, endothelial, and metabolic signals to increase the blood flow in the heart. Although direct binding of these released factors to influence vasomotor control is a major factor, the contribution of factors as being vesicle bound as well is not clear. Not surprisingly, during cardiac development, important paracrine signalling pathways, such as Wnt, fibroblast growth factors (FGF), and retinoic acid (RA), also play important roles in balancing proliferation and differentiation of the forming myocardium.46 It was conventionally thought that cells release these proteins into their environment and thereby stimulate neighbouring cells; however, more and more evidence indicates that vesicle-bound proteins are also released. This indicates that via vesicles they facilitate another mechanism of cellular communication containing similar factors, like a mechanism of Wnt transmission through release of exosome-like vesicles containing a Wnt-binding protein.47 Depending on the mechanism of action on target cells and the needed receptor molecules on their cell membranes, it might be suggested that the release of free factors like growth factors into the cell surroundings is less controlled. The release of molecules via vesicles might be better 306 J.P.G. Sluijter et al. Figure 3 Within the myocardium, different cell types communicate with each other via different vesicles with a specific content. These vesicles originate from the endothelium, thereby influencing smooth muscle cells, fibroblasts, cardiomyocytes, and also immune-cells but also from these non-endothelium cells to facilitate a proper response to environmental changes and maintenance of myocardial homeostasis. Additionally, stem cell-released vesicles are suggested to stimulate repair mechanisms upon injection. Several of the released vesicles from the myocardium are also detectable as biomarkers in the blood reflecting myocardial damage or local and systemic stress responses, highlighting the diversity of the role and use of extracellular vesicles. organized due to vesicle-mediated release and uptake, since both are being regulated by cell-specific release of host cells and receptor-specific target cell uptake, and thereby provide a better control on the complex orchestra of environmental signals (see Figure 3). 4. Cardiomyocyte vesicle release Cardiomyocytes are generally not considered a typical secretory cell, but in addition to several cytokines, chemokines, and factors like ANP, BNP, TGF-b, TNF-a, also microvesicles and exosomes called cardiosomes, are released from adult mouse heart-derived cardiomyocytes. HL-1 cells, a cell model of cardiomyocytes which was derived from a mouse atrial cardiomyocyte tumour,48 secrete microvesicles which were obtained by a stepwise centrifugation protocol, and identified by EM and positive signals on western blot for Flotilin and partly by caveolin-3. Several signs indicated heterogeneity in vesicle appearance, including size distributions, ranging in size from 40 to 300 nm, and surface antigens, which could imply differences in cargo as well as potential target cells. These obtained myocyte vesicles were able to change gene expression in fibroblasts during 48 h of co-incubation. However, due to the broad size range of these vesicles, indicating a mixed population, results are difficult to interpret with respect to the specific vesicle type.49 HSPs are an essential family of protective proteins and have important roles in protein folding, protein trafficking, and cell signalling.50 HSP60 is a mitochondrial and cytosolic protein that has been detected in the extracellular space, but the form is unknown. It was suggested that HSP60 could have a role as a ligand of toll-like receptor (TLR) 4, and thereby as a possible danger signal for the immune system.51 Although not characterized in detail, exosomes were isolated by centrifugation of supernatant from isolated neonatal rat primary cardiomyocytes and were increased upon hypoxia. Isolated exosomes contained HSP60, and are the main source of HSP60 release, and thereby potentially affect the environment and release into circulation under physiological as well as pathological conditions.40,52 Another factor released by the myocardium upon acute MI (AMI) is tumour necrosis factor-a (TNF-a), which was observed to be elevated in the plasma of patients, thereby contributing to myocardial injury and dysfunction.53 Interestingly, TNF-a was observed to be mainly released via Hif-1a-mediated non-classical secretory pathways, involving release of vesicles containing a membrane variant of TNF. The identified vesicles were suggested to be exosomes and, when obtained from hypoxic cardiomyocytes, could trigger cell death in other cardiomyoctes.54 Interestingly, a population of TNF receptor (TNFR1) exosome-like vesicles were also found to circulate in human plasma, which could modulate TNF-mediated inflammation.55 Moreover, exosomes collected from cardiomyocytes in culture and exposed to different growth factors had a changed content.56 Although still in an infant stage, these studies suggest the existence of cardiomyocyte-released vesicles and their contribution to specific disease signalling and progression, and permit a reevaluation of our understanding of how these molecules are released and affect their environment. 