Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
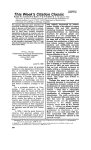
invited review Exercise regulation of glucose transport in skeletal muscle TATSUYA HAYASHI,1 JØRGEN F. P. WOJTASZEWSKI,2 AND LAURIE J. GOODYEAR1 Division, Joslin Diabetes Center, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts 02215; and 2Copenhagen Muscle Research Centre, August Krogh Institute, University of Copenhagen, DK-2100 Copenhagen, Denmark 1Research Hayashi, Tatsuya, Jørgen F. P. Wojtaszewski, and Laurie J. Goodyear. Exercise regulation of glucose transport in skeletal muscle. Am. J. Physiol. 273 (Endocrinol. Metab. 36): E1039–E1051, 1997.— Exercise increases the rate of glucose uptake into the contracting skeletal muscles. This effect of exercise is similar to the action of insulin on glucose uptake, and the mechanism through which both stimuli increase skeletal muscle glucose uptake involves the translocation of GLUT-4 glucose transporters to the plasma membrane and transverse tubules. Most studies suggest that exercise and insulin recruit distinct GLUT-4containing vesicles and/or mobilize different ‘‘pools’’ of GLUT-4 proteins originating from unique intracellular locations. There are different intracellular signaling pathways that lead to insulin- and exercisestimulated GLUT-4 translocation. Insulin utilizes a phosphatidylinositol 3-kinase-dependent mechanism, whereas the exercise signal may be initiated by calcium release from the sarcoplasmic reticulum leading to the activation of other signaling intermediaries, and there is also evidence for autocrine- or paracrine-mediated activation of transport. The period after exercise is characterized by increased sensitivity of muscle glucose uptake to insulin, which can be substantially prolonged in the face of carbohydrate deprivation. The ability of exercise to utilize insulin-independent mechanisms to increase glucose uptake in skeletal muscle has important clinical implications, especially for patients with diseases that are associated with peripheral insulin resistance, such as non-insulin-dependent diabetes mellitus. muscle contraction; glucose transporters; GLUT-4; calcium; insulin DURING PHYSICAL EXERCISE the increased requirement for metabolic substrates in the working muscles is met partially through the enhanced utilization of glucose. To meet this increased need, there is a significant elevation in the rate of glycogenolysis in the contracting muscles. In addition, exercise has an ‘‘insulin-like effect’’ to increase the uptake of glucose from the circulation into the working muscles. In the period after exercise, muscle glucose uptake is more sensitive to insulin, an effect that facilitates the resynthesis of muscle glycogen stores. Both the acute and persistent effects of exercise on glucose uptake and glycogen metabolism have important implications for individuals with insulin resistance, because these changes can effect the acute regulation of glucose homeostasis as well as chronic metabolic control. Several excellent reviews have described the effects of exercise on glucose uptake in skeletal muscle (17, 50, 95, 103, 122). The current review will discuss work from the last six to seven years that has focused on elucidating the underlying molecular mechanisms for the changes in glucose uptake that occur in skeletal muscle during and after a single bout of physical exercise. EFFECTS OF EXERCISE ON THE GLUCOSE TRANSPORT SYSTEM Under normal physiological conditions, glucose transport is the rate-limiting step in glucose utilization (69). Glucose transport occurs primarily by facilitated diffusion, an energy-independent process that uses a carrier protein for transport of a substrate across a membrane. The glucose transporter carrier proteins in mammalian tissues are a family of structurally related proteins that are expressed in a tissue-specific manner (5). GLUT-4 is the major isoform present in both human and rat skeletal muscle, whereas the GLUT-1 and GLUT-5 isoforms are expressed at a much lower abundance (58, 62). The major mediators of glucose transport activity 0193-1849/97 $5.00 Copyright r 1997 the American Physiological Society E1039 E1040 INVITED REVIEW in muscle are fiber contractions and insulin, although numerous other factors including catecholamines, hypoxia, growth factors, and corticosteroids can alter glucose transport. Glucose transport in skeletal muscle follows saturation kinetics, and most reports have shown that exercise and insulin increase glucose transport through an increase in the maximal velocity of transport (Vmax ) without an appreciable change in the substrate concentration at which glucose transport is half-maximal, or Km (43, 52, 86, 87). This increase in transport Vmax may occur through an increase in the rate that each carrier protein transports glucose (transporter turnover number), an increase in the number of functional glucose transporter proteins present in the plasma membrane, or both. Glucose Transporter Translocation In the early 1980s studies in rat adipose cells demonstrated that a major mechanism