Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gene therapy wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
Human–animal hybrid wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Genetic drift wikipedia , lookup
Oncogenomics wikipedia , lookup
Frameshift mutation wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Genetic testing wikipedia , lookup
Population genetics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Human genetic variation wikipedia , lookup
Point mutation wikipedia , lookup
Medical genetics wikipedia , lookup
History of genetic engineering wikipedia , lookup
Public health genomics wikipedia , lookup
Genetic engineering wikipedia , lookup
Genome (book) wikipedia , lookup
Microevolution wikipedia , lookup
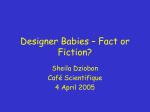
Diagnosis of genetic disease in preimplantation embryos Preimplantation genetic diagnosis today Alan H.Handyside Institute of Obstetrics and Gynaecology, Royal Postgraduate Medical School, Hammersmith Hospital, Du Cane Road, London W12 ONN, UK Introduction The use of assisted reproduction techniques allows preimplantation genetic diagnosis of an inherited disease in early human embryos before fertilization. Some genetic defects have even been identified before fertilization by analysis of the first polar body of the oocyte (Verlinsky et al., 1990, 1992). By selective transfer of only unaffected embryos, couples at risk of having affected children can avoid the possibility of terminating an affected pregnancy following more conventional diagnostic approaches later in gestation. Clinical experience is still limited but worldwide approaching 200 hundred cycles have now been reported resulting in 50 pregnancies and over 30 births (Table I) (Harper, 1996). Collecting and biopsying human embryos Attempts to flush embryos from the uterus following superovulation and conception in vivo have so far failed. In any case, there would always be a risk that a potentially affected embryo remained in the uterus. Clinical application of preimplantation genetic diagnosis has therefore exclusively used the methods of superovulation and in-vitro fertilization (IVF) established for the treatment of infertile couples. This produces a number of normally fertilized embryos in a single cycle accessible for genetic screening. Most couples are known to be fertile since the previous birth of an affected child is often the reason they are aware of the risk in future pregnancies. Nevertheless, the use of established ovarian stimulation protocols following down-regulation with gonadotrophinreleasing hormone (GnRH) analogues is appropriate because the probability of an embryo being affected is high in many cases. Maximizing the number of embryos screened increases the likelihood of establishing a pregnancy. Human embryos have been successfully biopsied at cleavage stages on day 3 post-insemination, at the 6-l0-cell stage, and at the blastocyst stage on days 5 or 6 (Dokras et al., 1990, 1991; Muggleton Harris et al., 1995; Pickering and Human Reproduction Volume 11 Supplement 1 1996 © European Society for Human Reproduction and Embryology 139 A.H.Handyside Table I. Summary of world clinical experience with preimplantation genetic diagnosis following in-vitro fertilization (IVF) and cleavage stage biopsy to February, 1995" Patients Cycles Transfers Pregnancies Babies X-linked (PCR) 41 62 53 14 II X-linked (FISH) 49 70 56 15 II Single gene defects Total 59 65 62 21 12 149 197 171 50 34 PCR = polymerase chain raction; FISH = fluorescence in-situ hybridization. Pregnancy rate = 25% per cycle, 29% per embryo transfer. Results collated from 14 centres. "Modified from Harper, (1996). Muggleton Harris, 1995). Blastocyst biopsy has the advantage that a larger number of cells can be removed from the outer trophectoderm layer without affecting the inner cell mass from which the fetus later develops. However, too few embryos reach this stage and implant after transfer to be clinically viable for preimplantation genetic diagnosis at the present time. Removal of one or two cells at the equivalent of the 8-cell stage does not