5. Vesicles and cardiac remodelling/ fibrosis Myocardial injury induces cardiomyocyte death and destroys the vasculature, thereby leading to several effects to stimulate repair and maintain cardiac integrity, including cardiac fibrosis. Fibrosis is mainly mediated by the presence of collagen secreting myo-fibroblasts, which originate from 307 Vesicles for intracardiac communication endogenous fibroblasts but also from other cell sources, like endothelial cells and circulating cells.57 Fibrosis affects the architecture and thereby the structure of the heart, a process called cardiac remodelling. Considering the significant reorganization of the heart during cardiac remodelling, communication of several cell types is involved to create these changes, like a cross talk between cardiomyocytes and fibroblasts.58 Fibroblasts are a regulating and secreting cell type, not only involved in maintaining the extracellular environment of the myocytes. From culture experiments in which cardiomyocytes were cultured in the presence of cardiac fibroblasts, it became clear that, for example, IL-6 and TNF-a from the fibroblasts were able to induce hypertrophic responses and could modulate electrophysiological behaviour and contractility.59,60 Cellular communication is further highlighted by the plasticity of different cardiac cells, and their interactions to induce fibrosis, by a process that is called endothelial-to-mesenchymal transition (EndMT) to generate fibroblasts. This process is mediated by Snail, a zinc finger transcription factor induced in EC upon ischaemia/reperfusion, that is well known for its capacity to induce EndMT of EC and thereby contribute to cardiac fibrosis.57 In addition to this, EC start to release more connective tissue growth factor (CTGF) in their environment, a growth factor that is known to be induced in the infarcted heart and a regulator of fibrosis.61 CTGF is capable of stimulating quiescent fibroblasts to become secreting myofibroblasts and thereby further enhance the fibrotic response. By inhibition of Snail in EC, this cascade that leads to fibroblast formation could be inhibited and fibrosis reduced, and highlights the close communication and effects that can be reached by a combination of cell types.62 Interestingly, although different from the heart, injured kidney epithelial cells can promote the proliferation, alpha-smooth muscle actin expression, F-actin expression, and type I collagen production in surrounding fibroblasts.63 Epithelial cells undergo an epithelial-tomesenchymal transition (EMT),64 which overlaps to a high degree with EndoMT. Upon this transition, they produce an increased number of exosomes with defined genetic information to activate fibroblasts. This response is mediated via TGF-b1-containing exosomes, a growth factor that has a powerful role in matrix deposition like CTGF, and thereby initiates a tissue repair/regenerative responses, highlighting a potential use for exosome-targeted therapies to control tissue fibrosis.65 6. Vesicles in endothelial communication EC interact with smooth muscle cells (SMCs) during development, angiogenesis, and atherosclerotic lesion formation, thereby modulating their proliferation behaviour or apoptosis. Several growth factors which regulate these interactions have been identified and described.66 Recently, miRNAs were identified as tight regulators67 and EC were shown to secrete miR-126 and target SMCs, thereby regulating their turnover in vitro and in vivo in a paracrine manner. Although mediation via vesicles was studied, the authors observed that a non-vesicle fraction was responsible and that Argonaute-2-bound miR-126 was transferred to the SMCs, subsequently blocking forkhead box O3, B-cell lymphoma 2, and insulin substrate 1 mRNAs, while stimulating neointimal lesion formation.68 Although the responsible fraction was non-vesicle, part of miR-126 was present in vesicles but did not affect the SMCs. Interestingly, others have observed that endothelial apoptotic bodies can also contain miR-126, which could be internalized by neighbouring ECs, thereby changing their CXCL12 and RGS16 levels, and recruiting progenitor cells to stabilize and reduce atherosclerotic lesions.69 These examples clearly demonstrate that differences in EC vesicle secretions can be observed between normal and apoptotic conditions. Consequently, vesicles target other cell types and affect their behaviour differently via miR-126, and regulate lesion formation in opposite directions. Differences in EC vesicle content upon different exposures were further supported by recent findings in which EC-derived exosome content was affected both on an RNA and on a protein level when these cells were exposed to different cellular stress signals, including hypoxia, TNF-a stimulation, and high glucose and mannose concentrations. Interestingly, although the content changed, the size distribution of secreted vesicles did not differ significantly between the different conditions.70 Another example of EC-secreted vesicles was observed by Hergenreider et al., when Krüppel-like Factor 2 (KLF2) was induced in HUVECs and directly increased levels of miR-143/145. These were exported via vesicles to SMCs in which they changed gene expression into an athero-protective SMC phenotype. This led to a reduction in atherosclerotic lesion formation upon injection into ApoE2/2 mice.71 7. Vesicles and immune responses The immune system plays a role at different stages of cardiac disease. Exosome release from immune cells was noticed from the mid-1990s onwards72 and exosome-release from B cells, T cells, mast cells, and dendritic cells has been described.72 