for the insulin-induced increase in glucose transport was through stimulating the movement of glucose transporter proteins from an intracellular ‘‘microsomal’’ compartment to the plasma membrane (19, 114). Despite its physiological importance, parallel studies were not initially performed in skeletal muscle because the complex ultrastructure and great abundance of contractile proteins made it very difficult to prepare subcellular fractions from this tissue. However, by the late 1980s, essentially two different techniques for the preparation of intracellular and plasma membranes had been developed for use in skeletal muscle (48, 49, 64, 112). These methods, which we will refer to as the Klip (64) and Hirshman-modified Grimditch (48) techniques, have been the most commonly used preparations for the study of glucose transporter physiology in rat, mouse, and human skeletal muscle. The membrane fractions derived from these preparations, or modifications thereof, have been used to measure total glucose transporter number by use of the cytochalasin B binding assay, GLUT-1 and GLUT-4 proteins by immunoblotting, and the rate of glucose transport into the isolated plasma membrane vesicles. An inherent weakness associated with preparing subcellular fractions in skeletal muscle is the relatively low recovery of plasma membranes (#15%). In addition, although the preparations are devoid of sarcoplasmic reticulum and mitochondrial membranes, there is often some degree of cross contamination of plasma and intracellular membranes. Despite these limitations, the use of these fractionation methods over the past several years has substantially advanced our fundamental understanding of the glucose transport system in skeletal muscle. To test the hypothesis that the translocation of glucose transporters is a major mechanism by which physical exercise increases glucose uptake, initial experiments studied skeletal muscles obtained from rats that were exercised by running on a motorized rodent treadmill. By use of either the Hirshman/Grimditch or Klip fractionation technique, in all but one study (113) exercise has consistently been reported to increase the number of glucose transporters in the plasma mem- brane fraction (Table 1) (23–25, 29, 36–38, 49, 102, 106). In addition, sciatic nerve stimulation, resulting in contraction of hindlimb skeletal muscles in situ, also increases plasma membrane glucose transporter number in the rat (9, 27, 31, 39). The exercise-induced translocation of glucose transporters is due to an increase in the plasma membrane content of the GLUT-4 isoform, because a single bout of exercise does not alter the abundance of plasma membrane GLUT-1 (23, 36, 38) or GLUT-5 (66). Exercise-induced GLUT-4 translocation occurs in both red and white skeletal muscle fibers (38) and also apparently occurs in response to swim exercise in rats (16). In addition to subcellular fractionation methods, sarcolemmal giant vesicles have been prepared and used to study the effects of exercise on GLUT-4 translocation in skeletal muscle (94). Although the use of these giant vesicles is limited because of very low protein recoveries and a failure to respond to insulin stimulation (94), this technique has recently been used to demonstrate that both maximal (67) and submaximal (68) bicycle exercise significantly increases sarcolemmal GLUT-4 protein in human vastus lateralis muscle. Similar to the effects of physical exercise, insulin also causes GLUT-4 translocation in rat skeletal muscle (23, 38, 39, 48). Because blood flow is increased during exercise, it could be hypothesized that the exerciseinduced recruitment of GLUT-4 to the plasma membrane is secondary to increased delivery of insulin to the working muscles. However, when hindlimb skeletal muscles are contracted in situ in the absence of insulin, plasma membrane GLUT-4 is increased to a similar degree to what occurs with exercise in vivo (9, 27, 31, 39). These findings demonstrate that contraction can recruit GLUT-4 to the plasma membrane in rat skeletal muscle independently of insulin, and they provide a mechanism for earlier reports showing that insulin is not required for muscle contraction to increase glucose uptake in skeletal muscle (92, 100, 124). The plasma membrane fractions that are derived from both the Klip and Hirshman/Grimditch preparations are a mixture of both surface membranes and transverse tubules, the membrane folds that extend inward from the plasma membrane (78 and M. F. Hirshman, E. S. Horton, and L. J. Goodyear, unpublished observations). By a modification of the Klip procedure to separate transverse tubules from outwardfacing surface membranes (78), it has been estimated that a significant percentage of the GLUT-4 that is translocated to the plasma membrane fraction with exercise associates with nonjunctional transverse tubules (102). The exercise-induced redistribution of GLUT-4 to transverse tubules probably functions to increase the overall rate of glucose transport into the muscles and facilitate glucose transport deep into the contracting muscle