appear to affect development to the blastocyst stage in vitro (Hardy et aI., 1990) and has proved to be highly efficient in practice (Ao and Handyside, 1995). The procedure involves dissolving a hole in the zona pellucida using acidified Tyrode's solution (Figure 1) and then aspirating the cells with a second larger micropipette. Also, co-culture of the isolated cells with the biopsied embryo supports limited proliferation and may provide an alternative to the more difficult procedure of blastocyst biopsy (Geber et al., 1995). So far there have been no reports of serious abnormalities at birth following cleavage stage biopsy. Human embryos, like other mammalian embryos, appear to be able to regulate their development at these early stages presumably because cells are not yet irreversibly committed to specific fates. Genetic analysis The genetic analysis of single cells has been made possible by the development of DNA amplification methods involving the polymerase chain reaction (PCR) and fluorescence in-situ hybridization (FISH) for rapid cytogenetic analysis of interphase nuclei. Single cells biopsied at cleavage stages are therefore prepared for analysis either by carefully placing the cells in lysis buffer in micro centrifuge tubes for PCR or by spreading the nucleus on a microscope slide for FISH. Single cell analysis by peR To amplify sufficient DNA from a single cell for analysis by conventional gel electrophoresis, two rounds of amplification are necessary. 'Nesting' the second 140 Preimplantation genetic diagnosis Figure 1. Scanning electron micrograph of a human cleavage stage embryo following zona drilling with Acid Tyrodes and biopsy to remove one of the blastomeres. Note the apparently double layered appearance of the zona and the extensive thinning of the outer layer. (Courtesy of Dr George Nikas). pair of oligonucleotide primers, which define the region to be amplified, internally to the first pair has several advantages and provides a safeguard for product contamination carried over into the sample tubes (Figure 2). Theoretically, only a single molecule could be amplified and give an erroneous result. Following amplification, many approaches have been used to identify the presence of different mutations (Table II). Since the aim is to transfer selected embryos on the same day as the biopsy to maximise pregnancy rates, amplification and mutation detection have to be completed in 8-12 h. Pregnancies and births confirmed to be free of the inherited disease have been established in couples at risk of several common single gene defects including cystic fibrosis (CF) (Handyside et aI., 1992), Duchenne muscular dystrophy (DMD) (Liu et aI., 1995) and Tay Sachs disease (Gibbons et aI., 1995). Preimplantation genetic diagnosis has also been achieved for a specific mutation causing the rare X-linked condition, Lesch-Nyhan syndrome (E. Hughes, P.P. Ray, R.M. Winston and A.H. Handyside, unpublished). With CF and Tay Sachs, the common three base pair (bp) deletion and 4 bp insertion respectively, were detected by heteroduplex formation (Figure 3). A 3 or 4 bp size difference in the amplified fragment cannot be reliably discriminated by rapid gel electrophoresis. By mixing the amplified DNA from the single cell with DNA previously 141 A.H.Handyside 01 ____ _ __'____Sl.¥.._ _ _ __ ----- ------2S----~-- 1 -20 cycles 102 11~ ~ 12 130 cycles 1 Figure 2. Diagrammatic representation of polymerase chain reaction (peR) using nested oligonucleotide primers. In the first amplification reaction, an outer pair of primers (0 I and 02) annealing to the sense and antisense strands of the genomic target sequence encompassing the mutation (tIiangles) is pm1ially amplified. In the second reaction, a second set of 'nested' pIimers (II and 12) annealing to the target sequence internal to that of the outer primers is used to amplify a smaller fragment from an aliquot of the first amplified product. Two rounds of amplification is necessary in most cases to amplify sufficient DNA from single cells for conventional analysis. The use of nested primers reduces non-specific