Immune cell-derived exosomes were found to aid in antigen presentation, immunoregulation, and signal transduction.73 Exosomes derived from immune cells mainly regulate other immune cells.72,74 However, when considering exosomes as a therapeutic option in cardiac disease, the influence of immune-derived exosomes can be crucial for two different processes. The first process concerns the tolerance and survival of cardiac allografts. Despite optimal matching, patients who undergo heart transplantation need to take a life-long course of immunosuppressive drugs with constant monitoring for graft rejection by T cells. Recently, it was discovered that exosomes derived from immature dendritic cells and regulatory T cells can suppress T-cell activation, leading to prolonged cardiac allograft survival.73,75,76 Although by itself this only replaces immunosuppressive drugs, studies combining exosomes with rapamycin appear to induce graft tolerance, which might make immunosuppressive drug therapy redundant in the future.75 Besides allograft tolerance, exosomes can interfere with the immune response during cardiac disease. During and after MI, the immune system becomes activated, leading to formation of pro-inflammatory and autoreactive immune cells.77 These cells continuously damage the heart, long after the initial damaging event has passed. Exosomes produced by macrophages, T cells, and dendritic cells can shift the inflammatory balance of this immune response.78 This shift leads to increased differentiation of anti-inflammatory and pro-healing immune cells including alternatively activated macrophages and regulatory T-cells, while the formation of pro-inflammatory immune subsets is suppressed. This change in immune cell subset could reduce or perhaps even halt progression towards heart failure after MI. 8. Small vesicles as biomarkers Microvesicle content as a reflection of the intracellular composition is dependent on the type and temporospatial status of the cell of 308 origin.70,2 For that reason, specific microvesicle profiles of extracellular fluid (e.g. blood, urine, cerebrospinal fluid, saliva) can be used for identification and detection of disease-specific biomarkers, without the need for a tissue biopsy. Since purification of microvesicles results in biomarker enrichment relative to the total secretome, small changes in microvesicle content can already be detected, which makes microvesicles and their content promising for biomarker development.79 Several studies have demonstrated the diagnostic potential of exosomeassociated proteins and nucleic acids, e.g. for kidney disease,80 inflammatory hepatic injury,81 metabolic disease,82 several cancer types,79 and in patients with clinically manifest vascular disease.83 Upon cardiac injury, extracellular microvesicles are released from activated platelets and apoptotic endothelial cells, which are associated to the area at risk during ST-elevation MI.84,85 The application of serum-derived microvesicles (proteins, miRNAs) as diagnostic biomarker for acute coronary syndrome (ACS) was not described before. However, recently it was demonstrated that serum-derived microvesicle-associated polygenic immunoglobin receptor, cystatin C, and complement factor C5a protein are markedly up-regulated in patients with ACS.86 This indicates that the content of serum-derived microvesicles, along with the well-known extravesicular markers cardiac troponin87 and CK-MB,88 and maybe miRNAs,89,90 might be useful as diagnostic biomarkers in the future in a patient population suspected of ACS. During coronary heart disease, microparticle release was altered in patients and demonstrated a change in miRNA content, thereby also being less able to transfer miRNAs to cultured HUVECs. This suggests not only a different content due to stress signals but also that surface proteins were affected and could alter their uptake.91 9. Therapeutic potential of extracellular vesicles In recent years, stem cell therapy has taken centre stage as an approach to both prevent cardiac damage and stimulate cardiac repair.92 Although animal models showed promising effects, clinical trials that were initiated using somatic stem cell transplantation have resulted in significant but limited positive effects on cardiac function.93,94 These studies have generally used the most convenient and accessible cells, rather than perhaps the most potent.95 Although the heart seems like a relatively simple organ in its cellular composition and organization, rebuilding it is still a major challenge. This is in part because its electrical activity has to be strictly controlled, scar tissue formation creates risks of arrhythmias, and communication between old and new cells has to be functional. Upon injection of cells into the diseased myocardium, cardiac regeneration can potentially be achieved via multiple mechanisms. Although actual differentiation of progenitor cells and active contribution to cardiac function is the main goal, the engraftment of progenitor cells and the number of newly generated cardiomyocytes and vascular cells are in most cases too low to account for the improvements in cardiac function and dimensions.96 – 98 Since it was postulated that stem cells mainly exert their current beneficial effects via paracrine factors,97,92 these factors from progenitor cells are of major interest and have extensively been studied with respect to the release of growth factors, cytokines, and chemokines. The most extensively