fibers (102). Although numerous studies have used subcellular fractionation methods to demonstrate that exercise and insulin stimulate the redistribution of GLUT-4 to the plasma membrane in skeletal muscle, more recently a technique that measures cell surface GLUT-4 protein E1041 INVITED REVIEW Table 1. Effects of exercise on the subcellular distribution of glucose transporters in normal rat skeletal muscle Method/Assay Exercise Effect PM Transporters Treatment* Exercise 1 Insulin PM Transporters Exercise Effect IM Transporters Hirshman et al. 1988 (49) Fractionation—H/G CB binding Treadmill run, 60 min > 100% Douen et al. 1989 (24) Fractionation—Klip CB binding Treadmill run, 45 min > 100% & Fushiki et al. 1989 (29) Fractionation—H/G and Klip CB binding Treadmill run, 2 hr > 54% (H/G) > 47 (Klip) < 48% (H/G) < 81% (Klip) Sternlicht et al. 1989 (113) Fractionation—H/G CB binding Treadmill run, 45 min Insulin injection & No additive effect, but no effect of exercise alone Goodyear et al. 1990 (39) Fractionation—H/G CB binding Hindlimb perfusion with contraction, insulin > 72% No additive effect, but no effect on glucose uptake Goodyear et al. 1990 (37) Fractionation—H/G CB binding Treadmill run, 60 min > 80% 0 min post Muscles obtained 0, 30, > 60% 30 min post or 120 min postexer- & 120 min post cise Douen et al. 1990 (23) Fractionation—Klip CB binding, GLUT-4 blotting Treadmill run, 45 min > 65% CB binding Insulin hindlimb perfu- > 150% GLUT-4 sion Douen et al. 1990 (25) Fractionation—Klip CB binding, GLUT-4 blotting Treadmill run, 45 min > 60% CB binding > 150% GLUT-4 & Goodyear et al. 1991 (36) Fractionation—H/G CB binding, GLUT-4 blotting Treadmill run, 60 min > 50% CB binding > 45% GLUT-4 < 30% CB binding < 25% GLUT-4 Goodyear et al. 1991 (38) Fractionation—H/G CB binding, GLUT-4 blotting Treadmill run, 60 min CB binding: Red & white gastrocne> 40% red, 100% mius muscle studied white GLUT-4: > 75% red, 79% white Etgen et al. 1993 (27) Fractionation—H/G GLUT-4 blotting Hindlimb perfusion with contraction > 67% Brozinick et al. 1994 (9) Fractionation—H/G CB binding, GLUT-4 blotting Hindlimb perfusion with contraction, insulin > 96% CB binding > 62% GLUT-4 No additive effect & CB binding & GLUT-4 Gao et al. 1994 (31) Fractionation—H/G GLUT-4 blotting Insulin infusion followed by contraction in situ > 113% Fully additive effect < 25% Lund et al. 1995 (75) Bis-mannose photolabel with GLUT-4 Contraction, insulin of soleus muscles in vitro > 397% Partially additive (84%) Coderre et al. 1995 (16) Fractionation—modi- Swimming, 30 min fied Klip GLUT-4 blotting Sherman et al. 1996 (106) Fractionation—H/G GLUT-4 blotting Treadmill run, 60 min Roy and Marette Fractionation—modi- Treadmill run, 45 min 1996 (102) fied Klip GLUT-4 blotting No additive effect using & either assay & < 45% in novel fraction > 40% < 48% > 95% PM > 60% t tubules < 40% in novel fraction PM, plasma membrane; IM, intracellular membrane; H/G, Hirshman-modified Grimditch fractionation technique; CB, cytochalasin B; t tubules, transverse tubules. * Insulin treatment is included only if the combination of exercise/contraction and insulin was studied. using a membrane-impermeable bis-mannose photolabel has been developed (54). By use of this exofacial labeling method, measurement of plasma membrane GLUT-4 protein is not affected by contamination of GLUT-4 originating from internal membranes, resulting in low basal levels of plasma membrane glucose transporters and significantly greater multiples of increase in response to various stimuli. Indeed, when this method was adapted to study rat soleus muscles incubated in vitro (75, 125), contraction increased plasma membrane GLUT-4 protein by nearly fourfold (75). Immunocytochemical analysis of skeletal muscle sec- E1042 INVITED REVIEW tions by electron microscopy has also been used to study the subcellular distribution of GLUT-4. Although not studied individually, the combination of exercise and insulin results in a substantial increase in GLUT-4 immunodetected in the plasma membranes (101). Taken together, all of these studies provide overwhelming evidence that a major mechanism for the exerciseinduced stimulation of glucose uptake in skeletal muscle involves the recruitment of glucose transporters to the plasma membrane. Furthermore, contraction in the absence of insulin, as well as insulin alone, can independently result in the movement of glucose transporters to the plasma membrane (Fig. 1). The increase in muscle glucose transport with the combination of a maximal contraction stimulus and a maximal insulin stimulus is greater than the effect of either contraction or insulin alone (32, 87, 123, 134). This ‘‘additive’’ effect of contraction plus insulin on glucose transport is consistent with the hypothesis that the two stimuli can act independently. If the amount of GLUT-4 in the plasma membrane is the limiting factor for glucose transport, the combination of contraction and insulin should result in a similarly additive effect on the recruitment of GLUT-4 to the plasma membrane. However, there has been