amplification. It is also a safeguard to prevent carry-over contamination of samples tubes with the final amplification product since the outer primers should not anneal to this sequence. Table II. Some methods for detecting mutations in amplified fragments for preimplantation genetic diagnosis Method Typical application Fragment length differences Distinguishing gene and intronless pseudogene sequences Analysis of variable number tandem repeats Heteroduplex formation Rapid detection of small insertions or deletions Restriction digestion Detection of mutations that eliminate restriction sites Allele specific oligonucleotides (ASOs) Hybridization of normal and mutant ASOs detected by nonradioactive methods Single strand conformation polymorphism (SSCP) Detection of majority of mutations anywhere within the amplified fragment Oligonucleotide ligation Direct detection of point mutations Microsequencing Mutation detection by incorporation of radio labelled nucleotides-avoids gel electrophoresis amplified from homozygous normal or affected individuals, denaturing the double stranded DNA fragments and allowing the mixtures to cool slowly, heteroduplexes are formed in those cases where both normal length fragments and mutated longer or shorter fragments are present. When these mixtures are electrophoresed, 142 Preimplantation genetic diagnosis CellI ~ + NN AA + Cell 2 ~ + NN Cell 3 ~ + + + AA NN AA Cell 4 ~ + NN + AA -- -------NN NA Amp failure Figure 3. Diagrammatic representation of the use of heteroduplex formation for the rapid detection of, in this example, the common 3 base pair (bp) deletion, L'1F508, causing cystic fibrosis, Amplified product from each of four single cells is mixed with amplified product from either known homozygous normal (NN) or affected (L'1L'1) individuals. The pattern of heteroduplex bands obtained with the two mixtures allows all three possible genotypes as well as amplification failure to be identified on a small polyacrylamide gel run for as little as 30 min. the heteroduplexes are significantly retarded on the gel and can be reliably interpreted for diagnosing the genotype of the cell biopsied from the embryo. Single cell analysis by FISH Pioneering studies of the karyotype of early human embryos following IVF demonstrated a high incidence of chromosomal abnormalities and mosaicism (Angell et aI., 1986; Plachot et aI., 1987; Jamieson et aI., 1994). The low incidence of metaphases, with or without the use of spindle inhibitors, and the difficulty of banding the short chromosomes at these stages, however, make it impractical to use this approach for diagnostic purposes and prevents analysis of all nuclei. FISH is equally applicable to both interphase and metaphase nuclei and the use of multicolour probes allows the detection of more than one probe simultaneously. Dual FISH with X and Y specific probes have been used clinically for identifying the sex of embryos in couples at risk of X-linked diseases which only affect boys (Griffin et al., 1992, 1993, 1994). This approach has now been further refined using directly labelled probes and an additional autosomal probe to distinguish sex chromosome aneuploidy from abnormal ploidy. Combined with a new spreading procedure involving dissolving the cytoplasm of the single cells and attaching the nuclei to poly-L-lysine-coated slides, it is now possible to complete the analysis within 2 h (Harper et aI., 1994). In addition to identifying sex in X-linked disease, FISH analysis is being used for detecting trisomies in couples in which one partner is carrying a reciprocal or Robertsonian translocation. These couples are often at high risk of trisomic pregnancies and many have repeated miscarriages. These couples are good candidates for preimplantation genetic diagnosis since several embryos can be screened in a single cycle. The usual probes specific for repeated sequences in 143 A.H.Handyside the centromeric region of particular chromosomes may not be suitable and more distal unique sequence yeast artificial chromosome (YAC) or cosmid contig probes are being developed. Combinations of probes, specific