studied cell type for paracrine cardiac cell therapy is the mesenchymal stem cell (MSC), which is known for its immune modulatory and regenerative capacity. In a model of acute MI, it has been shown that MSC-derived conditioned medium (CM) reduced infarct size in both murine and large animal J.P.G. Sluijter et al. models.99,100 Upon injection of concentrated CM from Akt-modified MSCs in infarcted rat hearts, apoptotic cell numbers were reduced and consequently infarct sizes were smaller.99 Additional research demonstrated that the exosome-containing fraction of MSC-CM was responsible for the preservation of cardiac function and prevention of adverse cardiac remodelling after ischaemia/reperfusion injury.101 These effects were mediated via decreased oxidative stress and activation of the PI3K/Akt pathway.102 Interestingly, not only MSCs have this effect, but also the secretome of peripheral blood cells was shown to be cardio-protective in a pre-clinical reperfusion injury porcine model.103 Additionally, cardiac progenitor cells (CPCs) are of great interest for their paracrine actions, since these cells originate from the heart itself.104 This means that they are possibly predisposed with signalling pathways necessary for cardiac regeneration. It has been demonstrated that CPC-derived exosomes stimulate migration of endothelial cells in vitro 105 and a recently published in vivo study hints towards cardioprotective effects of CPC exosomes in ischaemic myocardium.106 Likewise, progenitor cell populations in adult mouse hearts and in in vitro cultured human cardiospheres (CSs) were shown to release exosomes and microvesicles. These progenitor cells were unfortunately only identified by morphology, having a large nucleus to cytoplasm ratio. The authors observed nano-scale vesicles being released into the myocardium107 and indicated that these are an important mechanism involved in the heterocellular communication in the adult heart,108 especially between telocytes and resident progenitor cells. Recently, Sahoo et al. 109 demonstrated the paracrine angiogenic role of exosomes derived from CD34(+) cells in vitro and their potential to stimulate angiogenesis in both Matrigel plug assay and corneal assays. Moreover, the angiogenic activity was limited to exosomes from CD34(+) cells and not from CD34(+) cell-depleted mononuclear cells. They further identified the sonic hedgehog (Shh) protein to represent a major mechanism via which cardiac function was improved.110 Shh is a well-established angiogenic morphogen and is known to play important roles in cardiac development and postnatal ischaemic injury recovery.111 Stem cell therapy is an ongoing strategy to repair the damaged heart, which still needs further optimization to fulfil its promises. However, the use of the progenitor cell secretome, or more specifically their stable released vesicles, might be used for an off-the-shelf therapeutic application. These may circumvent many of the current hurdles associated with cell retentions, including the use of replicating cells as a direct therapeutic agent and the need for autologous cell culture. The use of these vesicles provides an alternative strategy for the paracrine effects of cell transplantation and activation of the repair mechanisms of the resident myocardium. 10. Conclusions The discovery, but more the acknowledgement, of the existence of several classes of extracellular vesicles used for inter-cellular or interorgan communication introduces a novel level and mechanism for information exchange between cells. Cells in the heart are able to use these vesicles to affect other cells and to pass on their status and environmental changes during normal cardiac homeostasis and upon pathological conditions. The extracellular vesicles contain a repertoire of proteins, peptides, mRNA, and miRNAs which are altered upon stress signal exposures. Cells can control the signals sent to others by changing the vesicle content or surface markers. The receiving cells can in turn control vesicle uptake. This tight control of information exchange Vesicles for intracardiac communication allows cells to better control the complex orchestra of environmental signals. Additionally, the dual role of microvesicles as biomarkers and active biological messenger creates opportunities to measure cellular temporal–spatial status and to gain more insight into the possibility to interfere with the biological targets of these released microvesicles. Finally, the therapeutic potential of (progenitor) cell-derived extracellular vesicles is promising, as they are a naturally occurring, efficient, therapeutic delivery vehicle that might be used to deliver therapeutics and drugs to specific cell types. Although interesting from a biological perspective, promising as a therapeutical approach, or source of novel biomarkers, we need to improve our understanding of how extracellular vesicles are produced by cells, and how their content is sorted and affects target cells. Complications of their therapeutic use in non-target organs, overstimulation in targeted cells, or stimulation of the immune-system are possible. Only after further research will we be able to intervene in pathological processes or employ their powerful effects to their full potential. Conflict of interest: none declared. Funding This work was supported by a grant from the Alexandre Suerman program for MD/PhD students of the University Medical Center, Utrecht, the Netherlands, the ZonMw-TAS program (#116002016), and the Netherlands CardioVascular Research Initiative (CVON): the Dutch Heart Foundation, Dutch Federation of University Medical Centers, the Netherlands Organization for Health Research and Development, and the Royal Netherlands Academy of Sciences. References 1. Wolf P. The nature and significance of platelet products in human plasma. Br J Haematol 1967;13:269 –288. 