considerable discrepancy among studies that have examined this question (Table 1) (9, 23, 31, 75). When treadmill exercise (23) or contractions in situ (9) were combined with a maximal insulin treatment, there was a partially additive effect on muscle glucose uptake, but the increase in plasma membrane glucose transporters was not greater than the effect of exercise or insulin alone. These results, which assessed glucose transporters in plasma membranes purified by fractionation, suggest that the additive effect of exercise and insulin on glucose uptake is due to an increase in transporter turnover number. In contrast to these findings is a study that also used subcellular fractionation methods but reported that the combination of insulin with contractions in situ has a fully additive effect on increasing plasma membrane GLUT-4 (31). Furthermore, with use of the exofacial labeling method in rat soleus muscles, the combination of contraction and insulin treatments resulted in an almost completely additive increase in plasma membrane GLUT-4 protein (75). Thus the results of two studies suggest that the increase in GLUT-4 at the plasma membrane is the sole mechanism for the increase in glucose transport (31, 75), whereas the two other studies raise the possibility that exercise increases glucose transporter turnover number (9, 23), a process that is frequently referred to as ‘‘intrinsic activity.’’ Fig. 1. GLUT-4 translocation in skeletal muscle. Muscle contractions and insulin cause translocation of GLUT-4 glucose transporter proteins to plasma membrane and transverse tubules (T-tubules). GLUT-1 and GLUT-5 are present in plasma membrane. The subcellular origin of GLUT-4-containing vesicles is not clear, but exercise and insulin appear to recruit distinct GLUT-4-containing vesicles and/or mobilize different ‘‘pools’’ of GLUT-4 proteins. Insulin-stimulated GLUT-4 translocation involves insulin receptor substrate 1 (IRS-1) and phosphatidylinositol (PI) 3-kinase and redistribution of Rab4. Contraction utilizes a PI 3-kinase- and mitogen-activated protein kinase (MAPK)-independent mechanism and does not result in redistribution of Rab4. Contraction signal is probably initiated by release of calcium from sarcoplasmic reticulum and may involve an autocrine/paracrine mechanism (e.g., nitric oxide, adenosine, bradykinin), protein kinase C (not shown), or a combination of these and other currently unknown factors. NO, nitric oxide; JNK, c-Jun NH2-terminal kinase. INVITED REVIEW Glucose Transporter Turnover Number In most early studies of adipose cells and skeletal muscle, the incremental increase in the rate of insulinor exercise-stimulated glucose transport was greater than the increased recruitment of glucose transporters to the cell surface, suggesting an increase in transporter turnover number. To measure transporter turnover number in skeletal muscle, glucose transport into isolated plasma membrane vesicles is assayed using the same plasma membrane preparation that is used to measure total glucose transporter number by the Dglucose-inhibitable cytochalasin B binding assay (38, 60). The transporter turnover number is calculated by dividing the glucose transport Vmax by the total glucose transporter number (R0 ), which is determined by Scatchard analysis of cytochalasin B binding data in the absence or presence of glucose. By use of these methods, exercise was shown to increase glucose transport Vmax by fourfold and R0 by twofold, resulting in a doubling of the transporter turnover number and suggesting that the mechanism for the exercise-induced increase in skeletal muscle glucose uptake involves both the translocation of glucose transporters to the plasma membrane and an increase in the average intrinsic activity of the transporters that are present in the plasma membrane (38, 60). One limitation of this method is that it does not discriminate the activity of the individual glucose transporter isoforms, and thus a change in activity could reflect the recruitment of a more active transporter isoform to the plasma membrane. In fact, studies using Xenopus laevis oocytes suggest that GLUT-4 has a higher intrinsic activity than GLUT-1 (88) and, as discussed above, only GLUT-4 is recruited to the plasma membrane in response to exercise (23, 36, 38). When transporter translocation is assessed using the GLUT-4-specific exofacial labeling method, the contraction-stimulated increases in the rate of glucose transport into the isolated soleus muscles and GLUT-4 recruitment to the plasma membrane were nearly identical (75). Thus, although there may be some conditions that directly modify glucose transporter activity (111), it is unlikely that exercise increases the intrinsic activity of the individual glucose transporter isoforms. Instead, exercise probably increases the average turnover number of all transporters in the plasma membrane by recruiting the more active GLUT-4. Separate ‘‘Pools’’ of Glucose Transporters for Exercise and Insulin? If the combination of exercise and insulin has additive effects on glucose transport and