for the same chromosome, can also be used for accurate detection of particular trisomies, for example, in women believed to be gonadal mosaics (c. Conn, J. Harper and J.D.A. Delhanty, personal communication). Analysis of spare human embryos or those rejected for transfer following FISH analysis of the sex chromosomes has confirmed the relatively high incidence of aneuploidy (-25%) at conception (Munne et al., 1993). There also appears to be an unexpectedly marked increase with maternal age. In some studies this increased to almost 50% above the age of 40 (Munne et al., 1995). As the majority of aneuploidies arise during maternal meiosis especially meiosis I, first and/or second polar body analysis with combinations of probes detecting X, Y, 21, 18 and 13 are being used to screen embryos in older women undergoing IVF (Verlinsky et al., 1995). If sufficient euploid embryos can be identified this may improve pregnancy rates and decrease miscarriage rates in these women. Analysis of all nuclei in individual embryos at cleavage stages has confirmed that many embryos are chromosomally mosaic. In addition to aneuploidies arising during gametogenesis and abnormalities arising at fertilization, it is clear that there is also a high incidence of postzygotic abnormalities (Delhanty et al., 1996). Most of the nuclei involved, however, have an abnormal ploidy. For example, tetraploid nuclei are relatively common although haploid and triploid nuclei have also been detected. The origin of these cells is not known but it is possible that in some cases it results from delayed fertilization or pronucleus formation by supernumerary spermatozoa for example. Non-disjunction in early cleavage has been observed but is relatively uncommon. Finally, some embryos have apparently chaotic chromosomal complements in almost every nucleus and this appears to be associated with particular patients as it is consistently observed in successive cycles of IVE Human embryos like those of lower vertebrates and invertebrates, therefore, may lack the normal cell cycle checkpoints and accumulate chromosomal errors during cleavage (Delhanty and Handy-side, 1995). The accuracy of preimplantation genetic diagnosis The accuracy of preimplantation genetic diagnosis remains to be assessed in clinical practice. Three misdiagnoses have already been reported (Harper and Handyside, 1994). However, these involved different diagnostic procedures and probably occurred for different reasons. All five children resulting from a recent series of 18 preimplantation genetic diagnosis cycles for the predominant ~F508 deletion causing CF were confirmed to be homozygous normal (Ao et al., 1995). However, analysis of each blastomere from the embryos which were not transferred did reveal some errors particularly in amplifying both parental alleles in heterozygous carrier cells. Often one parental allele failed to amplify, apparently randomly (allele dropout), resulting in an incorrect diagnosis as homozygous 144 Preimplantation genetic diagnosis normal or affected. Further work with single heterozygous lymphocytes has now shown that this phenomenon is partly explained by incomplete denaturation of the genomic template DNA during the initial cycles of PCR (Ray and Handyside, 1996). Raising the temperature in the initial cycles improves the efficiency of denaturation and minimizes but does not eliminate allelic dropout (Figure 4). Fortunately in an autosomal recessive condition, allele dropout cannot cause a serious misdiagnosis leading to the transfer of a homozygous affected embryo (at least in these couples in which both partners were carrying the same mutation). For compound heterozygote detection or dominant conditions, however, this could theoretically occur in half the cases of allele dropout in which the affected allele did not amplify. One way of avoiding these errors for diagnosis of compound heterozygotes is to amplify a single DNA fragment encompassing both mutations. This has recently been demonstrated for ~-thalassaemia: major diagnosis with single lymphocytes from a boy who is a compound heterozygote