2. Chaput N, Théry C. Exosomes: immune properties and potential clinical implementations. Semin Immunopathol 2011;33:419 –440. 3. Record M, Subra C, Silvente-Poirot S, Poirot M. Exosomes as intercellular signalosomes and pharmacological effectors. Biochem Pharmacol 2011;81:1171 –1182. 4. Valadi H, Ekström K, Bossios A, Sjöstrand M, Lee JJ, Lötvall JO. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol 2007;9:654 –659. 5. Crescitelli R, Lässer C, Szabó TG, Kittel A, Eldh M, Dianzani I et al. Distinct RNA profiles in subpopulations of extracellular vesicles: apoptotic bodies, microvesicles and exosomes. J Extracellular Vesicles 2013;2:20677. 6. Witwer KW, Buzás EI, Bemis LT, Bora A, Lässer C, Lötvall J et al. Standardization of sample collection, isolation and analysis methods in extracellular vesicle research. Journal of Extracellular Vesicles 2013;2:1 –25. 7. Théry C, Ostrowski M, Segura E. Membrane vesicles as conveyors of immune responses. Nat Rev Immunol 2009;9:581 –593. 8. Silverman JM, Reiner NE. Exosomes and other microvesicles in infection biology: organelles with unanticipated phenotypes. Cell Microbiol 2011;13:1 –9. 9. György B, Szabó TG, Pásztói M, Pál Z, Misják P, Aradi B et al. Membrane vesicles, current state-of-the-art: emerging role of extracellular vesicles. Cell Mol Life Sci 2011;68: 2667 –2688. 10. Oerlemans MIFJ, Koudstaal S, Chamuleau SA, Kleijn DP, de, Doevendans PA, Sluijter JPG. Targeting cell death in the reperfused heart: Pharmacological approaches for cardioprotection. Int J Cardiol 2012;165:410 –422. 11. Coleman ML, Sahai EA, Yeo M, Bosch M, Dewar A, Olson MF. Membrane blebbing during apoptosis results from caspase-mediated activation of ROCK I. Nat Cell Biol 2001;3:339 –345. 12. Orlando KA, Stone NL, Pittman RN. Rho kinase regulates fragmentation and phagocytosis of apoptotic cells. Exp Cell Res 2006;312:5 –15. 13. Wickman GR, Julian L, Mardilovich K, Schumacher S, Munro J, Rath N et al. Blebs produced by actin-myosin contraction during apoptosis release damage-associated molecular pattern proteins before secondary necrosis occurs. Cell Death Differ 2013;20: 1293 –1305. 14. Holme PA, Orvim U, Hamers MJ, Solum NO, Brosstad FR, Barstad RM et al. Shearinduced platelet activation and platelet microparticle formation at blood flow conditions as in arteries with a severe stenosis. Arterioscler Thromb Vasc Biol 1997;17: 646 –653. 309 15. Daleke DL. Regulation of transbilayer plasma membrane phospholipid asymmetry. J Lipid Res 2003;44:233 –242. 16. Fox JE, Austin CD, Reynolds CC, Steffen PK. Evidence that agonist-induced activation of calpain causes the shedding of procoagulant-containing microvesicles from the membrane of aggregating platelets. J Biol Chem 1991;266:13289 –13295. 17. Dean WL, Lee MJ, Cummins TD, Schultz DJ, Powell DW. Proteomic and functional characterisation of platelet microparticle size classes. Thromb Haemost 2009;102: 711– 718. 18. Hunter MP, Ismail N, Zhang X, Aguda BD, Lee EJ, Yu L et al. Detection of microRNA expression in human peripheral blood microvesicles. PLoS One 2008;3:e3694. 19. Anitei M, Wassmer T, Stange C, Hoflack B. Bidirectional transport between the transGolgi network and the endosomal system. Mol Membr Biol 2010;27:443 – 456. 20. Harding C, Heuser J, Stahl P. Receptor-mediated endocytosis of transferrin and recycling of the transferrin receptor in rat reticulocytes. J Cell Biol 1983;97:329 –339. 21. Raposo G, Nijman HW, Stoorvogel W, Liejendekker R, Harding CV, Melief CJ et al. B lymphocytes secrete antigen-presenting vesicles. J Exp Med 1996;183:1161 – 1172. 22. Yu S, Liu C, Su K, Wang J, Liu Y, Zhang L et al. Tumor exosomes inhibit differentiation of bone marrow dendritic cells. J Immunol 2007;178:6867 – 6875. 23. Luketic L, Delanghe J, Sobol PT, Yang P, Frotten E, Mossman KL et al. Antigen presentation by exosomes released from peptide-pulsed dendritic cells is not suppressed by the presence of active CTL. J Immunol 2007;179:5024 –5032. 24. Caby M-P, Lankar D, Vincendeau-Scherrer C, Raposo G, Bonnerot C. Exosomal-like vesicles are present in human blood plasma. Int Immunol 2005;17:879–887. 25. Ostrowski M, Carmo NB, Krumeich S, Fanget I, Raposo G, Savina A et al. Rab27a and Rab27b control different steps of the exosome secretion pathway. Nat Cell Biol 2010; 12:19–30. Sup. pp 1– 13. 26. Mathivanan S, Simpson RJ. ExoCarta: a compendium of exosomal proteins and RNA. Proteomics 2009;9:4997 –5000. 27. Pegtel DM, Cosmopoulos K, Thorley-Lawson DA, Eijndhoven MAJ, van, Hopmans ES, Lindenberg JL et al. Functional delivery of viral miRNAs via exosomes. Proc Natl Acad Sci USA 2010;107:6328 –6333. 28. Baietti MF, Zhang Z, Mortier E, Melchior A, Degeest G, Geeraerts A et al. Syndecan-syntenin-ALIX regulates the biogenesis of exosomes. Nat Cell Biol 2012;14: 677– 685. 29. Trajkovic K, Hsu C, Chiantia S, Rajendran L, Wenzel D, Wieland F et al. Ceramide triggers budding of exosome vesicles into multivesicular endosomes. Science 2008;319: 1244–1247. 30. Gassart A, de, Geminard C, Fevrier B, Raposo G, Vidal M. Lipid raft-associated protein sorting in exosomes. Blood 2003;102:4336 – 4344. 