GLUT-4 recruitment to the plasma membrane, then at some level there must be different mechanisms leading to the stimulation of muscle glucose transport. Data from several studies have suggested that this could result from two distinct intracellular locations or pools of glucose transporters, one that responds to exercise and one that responds to insulin (23–25). In these reports, insulin, but not exercise, was shown to decrease glucose trans- E1043 porters from an intracellular microsomal membrane fraction (Table 1). Interestingly, the differential effects of exercise and insulin to decrease glucose transporters in the intracellular membrane fraction have only been consistently demonstrated when the Klip fractionation procedure was used, suggesting that the Klip and Hirshman/Grimditch methods isolate different populations of intracellular membranes. Recently, modification of the Klip procedure has resulted in the isolation of a novel intracellular membrane fraction that is sensitive to exercise (16, 102), giving further support to the hypothesis that there are separate pools of glucose transporters in skeletal muscle. Surprisingly, although there are different sedimentation coefficients for the insulin- and exercise-sensitive fractions, there appears to be very little difference in the major protein composition of these fractions (16). Regulation of GLUT-4 Vesicular Translocation The majority of intracellular GLUT-4 is located in small tubulo-vesicular organelles (48, 101), and it is still not completely clear whether these vesicles are unique intracellular compartments or ubiquitously expressed organelles that are enriched in GLUT-4. As has recently been reviewed in detail (111), most studies in adipose cells suggest that there is a low rate of continuous recycling of GLUT-4 in the basal state and that insulin acts primarily through increasing transporter exocytosis. The molecular mechanism by which exercise stimulates the movement of these GLUT-4-containing vesicles to the cell surface in skeletal muscle is not known. Proteins that have been identified as components of GLUT-4-containing vesicles in skeletal muscle include the vesicle-associated membrane protein-2 [VAMP-2; also called synaptobrevin 2 (67, 121)], cellubrevin [also called VAMP-3 (121)], gp160 (16, 80), and Rab4 (106). Both gp160 (16) and VAMP-2 (67) have been shown to translocate in response to physical exercise in skeletal muscle, similar to the effects of insulin. In contrast to the similar effects of exercise and insulin on gp160 and VAMP-2 distribution, there are differential effects of exercise and insulin on the redistribution of Rab-4 (106). Rab proteins are guanosine triphosphate (GTP)-binding proteins that are thought to be involved in all vesicular activity (formation, targeting, fusion) and may act as molecular switches, catalyzing membrane trafficking events by conversion from an inactive guanosine diphosphate-bound form to an active GTP-bound form (109, 118). Studies in adipose cells suggest that the Rab4 isoform is involved in insulin-stimulated GLUT-4 translocation (18, 108). By use of the Hirshman/Grimditch fractionation technique in skeletal muscle, both insulin and exercise have been shown to decrease GLUT-4 in the microsomal membranes, but only insulin caused a redistribution of Rab4 from this fraction (106). Consistent with these findings is work showing that insulin and exercise both cause an increase in the plasma membrane content of small GTP-binding proteins (as assessed by [32P]GTP-binding overlay assays), whereas only insulin treatment re- E1044 INVITED REVIEW sulted in a concomitant decrease in these proteins in the intracellular microsomal fraction (27). Although these experiments using nonspecific GTP-binding proteins and Rab4 as markers do not necessarily contradict the hypothesis that insulin- and exercise-stimulated transporters originate from different locations in the muscle fibers, the findings do suggest that there may be distinct GLUT-4-containing vesicles, some that are sensitive to insulin and some that are sensitive to exercise. Thus there could be a common subcellular location of transporters with different molecular ‘‘switches’’ for mobilization. Future studies will be necessary to determine the exact location of exerciseand insulin-stimulated GLUT-4 vesicles and the vesicular machinery that regulates the redistribution of these organelles in skeletal muscle. SIGNALING MECHANISMS FOR EXERCISE-STIMULATED GLUCOSE TRANSPORT Whereas considerable progress has been made in understanding the role of glucose transporter proteins in the stimulation of glucose transport with exercise, much less is known about the intracellular signaling mechanisms that lead to exercise-stimulated GLUT-4 translocation. However, over the past several years there have been many advances in elucidating the signaling components involved in insulin-stimulated GLUT-4 translocation. Because exercise and insulin both increase glucose uptake through the translocation of GLUT-4, several studies have determined whether these two stimuli share