for two common Indian mutations of the ~-globin gene (Ray et ai., 1996). A 208 bp fragment including ex on 1 and part of intervening sequence 1 encompassing 12 of the common ~-thalassaemia mutations and also the mutation causing sickle cell disease was amplified with high efficiency from single cells (Figure 5). Allele dropout did occur in a minority of cells but in these cases the genotype appeared to be homozygous at one locus for the normal allele and at the other for the mutation. Since this is an impossible combination of parental alleles the possibility of an error is avoided (Figure 6). Clinical application of preimplantation genetic diagnosis for couples at risk of ~-thalassaemia, many of whom carry different mutations, should therefore be possible using this approach. Four general sources of errors have been identified with single blastomere analysis at cleavage stages (Table III). However, careful monitoring of FISH or amplification efficiency and contamination levels and reducing allelic dropout I <Xl 0 80 Q ..rt < ~ ~ 60 40 20 0 87 90 (n=50) 93 (n=62) 96 (n=78) Denaturation temperature Figure 4. Graph demonstrating the relationship of the incidence of total amplification failure and randum allele dropout (ADO) with varying denaturing temperatures in the first cycles of nested polymerase chain reaction (PCR) for a series of single lymphocytes heterozygous for the Ll.F5<Hi deletion. Amplification efficiency. i.e. amplification of at least one allele. is high at all temperatures (top line) whereas the incidence of ADO is significantly reduced by raising the annealing temperature to 96°C (bottom line). This suggests that ADO is caused by a combination of failure to denature the genomic target and genomic target degradation in the first cycles of PCR. 145 A.H.Handyside Table III. Sources of errors in preimplantation genetic diagnosis Potential consequences Source of errors PCR failures Amplification failure No diagnosis. Misdiagnosis of deletions Allele dropout (ADO) Misdiagnosis of carriers. Preferential amplification Misdiagnosis of carriers Non-specific amplification General misdiagnosis Carryover contamination General misdiagnosis Extraneous contamination General misdiagnosis FISH failures Hybridization failure or extraneous signals Misdiagnosis of sex with single probe. Misdiagnosis as aneuploid Nuclear abnormalities Anucleate blastomeres No diagnosis. Misdiagnosis of deletions Binucleate blastomeres Arise by failure of cytokinesis. Not known to cause errors Multinucleate blastomeres Mostly fragmenting nuclei. Misdiagnosis likely Apoptotic or degenerating nuclei General misdiagnosis Chromosomal abnormalities Haploid Misdiagnosis of carriers Triploid Depending on origin probably not a risk Tetraploid Depending on origin probably not a risk Aneuploid Only a risk if involving the chromosome with the defect Chaotic High risk of misdiagnosis ......0 - - - - - - - - - - - - - - 772bp - - - - - - - - - - - _ . , "" ... o O - - - - 2 0 8 b p - - - - I.~" . ~ 5' ~ -:-~: I If' ~ nt 1:JCnI Exon 1 J 5: IVS 1 I Exon~--,--.:..:..::..=IVS'2-;/- I pxon3 1 3' Figure 5. Diagrammatic representation of the position of the nested primers (outer primers: 01 and 02; inner primers: [3 and 14) used to amplify the first exon and part of intervening sequence [ (IVS-I) of the 0-globin gene from single cells for the preimplantation diagnosis of 0-thalassaemia. The smaller inner amplification product of 208 bp encompasses the sites of 12 common mutations including two Indian mutations at IVS-I nucleotide 1 and 5 (nt 1 and nt5). and the mutation causing sickle cell disease (0'). by manipulating amplification conditions together with analysis of two cells from each embryo where possible should minimize the risk. Estimates of the risk based on analysis of several hundred single blastomeres from the series of preimplantation genetic diagnosis cycles for the common LlF508 mutation causing CF (see above) ranged betweeri 0.1-2% depending on the genotype and whether one or two cells are analysed (PRay and A.Handyside, unpublished). At the 146 Preimplantation genetic diagnosis PARENTS