31. Wubbolts R, Leckie RS, Veenhuizen PTM, Schwarzmann G, Möbius W, Hoernschemeyer J et al. Proteomic and biochemical analyses of human B cell-derived exosomes. Potential implications for their function and multivesicular body formation. J Biol Chem 2003;278:10963– 10972. 32. Hsu C, Morohashi Y, Yoshimura S-I, Manrique-Hoyos N, Jung S, Lauterbach MA et al. Regulation of exosome secretion by Rab35 and its GTPase-activating proteins TBC1D10A-C. J Cell Biol 2010;189:223–232. 33. Ponnambalam S, Baldwin SA. Constitutive protein secretion from the trans-Golgi network to the plasma membrane. Mol Membr Biol 2003;20:129 –139. 34. Savina A, Furlán M, Vidal M, Colombo MI. Exosome release is regulated by a calciumdependent mechanism in K562 cells. J Biol Chem 2003;278:20083 –20090. 35. Emmanouilidou E, Melachroinou K, Roumeliotis T, Garbis SD, Ntzouni M, Margaritis LH et al. Cell-produced alpha-synuclein is secreted in a calcium-dependent manner by exosomes and impacts neuronal survival. J Neurosci 2010;30:6838 –6851. 36. Yu X, Harris SL, Levine AJ. The regulation of exosome secretion: a novel function of the p53 protein. Cancer Res 2006;66:4795 –4801. 37. Lespagnol A, Duflaut D, Beekman C, Blanc L, Fiucci G, Marine J-C et al. Exosome secretion, including the DNA damage-induced p53-dependent secretory pathway, is severely compromised in TSAP6/Steap3-null mice. Cell Death Differ 2008;15:1723 –1733. 38. Qu Y, Dubyak GR. P2X7 receptors regulate multiple types of membrane trafficking responses and non-classical secretion pathways. Purinergic Signal 2009;5:163 –173. 39. Théry C, Regnault A, Garin J, Wolfers J, Zitvogel L, Ricciardi-Castagnoli P et al. Molecular characterization of dendritic cell-derived exosomes. Selective accumulation of the heat shock protein hsc73. J Cell Biol 1999;147:599 – 610. 40. Gupta S, Knowlton AA. HSP60 trafficking in adult cardiac myocytes: role of the exosomal pathway. Am J Physiol Heart Circul Physiol 2007;292:H3052 –6. 41. Vessey DA, Li L, Kelley M. P2X7 receptor agonists pre- and postcondition the heart against ischemia-reperfusion injury by opening pannexin-1/P2X? channels. Am J Physiol Heart Circul Physiol 2011;301:H881–H887. 42. Hill LM, Gavala ML, Lenertz LY, Bertics PJ. Extracellular ATP may contribute to tissue repair by rapidly stimulating purinergic receptor X7-dependent vascular endothelial growth factor release from primary human monocytes. J Immunol 2010;185: 3028–3034. 43. Banerjee I, Fuseler JW, Price RL, Borg TK, Baudino TA. Determination of cell types and numbers during cardiac development in the neonatal and adult rat and mouse. Am J Physiol Heart Circul Physiol 2007;293:H1883 –H1891. 44. Molkentin JD, Dorn GW. Cytoplasmic signaling pathways that regulate cardiac hypertrophy. Annu Rev Physiol 2001;63:391 –426. 310 45. Lopez JJ, Laham RJ, Carrozza JP, Tofukuji M, Sellke FW, Bunting S et al. Hemodynamic effects of intracoronary VEGF delivery: evidence of tachyphylaxis and NO dependence of response. Am J Physiol 1997;273:H1317 –H1323. 46. Tian Y, Morrisey EE. Importance of myocyte-nonmyocyte interactions in cardiac development and disease. Circul Res 2012;110:1023 –1034. 47. Korkut C, Ataman B, Ramachandran P, Ashley J, Barria R, Gherbesi N et al. Transsynaptic transmission of vesicular Wnt signals through Evi/Wntless. Cell 2009;139: 393 –404. 48. Claycomb WC, Lanson NA, Stallworth BS, Egeland DB, Delcarpio JB, Bahinski A et al. HL-1 cells: a cardiac muscle cell line that contracts and retains phenotypic characteristics of the adult cardiomyocyte. Proc Natl Acad Sci USA 1998;95:2979 –2984. 49. Waldenström A, Gennebäck N, Hellman U, Ronquist G. Cardiomyocyte microvesicles contain DNA/RNA and convey biological messages to target cells. PLoS One 2012;7: e34653. 50. Henderson B, Pockley AG. Proteotoxic stress and circulating cell stress proteins in the cardiovascular diseases. Cell Stress Chaperones 2012;17:303 –311. 51. Ohashi K, Burkart V, Flohé S, Kolb H. Cutting edge: heat shock protein 60 is a putative endogenous ligand of the toll-like receptor-4 complex. J Immunol 2000;164:558 –561. 52. Malik ZA, Kott KS, Poe AJ, Kuo T, Chen L, Ferrara KW et al. Cardiac myocyte exosomes: stability, HSP60 and proteomics. Am J Physiol Heart Circul Physiol 2013;304:H954–H965. 53. Tracey KJ, Cerami A. Tumor necrosis factor, other cytokines and disease. Annu Rev Cell Biol 1993;9:317 –343. 54. Yu X, Deng L, Wang D, Li N, Chen X, Cheng X et al. Mechanism of TNF-a autocrine effects in hypoxic cardiomyocytes: initiated by hypoxia inducible factor 1a, presented by exosomes. J Mol Cell Cardiol 2012;53:848–857. 55. Zhang J, Hawari FI, Shamburek RD, Adamik B, Kaler M, Islam A et al. Circulating TNFR1 exosome-like vesicles partition with the LDL fraction of human plasma. Biochem Biophys Res Commun 2008;366:579 –584. 56. Gennebäck N, Hellman U, Malm L, Larsson G, Ronquist G, Waldenström A et al. Growth factor stimulation of cardiomyocytes induces changes in the transcriptional contents of secreted exosomes. J Extracellular Vesicles 2013;2:20167. 57. Zeisberg EM, Tarnavski O, Zeisberg M, Dorfman AL, Mcmullen JR, Gustafsson E et al. Endothelial-to-mesenchymal transition contributes to cardiac fibrosis. Nat Med 2007; 13:952 –961. 58. Zhang P, Su J, Mende U. Cross talk between cardiac myocytes and fibroblasts: from multiscale investigative approaches to mechanisms and functional consequences. Am J Physiol Heart Circul Physiol 2012;303:H1385 –H1396. 