the same signaling intermediaries. Phosphatidylinositol 3-Kinase Numerous studies in various cell types have demonstrated that the activation of phosphatidylinositol 3kinase (PI 3-kinase) is necessary for the stimulation of GLUT-4 translocation (see reviews in 13, 14). In skeletal muscle, insulin stimulation results in the rapid phosphorylation of the insulin receptor and insulin receptor substrate 1 (IRS-1) on tyrosine residues and activation of PI 3-kinase (28, 34). Inhibition of PI 3-kinase by pharmacological blockade by wortmannin has shown that PI 3-kinase is an essential molecule for insulin-stimulated GLUT-4 translocation (75) and glucose transport (73–75, 127, 129) in skeletal muscle. In contrast, these initial signaling events in insulin action that lead to GLUT-4 translocation do not appear to be involved in the mechanism for exercise-stimulated glucose transport. Exercise has no effect on autophosphorylation of isolated insulin receptors (99), and contraction of hindlimb muscles by electrical stimulation of sciatic nerves has no effect on tyrosine phosphorylation of the insulin receptor and IRS-1 or PI 3-kinase activity (34, 127). Furthermore, wortmannin does not inhibit glucose transport in isolated rat muscle incubated and contracted in vitro (73, 75, 129). In contrast to these findings, one study has shown that wortmannin can partially inhibit contraction-stimulated glucose transport in perfused rat hindlimb muscles without confounding effects on contractility or oxygen uptake (127). However, this effect of wortmannin might be independent of effects on PI 3-kinase (127). Thus the majority of studies suggest that, although exercise and insulin both recruit GLUT-4 to the plasma membrane and activate glucose transport, there are distinct signaling mechanisms that lead to the translocation of glucose transporters in skeletal muscle. Calcium and Protein Kinase C Muscle contraction is initiated by depolarization of the plasma membrane, triggering the release of calcium from the sarcoplasmic reticulum. The spike in intracellular calcium leads to the interaction of actin and myosin filaments, resulting in the development of tension in the muscle fibers. Of these events, the increase in cytoplasmic calcium concentrations has long been considered a critical mediator or initiator of contraction-stimulated glucose transport (50), and this topic has recently been reviewed in detail (51). The calcium hypothesis is supported by various lines of evidence, including an early study in amphibian muscle showing that the incremental increase in contractionstimulated transport correlates with the frequency of contraction, not the amount of work or tension developed (52). A role for membrane depolarization in contraction-stimulated glucose transport was also ruled out by an early study showing that caffeine, an agent that causes contraction by increasing calcium release from the sarcoplasmic reticulum in the absence of membrane depolarization, increases glucose transport in isolated amphibian muscle (53). Several studies have shown that rates of glucose transport are increased in mammalian muscle when cytoplasmic calcium concentrations are raised using various agents (45, 50, 130), and dantrolene, which prevents the release of calcium from sarcoplasmic reticulum, blocks glucose transport in skeletal muscle (89, 130). All of these studies provide indirect evidence that exercise utilizes a calciumsensitive glucose transport system. However, it should be noted that, although calcium can activate glucose transport in skeletal muscle, an increase in intracellular calcium does not share all the characteristics of exercise. For example, calcium-induced glucose transport actually inhibits insulin-induced glucose transport (26, 72), a response that clearly contrasts with the effects of exercise. If calcium is involved in regulating exercise-stimulated glucose transport, then calcium ions probably do not directly activate the glucose transport system. This is because cytoplasmic calcium concentrations are elevated for only a fraction of a second after each muscle contraction, whereas the increase in muscle glucose transport can remain elevated for a considerable period of time after the contractile activity ceases. Instead, the rise in cytosolic calcium may initiate or facilitate the activation of intracellular signaling molecules or cascades of signaling proteins that lead to both the immediate and prolonged effects of exercise on muscle glucose transport. Protein kinase C (PKC) is an example of a calciumdependent signaling intermediary that may be activated by muscle contraction (15, 96). Downregulation of INVITED REVIEW PKC by long-term phorbol ester treatment (15) and inhibition of PKC using polymyxin B (47, 131) have both been associated with decreases in contractionstimulated glucose transport. However, caution must be taken in interpreting these data, because polymyxin B is not a specific inhibitor of PKC, and both of these treatments can result in decreased contractility of the muscle fibers. Furthermore, early studies