POSSIBLE OFFSPRING APPARENT GENOTYPE OF COMPOUND HETEROZYGOTE '-y-J ---+ nonsense ADO Figure 6. Diagram illustrating the consequences of allelic dropout (ADO) when attempting to identify compound heterozygotes. Following amplification of a fragment encompassing both mutations from a single compound heterozygous cell, ADO results in failure to amplify an allele with one of the parental mutations. However. as the cell cannot be simultaneously homozygous for one mutation and homozygous for the normal allele at the other site, this result prevents any risk of the embryo being considered for transfer. lower end of this range this is probably acceptable though it should be possible to improve on these results and reduce the risk to closer to one in a thousand. In view of the regulative capacity of embryos at these early stages and the possibility that the fetus will be derived from only a subset of cells, however, it may never be possible to exclude errors. For most couples, considerably reducing their risk of an affected pregnancy is sufficient especially if the a priori risk is high. The future of preimplantation genetic diagnosis The development of techniques for genetic analysis of single cells has given us powerful tools to study early human embryos and understand the contribution of chromosomal and other genetic abnormalities to developmental failure at these early stages. Polar body screening and screening of blastomeres from cleavage stage embryos offer the prospect of improving selection of viable embryos for transfer which should increase implantation and pregnancy rates in infertile couples following IVF. For preimplantation genetic diagnosis in couples at risk of inherited disease, initial clinical experience and recent developments in the technology of single cell analysis, offer the prospect of accurate diagnosis of a broadening range of conditions. These developments include the use of fluorescent analysis of peR products allowing multiplex analysis of several fragments amplified in the same 147 A.H.Handyside Table IV. Genetic disorders prevalent in the UK" Recessive Haemochromatosis 1 in 500 Cystic fibrosis 1 in 2000 Sickle cell anaemia 1 in 400 Thalassaemia 1 in 400 Pheny lketonuria I in 10000 Dominant Huntington's disease I in 10 000 X-linked Duchenne muscular dystrophy I in 4000 males Complex multifactorial Cardiovascular disease > 10% lifetime risk Alzheimer's disease 10% over 65 years Breast cancer 10% familial Colorectal cancer 1 in 200 (HNPCC) I in 8000 (APC) Diabetes Type I 1 in 500 Diabetes Type II 1-7% adults Schizophrenia 1% lifetime risk Chromosomal Down's syndrome 1 in 625 "Modified from Science and Technology Committee (1995). reaction (Findlay et aI., 1995), a multiplex oligonucleotide ligation assay for 30 common CF mutations accounting for >96% of CF carriers (Eggerding et aZ., 1995), and whole genome preamplification allowing secondary amplification of several DNA sequences from single cells (Zhang et aI., 1992; Kristjansson et aI., 1994). For chn;)mosomal analysis, comparative genome hybridization (CGH) (Kallioniemi et aI., 1992) may be possible by generating a probe from single cells by whole genome amplification. This would allow karyotype analysis by hybridizing a mixture of probes from the embryo cell and a normal cell to a normal metaphase spread. Computer analysis of the relative strength of the hybridization signals then allows identification of regions over or under represented in the test sample e.g. trisomies or monsomies. Alternatively, again using computer-assisted analysis, analysis of all 23 pairs of chromosomes using chromosome specific paint probes labelled with different fiuorochromes has recently been achieved (Speicher et aI., 1996). If possible at the single cell level, 148 Preimplantation genetic diagnosis this would enable screening for any translocations as well as aneuploidy and some other structural abnormalities. Single cell genetic analysis is already possible for many of the prevalent inherited single gene defects in the UK (Table IV). Now because preimplantation genetic diagnosis does not involve