59. LaFramboise WA, Scalise D, Stoodley P, Graner SR, Guthrie RD, Magovern JA et al. Cardiac fibroblasts influence cardiomyocyte phenotype in vitro. Am J Physiol Cell Physiol 2007;292:C1799–C1808. 60. Pedrotty DM, Klinger RY, Kirkton RD, Bursac N. Cardiac fibroblast paracrine factors alter impulse conduction and ion channel expression of neonatal rat cardiomyocytes. Cardiovasc Res 2009;83:688 –697. 61. Chen MM, Lam A, Abraham JA, Schreiner GF, Joly AH. CTGF expression is induced by TGF- beta in cardiac fibroblasts and cardiac myocytes: a potential role in heart fibrosis. J Mol Cell Cardiol 2000;32:1805 –1819. 62. Lee S-W, Won J-Y, Kim WJ, Lee J, Kim K-H, Youn S-W et al. Snail as a potential target molecule in cardiac fibrosis: paracrine action of endothelial cells on fibroblasts through snail and CTGF axis. Mol Therapy 2013;21:1767 –1777. 63. Webber J, Steadman R, Mason MD, Tabi Z, Clayton A. Cancer exosomes trigger fibroblast to myofibroblast differentiation. Cancer Res 2010;70:9621 – 9630. 64. Iwano M, Plieth D, Danoff TM, Xue C, Okada H, Neilson EG. Evidence that fibroblasts derive from epithelium during tissue fibrosis. J Clin Investig 2002;110:341 – 350. 65. Borges FT, Melo SA, Özdemir BC, Kato N, Revuelta I, Miller CA et al. TGF-b1-containing exosomes from injured epithelial cells activate fibroblasts to initiate tissue regenerative responses and fibrosis. J Am Soc Nephrol 2013;24:385 –392. 66. Hoefer IE, Piek JJ, Pasterkamp G. Pharmaceutical interventions to influence arteriogenesis: new concepts to treat ischemic heart disease. Curr Med Chem 2006;13:979 –987. 67. Sluijter JPG. MicroRNAs in cardiovascular regenerative medicine: directing tissue repair and cellular differentiation. ISRN Vasc Med 2013;2013:1 –16. 68. Zhou J, Li Y-S, Nguyen P, Wang K-C, Weiss A, Kuo Y-C et al. Regulation of vascular smooth muscle cell turnover by endothelial cell-secreted microRNA-126: role of shear stress. Circul Res 2013;113:40 –51. 69. Zernecke A, Bidzhekov K, Noels H, Shagdarsuren E, Denecke B, Hristov M et al. Delivery of microRNA-126 by apoptotic bodies induces CXCL12-dependent vascular protection. Sci Signal 2009;2:ra81. 70. Jong OG, de, Verhaar MC, Chen Y, Vader P, Gremmels H, Posthuma G et al. Cellular stress conditions are reflected in the protein and RNA content of endothelial cellderived exosomes. J Extracellular Vesicles 2012;1:18396. 71. Hergenreider E, Heydt S, Tréguer K, Boettger T, Horrevoets AJG, Zeiher AM et al. Atheroprotective communication between endothelial cells and smooth muscle cells through miRNAs. Nat Cell Biol 2012;14:249 –256. 72. Ludwig A-K, Giebel B. Exosomes: small vesicles participating in intercellular communication. Int J Biochem Cell Biol 2012;44:11– 15. 73. Yu X, Huang C, Song B, Xiao Y, Fang M, Feng J et al. CD4(+)CD25(+) regulatory T cells-derived exosomes prolonged kidney allograft survival in a rat model. Cellular Immunol 2013;285:62–68. J.P.G. Sluijter et al. 74. Zhang H-G, Grizzle WE. Exosomes and cancer: a newly described pathway of immune suppression. Clin Cancer Res 2011;17:959 –964. 75. Li X, Li J-J, Yang J-Y, Wang D-S, Zhao W, Song W-J et al. Tolerance induction by exosomes from immature dendritic cells and rapamycin in a mouse cardiac allograft model. PLoS One 2012;7:e44045. 76. Pêche H, Renaudin K, Beriou G, Merieau E, Amigorena S, Cuturi MC. Induction of tolerance by exosomes and short-term immunosuppression in a fully MHC-mismatched rat cardiac allograft model. Am J Transplant 2006;6:1541 –1550. 77. Akker F, van den, Deddens JC, Doevendans PA, Sluijter JPG. Cardiac stem cell therapy to modulate inflammation upon myocardial infarction. Biochim Biophys Acta 2013;1830: 2449–2458. 78. Ismail N, Wang Y, Dakhlallah D, Moldovan L, Agarwal K, Batte K et al. Macrophage microvesicles induce macrophage differentiation and miR-223 transfer. Blood 2013; 121:984 –995. 79. Pant S, Hilton H, Burczynski ME. The multifaceted exosome: biogenesis, role in normal and aberrant cellular function, and frontiers for pharmacological and biomarker opportunities. Biochem Pharmacol 2012;83:1484 –1494. 80. Fang DY, King HW, Li JY, Gleadle JM. Exosomes and the kidney: blaming the messenger. Nephrology 2013;18:1– 10. 81. Bala M, Gazalla SA, Faroja M, Bloom AI, Zamir G, Rivkind AI et al. Complications of high grade liver injuries: management and outcomewith focus on bile leaks. Scand J Trauma Resusc Emerg Med 2012;20:20. 82. Müller G. Microvesicles/exosomes as potential novel biomarkers of metabolic diseases. DiabetesMetabolic Syndr Obesity 2012;5:247–282. 83. Kanhai DA, Visseren FLJ, Graaf Y, van der, Schoneveld AH, Catanzariti LM, Timmers L et al. Microvesicle protein levels are associated with increased risk for future vascular events and mortality in patients with clinically manifest vascular disease. Int J Cardiol 2013;168:2358 –2363. 84. Jeanneteau J, Hibert P, Martinez MC, Tual-Chalot S, Tamareille S, Furber A et al. Microparticle release in remote ischemic conditioning mechanism. Am J Physiol Heart Circul Physiol 2012;303:H871 – H877. 85. Jung C, Sörensson P, Saleh N, Arheden H, Rydén L, Pernow J. Circulating endothelial and platelet derived microparticles reflect the size of myocardium at risk in patients with ST-elevation myocardial infarction. Atherosclerosis 2012;221:226 –231. 86. Hoog VC, de, Timmers L, Schoneveld AH, Wang J-W, Weg SM, van de, Sze SK et al. Serum extracellular vesicle protein levels are associated with acute coronary syndrome. Eur Heart J Acute Cardiovasc Care 2013;2:53 –60. 