that measured PKC activity in muscle used the nonspecific kinase substrate histone IIIS, and it is now known that contraction can increase the activity of numerous kinases in skeletal muscle (1, 85). If PKC is involved in regulating contraction-stimulated glucose transport, then it will be important to determine which of the 12 different PKC isoforms that have been identified in mammalian cells are responsible. PKC isoforms have been classified into three subfamilies on the basis of amino acid similarity and mode of activation: conventional PKCs (cPKC), novel PKCs (nPKC), and atypical PKCs (aPKC). Skeletal muscles express the a, bI, and bII isoforms (128 and D. J. Sherwood and L. J. Goodyear, unpublished observations), members of the cPKC subfamily that are calcium dependent and sensitive to phorbol ester stimulation. Because phorbol esters can modestly stimulate glucose transport in skeletal muscle (45, 56, 110), by analogy it is possible to deduce that if these specific isoforms are stimulated by muscle contraction, they may be involved in the regulation of contraction-stimulated glucose transport. Interestingly, skeletal muscle also expresses very high levels of the u isoform (128) and lower levels of the e, h, d, and z PKCs (55, 128 and D. J. Sherwood and L. J. Goodyear, unpublished observations). These proteins belong to the nPKC or aPKC subfamilies, isoforms that do not require calcium for activation. If exercise stimulates these PKC isoforms, it will be interesting to determine whether they are involved in regulating glucose transport or other biological effects of contraction in skeletal muscle. Autocrine/Paracrine Mechanisms Studies in cultured skeletal and cardiac muscle cells have suggested that mechanical stretch can activate intracellular signaling pathways by releasing growth factors, which in turn stimulate cell surface receptors and subsequently second messenger systems (104, 117). In adult skeletal muscle, there is also evidence that contracting skeletal muscle can evoke an autocrine and/or paracrine response. This type of mechanism may function to help activate cell-signaling molecules such as PKC and subsequently lead to the increase in glucose transport. Nitric oxide is an example of a molecule that may act on skeletal muscle through an autocrine or paracrine mechanism, and recent evidence suggests that nitric oxide may be involved in regulating contraction-stimulated glucose transport. Nitric oxide is released from skeletal muscle contracted in vitro, and inhibition of nitric oxide synthase has been demonstrated to decrease both basal (3) and contractionstimulated (4) rates of muscle glucose transport, an effect that may be regulated by a guanosine 38,58-cyclic monophosphate-mediated mechanism (2, 132). Interest- E1045 ingly, consistent with the concept that exercise and insulin act through distinct signaling mechanisms, there was no effect of nitric oxide synthase inhibition on insulin-stimulated glucose transport in skeletal muscle (4). Another molecule that may be involved with contraction-stimulated glucose transport is kallikrein, which catalyzes the production of bradykinin and is a potential stimulator of nitric oxide synthase. Kallikrein is predominantly expressed in slow-twitch red muscles, the fiber type that expresses greater amounts of GLUT-4 (81). Adenosine has also been shown to be secreted from contracting muscle fibers (105), and the adenosine receptor has been suggested to mediate the signaling mechanism through which contraction results in the synergistic stimulation of insulin-stimulated glucose transport (119). Other Putative Mechanisms Several other intracellular signaling proteins have been shown to be activated in response to physical exercise; however, to date there is no evidence to suggest that these molecules regulate contractionstimulated glucose transport. For example, exercise activates the mitogen-activated protein (MAP) kinase signaling cascade in both rat (33) and human (1) skeletal muscle, but we have recently demonstrated that inhibition of MAP kinase signaling by use of pharmacological blockade (PD-98059) has no effect on contraction-stimulated glucose transport in vitro (Hayashi and Goodyear, unpublished observations) or in the perfused hindlimb (J. F. P. Wojtaszewski, A. B. Jacobsen, and E. A. Richter, unpublished observations). The c-Jun NH2-terminal kinase (JNK) and p38 kinase signaling cascades are also stimulated by physical exercise in skeletal muscle (33). It is not known whether these signaling cascades mediate the effects of contraction on carbohydrate metabolism, although one recent report has suggested that JNK signaling is involved in the regulation of insulin-stimulated glycogen synthesis in skeletal muscle (84). Because these signaling cascades have been suggested to regulate gene transcription in other cell types, activation of these pathways by acute exercise may function to regulate more chronic adaptations to repeated bouts of exercise. The glycogenolytic process may also play a role in the regulation of exercise-induced GLUT-4 