terminating established pregnancies, attention is focussing on the potential for screening late onset diseases and other medical conditions which may put the mother or baby at risk. With late onset disease, individuals are often only affected after they have had children. If they know family members have been affected they may not wish to know their own carrier status but want to prevent their children inheriting the defect. One relatively common example is Huntington's chorea. In these cases, termination of an otherwise healthy fetus would be a difficult choice. Alternatively it is theoretically possible to offer preimplantation genetic diagnosis without informing the parents of their carrier status (Schulman et al., 1996). Screening for dominant single gene defects which predispose carriers to familial forms of breast and colon cancer is also being considered. In many of these cases, the penetration of the gene defect is high and affected individuals will almost certainly develop tumours in later life. In these conditions, even radical surgery may not completely eliminate the risk of other malignancies associated with the loss of tumour supressor activity. Beyond these conditions, however, screening for genetic contributions to common diseases with a significant environmental component is unlikely to be effective and raises serious ethical issues. References Angell, R.R., Templeton, AA, and Aitken, R.J. (1986) Chromosome studies in human in vitro fertilization. Hum. Genet., 72, 333-339. Ao, A and Handyside, AH. (1995) Cleavage stage human embryo biopsy. Hum. Reprod. Update, 1,3. Ao, A, Ray, P., Lesko, J et al. (1995) Clinical experience with preimplantation diagnosis oLthe ,iF508 deletion causing cystic fibrosis. Prenat. Diagn., 16, 137-142. Delhanty, J.D.A. and Handyside, AH. (1995) The origin of genetic defects in the human and their detection in the preimplantation embryo. Oxford Rev. Reprod. BioI., 17, 125-158. Delhanty, J.D.A, Harper, J.C., Ao, A et al. (1996) Multicolour FISH detects frequent chromosomal mosaicism in normal preimplantation embryos from fertile patients. Prenat. Diagn., (in press). Dokras, A, Sargent, I.L., Ross, C. et al. (1990) Trophectoderm biopsy in human blastocysts: Hum. Reprod., 5, 821-825. Dokras, A, Sargent, I.L., Gardner, R.L. and Barlow, D.H. (1991) Human trophectoderm biopsy and secretion of chorionic gonadotrophin. Hum. Reprod., 6, 1453-1459. Eggerding, F.A, Iovannisci, D.M., Brinson, E. et al. (1995) Fluorescence-based oligonucleotide ligation assay for analysis of cystic fibrosis transmembrane conductance regulator gene mutations. Hum. Mutat., 5, 153-165. Findlay, I., Urquhart, A, Quirke, P. et al. (1995) Simultaneous DNA 'fingerprinting', diagnosis of sex and single-gene defect status from single cells. Hum. Reprod., 10, 1005-1013. Geber, S., Winston, R.M., and Handyside, A.H. (1995) Proliferation of blastomeres from biopsied cleavage stage human embryos in vitro: an alternative to blastocyst biopsy for preimplantation diagnosis. Hum. Reprod., 10, 1492-1496. Gibbons, W.E., Gitlin, S.A, Lanzendorf, S.E. et al. (1995) Pre implantation genetic diagnosis of 149 A.H.Handyside Tay Sachs disease; successful pregnancy after pre-embryo biopsy and gene amplification by polymerase chain reaction. Fertil. Steril., 63,723-728. Griffin, D.K., Wilton, L.I., Handyside, A.H. et al. (1992) Dual fluorescent in situ hybridisation for simultaneous detection of X and Y chromosome-specific probes for the sexing of human preimplantation embryonic nuclei. Hum. Genet., 89, 18-22. Griffin, D.K., Wilton, L.J., Handyside, AH. et al. (1993) Diagnosis of sex in preimplantation embryos by fluorescent in situ hybridisation. Br. Med. J., 306, 1382. Griffin, D.K., Handyside, AH., Harper, J.e. et al. (1994) Clinical experience with preimplantation diagnosis of sex by dual fluorescent in situ hybridization. J. Assist. Reprod Genet., 11, 132-143. Handyside, AH., Lesko, J.G., Tarin, J.J. et al. (1992) Birth of a normal girl after in vitro fertilization and preimplantation diagnostic testing for cystic fibrosis [see comments]. N. Engl. J. Med., 327, 