87. Stengaard C, Sørensen JT, Ladefoged SA, Christensen EF, Lassen JF, Bøtker HE et al. Quantitative point-of-care troponin T measurement for diagnosis and prognosis in patients with a suspected acute myocardial infarction. Am J Cardiol 2013;112: 1361–1366. 88. Moussa ID, Klein LW, Shah B, Mehran R, Mack MJ, Brilakis ES et al. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J Am Coll Cardiol 2013;62:1563 –1570. 89. Oerlemans MIFJ, Mosterd A, Dekker MS, Vrey EA, de, Mil A,, van Pasterkamp G et al. Early assessment of acute coronary syndromes in the emergency department: the potential diagnostic value of circulating microRNAs. EMBO Mol Med 2012;4: 1176 – 1185. 90. Deddens JC, Colijn JM, Oerlemans MIFJ, Pasterkamp G, Chamuleau SA, Doevendans PA et al. Circulating MicroRNAs as novel biomarkers for the early diagnosis of acute coronary syndrome. J Cardiovasc Transl Res 2013;6:884 –898. 91. Finn NA, Eapen D, Manocha P, Kassem H, Al Lassegue B, Ghasemzadeh N et al. Coronary heart disease alters intercellular communication by modifying microparticlemediated microRNA transport. FEBS Lett 2013;587:3456 –3463. 92. Vrijsen KR, Noort WA, Chamuleau SAJ, Doevendans PA, Sluijter JPG. Stem cell therapy for end-stage heart failure: indispensable role for the cell? Curr Opin Organ Transplant 2009;14:560–565. 93. Abdel-Latif A, Bolli R, Tleyjeh IM, Montori VM, Perin EC, Hornung CA et al. Adult bone marrow-derived cells for cardiac repair: a systematic review and meta-analysis. Arch Int Med 2007;167:989 – 997. 94. Jeevanantham V, Butler M, Saad A, Abdel-Latif A, Zuba-Surma EK, Dawn B. Adult bone marrow cell therapy improves survival and induces long-term improvement in cardiac parameters: a systematic review and meta-analysis. Circulation 2012;126: 551– 568. 95. Goumans M-J, Boer TP, de Smits AM, Laake LW, van Vliet P, van Metz CHG et al. TGF-beta1 induces efficient differentiation of human cardiomyocyte progenitor cells into functional cardiomyocytes in vitro. Stem Cell Res 2007;1:138–149. 96. Smits AM, Laake LW, Van Ouden K, Den Schreurs C, Echteld CJ, Van Mummery CL et al. Human cardiomyocyte progenitor cell transplantation preserves long-term function of the infarcted mouse myocardium. Cardiovasc Res 2009;83:527 –535. 97. Gnecchi M, Zhang Z, Ni A, Dzau VJ. Paracrine mechanisms in adult stem cell signaling and therapy. Circul Res 2008;103:1204 –1219. 98. Tang X-L, Rokosh G, Sanganalmath SK, Yuan F, Sato H, Mu J et al. Intracoronary administration of cardiac progenitor cells alleviates left ventricular dysfunction in rats with a 30-day-old infarction. Circulation 2010;121:293 –305. Vesicles for intracardiac communication 99. Gnecchi M, He H, Liang OD, Melo LG, Morello F, Mu H et al. Paracrine action accounts for marked protection of ischemic heart by Akt-modified mesenchymal stem cells. Nat Med 2005;11:367 –368. 100. Timmers L, Lim SK, Arslan F, Armstrong JS, Hoefer IE, Doevendans PA et al. Reduction of myocardial infarct size by human mesenchymal stem cell conditioned medium. Stem Cell Res 2007;1:129 –137. 101. Lai RC, Arslan F, Lee MM, Sze NSK, Choo A, Chen TS et al. Exosome secreted by MSC reduces myocardial ischemia/reperfusion injury. Stem Cell Res 2010;4:214 –222. 102. Arslan F, Lai RC, Smeets MB, Akeroyd L, Choo A, Aguor ENE et al. Mesenchymal stem cell-derived exosomes increase ATP levels, decrease oxidative stress and activate PI3K/ Akt pathway to enhance myocardial viability and prevent adverse remodeling after myocardial ischemia/reperfusion injury. Stem Cell Res 2013;10:301–312. 103. Lichtenauer M, Mildner M, Hoetzenecker K, Zimmermann M, Podesser BK, Sipos W et al. Secretome of apoptotic peripheral blood cells (APOSEC) confers cytoprotection to cardiomyocytes and inhibits tissue remodelling after acute myocardial infarction: a preclinical study. Basic Res Cardiol 2011;106:1283 –1297. 104. Smits AM, Vliet P, van Metz CH, Korfage T, Sluijter JP, Doevendans PA et al. Human cardiomyocyte progenitor cells differentiate into functional mature cardiomyocytes: an in vitro model for studying human cardiac physiology and pathophysiology. Nat Protoc 2009;4:232 –243. 311 105. Vrijsen KR, Sluijter JPG, Schuchardt MWL, Balkom BWM, Van Noort WA, Chamuleau SAJ et al. Cardiomyocyte progenitor cell-derived exosomes stimulate migration of endothelial cells. J Cell Mol Med 2010;14:1064 –1070. 106. Chen L, Wang Y, Pan Y, Zhang L, Shen C, Qin G et al. Cardiac progenitor-derived exosomes protect ischemic myocardium from acute ischemia/reperfusion injury. Biochem Biophys Res Commun 2013;431:566–571. 107. Barile L, Gherghiceanu M, Popescu LM, Moccetti T, Vassalli G. Ultrastructural evidence of exosome secretion by progenitor cells in adult mouse myocardium and adult human cardiospheres. J Biomed Biotechnol 2012;2012:354605. 108. Gherghiceanu M, Popescu LM. Cardiac telocytes - their junctions and functional implications. Cell Tissue Res 2012;348:265–279. 109. Sahoo S, Klychko E, Thorne T, Misener S, Schultz KM, Millay M et al. Exosomes from human CD34(+) stem cells mediate their proangiogenic paracrine activity. Circul Res 2011;109:724–728. 110. Mackie AR, Klyachko E, Thorne T, Schultz KM, Millay M, Ito A et al. Sonic hedgehogmodified human CD34+ cells preserve cardiac function after acute myocardial infarction. Circul Res 2012;111:312–321. 111. Pola R, Ling LE, Silver M, Corbley MJ, Kearney M, Blake Pepinsky R et al. The morphogen Sonic hedgehog is an indirect angiogenic agent up-regulating two families of angiogenic growth factors. Nat Med 2001;7:706–711.