905-909. Hardy, K., Martin, K.L., Leese, H.I. et al. (1990) Human preimplantation development in vitro is not adversely affected by biopsy at the 8-cell stage. Hum. Reprod., 5, 708-714. Harper, J.C., Coonen, E., Ramaekers, P.e. et al. (1994) Identification of the sex of human preimplantation embryos in 2 hours using an improved spreading method and fluorescent insitu hybridization (FISH) using directly labelled probes. Hum. Reprod., 9, 721-724. Harper, J.e. and Handyside, AH. (1994) The current status of preimplantation diagnosis. Curro Obstet. Gynecol., 4, 143-149. Harper, J.e. (1996) Preimplantation diagnosis of inherited disease by embryo biopsy. An update of world figures. J. Assist. Reprod. Genet., 13, 90-95. Jamieson, M.E., Coutts, J.R.T., and Connor, J.M. (1994) The chromosome consitution of human preimplantation embryos fertilized in vitro. Hum. Reprod., 9, 709-715. Kallioniemi, A, Kallioniemi, O-P., Suder, D. et al. (1992) Comparative genomic hybridization for molecular cytogenetic analysis of solid tumours. Science, 258, 818-821. Kristjansson, K., Chong, S.S., Van den Veyver, LB. et al. (1994) Preimplantation single cell analyses of dystrophin gene deletions using whole genome amplification. Nature Genet., 6,19-23. Liu, J., Lissens, W., Van Broeckhoven, e. et al. (1995) Normal pregnancy after preimplantation DNA diagnosis of a dystrophin gene deletion. Prenat. Diagn., 15, 351-358. Muggleton Harris, AL., Glazier, AM., Pickering, S. and Wall, M. (1995) Genetic diagnosis using polymerase chain reaction and fluorescent in-situ hybridization analysis of biopsied cells from both the cleavage and blastocyst stages of individual cultured human preimplantation embryos. Hum. Reprod., 10, 183-192. Munne, S., Lee, A, Rosenwaks, Z. et al. (1993) Diagnosis of major chromosome aneuploidies in human preimplantation embryos. Hum. Reprod., 8, 2185-2191. Munne, S., Sultan, K.M., Weier, H.U. et al. (1995) Assessment of numeric abnormalities of X, Y, 18, and 16 chromosomes in preimplantation human embryos before transfer. Am. J. Obstet. Gynecol., 172, 1191-1199. Pickering, S.I. and Muggleton Harris, A.L. (1995) Reliability and accuracy of polymerase chain reaction amplification of two unique target sequences from biopsies of cleavage-stage and blastocyst-stage human embryos. Hum. Reprod., 10, 1021-1029. Plachot, M., de Grouchy, J., Junca, A-M. et al. (1987) From oocyte to embryo: a model, deduced from in vitro fertilization for natural selection against chromosome abnormalities. Ann. Genet., 30,22-32. Ray, P.P. and Handyside, AH. (1996) Increasing the temperature during the first cycles of amplification reduces allele dropout from single cells for preimplantation genetic diagnosis. Hum. Reprod., 2, 213-218. Ray, P.P., Kaeda, J.S., Bingham, J. et al. (1996) Preimplantation genetic diagnosis of ~-thalassaemia major: accurate detection of mutations in a compound heterozygote following single cell amplification. Lancet, 347, 1696. Schulman, J.D., Black, S.H., Handyside, AH. and Nance, W.E. (1996) Preimplantation genetic testing for Huntington Disease and certain other dominantly inherited disorders. Clin. Genet., in press. Science and Technology Committee (1995) Human Genetics: the Science and its Consequences. Third Report. HMSO, London. 150 Preimplantation genetic diagnosis Speicher, M.R., Gwyn Ballard, S. and Ward, D.C. (1996) Karyotyping human chromosomes by combinatorial multi-fluor FISH. Nature Genet., 12, 368-375. Verlinsky, Y., Ginsberg, N., Lifchez, A. et al. (1990) Analysis of the first polar body: preconception genetic diagnosis. Hum. Reprod., 5, 826-829. Verlinsky, Y., Rechitsky, S., Evsikov, S. et al. (1992) Preconception and preimplantation diagnosis for cystic fibrosis. Prentit. Diagn., 12, 103-110. Verlinsky, Y., Cieslak, J., Freidine, M. et al. (1995) Pregnancies following pre-conception diagnosis of common aneuploidies by fluorescent in-situ hybridization. Hum. Reprod., 10, 1923-1927. Zhang, L., Cui, X., Schmitt, K. et al. (1992) Whole genome amplification from a single cell: implications for genetic analysis. Proc. Nat!. Acad. Sci. USA, 89, 5847-5851. 151