translocation in skeletal muscle. Although there is still no direct evidence, it has long been hypothesized that transporter molecules are associated with glycogen particles in the muscle and that the contraction-stimulated hydrolysis of glycogen releases GLUT-4, leading to translocation of these transporters to the cell surface. Future studies will be needed to directly test this hypothesis, and work in other areas is needed to precisely define the role of the other putative mechanisms that have been discussed in this review. With continued focus in this area, along with the development of novel methodologies, we should soon have a clearer understanding of the molecular basis for exercise-induced increases in muscle glucose uptake. E1046 INVITED REVIEW MECHANISMS FOR POSTEXERCISE INCREASES IN MUSCLE INSULIN SENSITIVITY Increased insulin sensitivity of skeletal muscle glucose uptake is usually observed after a single bout of exercise. This was first shown in perfused rat muscles (57, 97) and has since been verified in numerous human studies (6, 21, 82, 99). By use of one-legged exercise models, it has become clear that the exercise-induced increase in insulin sensitivity is a local phenomenon restricted to the exercised muscles (98, 99). In addition to the glucose transport step (12, 97, 98, 123), prior exercise potentiates insulin-stimulated glycogen synthesis (71, 97, 98) and amino acid transport (133). Carbohydrate deprivation in the postexercise period prolongs the increased insulin sensitivity in rat muscle (12) and, in fact, no reversal of the increased insulin sensitivity is observed in incubated muscles when the nonmetabolizable 2-deoxyglucose is substituted for D-glucose (40). Thus the rate that glucose is stored or metabolized in the postexercise period may be involved in the reversal of the increased insulin sensitivity of muscle glucose uptake and may partially explain the different durations of the increased insulin sensitivity reported (20, 82, 91, 97). Several studies have determined whether enhanced insulin binding or insulin signaling are mechanisms for the increase in muscle insulin sensitivity after exercise. However, there is no difference in insulin clearance rates between rested and exercised legs 4 h after one-legged exercise in humans (99), and the majority of studies show that prior exercise does not change insulin binding to its receptor (7, 115, 133). Prior exercise does not increase insulin-stimulated receptor tyrosine kinase activity in skeletal muscles obtained from rats (115) or humans (126) and, in fact, prior contraction of rat hindlimb skeletal muscles has been shown to cause a paradoxical decrease in insulin-stimulated tyrosine phosphorylation of the insulin receptor and IRS-1, and receptor- and IRS-1-associated PI 3-kinase activities (34). Consistent with these findings are recent studies showing that insulin’s ability to activate IRS-1-associated PI 3-kinase activity in vivo is diminished in previously exercised humans (126). This mismatch between the signaling events and the end point of cellular activation (glucose uptake) suggests that IRS1-associated PI 3-kinase activity is not the sole mediator of insulin-stimulated glucose transport in skeletal muscle. Furthermore, these findings provide additional support to the hypothesis that exercise and insulin act through distinct signaling mechanisms. Clues leading to the mechanism of increased insulin sensitivity may come from studies in which the postexercise period is not characterized by increased insulin sensitivity. In contrast to exercise in vivo (98) or contraction of hindlimb muscles during perfusion (100), when intact muscles are isolated, washed, and then contracted in vitro, there is no increase in insulin sensitivity after contractions (11). This work and a subsequent report have suggested that a serum factor, probably a protein, is required for the effects of contrac- tion to enhance insulin sensitivity (30). Other work has indicated that adenosine receptors may mediate the ability of muscle contraction to increase insulinstimulated glucose uptake (119), and another hypothesis, based on the finding that prior exercise can also increase hypoxia-stimulated glucose transport, suggests that the glucose transport system is simply left in a more easily recruitable state in the period after glycogen-depleting exercise (11). Taken together, these studies suggest that there may be no single factor that regulates the enhanced muscle insulin sensitivity for glucose uptake in the postexercise state. Instead, this physiological phenomenon may be regulated by a combination of humoral factors, autocrine/paracrine mechanisms, and muscle glycogen concentrations. EFFECTS OF EXERCISE ON GLUCOSE TRANSPORT IN THE INSULIN-RESISTANT STATE Exercise has long been advocated as beneficial for patients with non-insulin-dependent diabetes mellitus (NIDDM), partially because, even in the face of insulin resistance, physical work can stimulate muscle glucose uptake. This observation is consistent with the thesis that exercise and insulin stimulate muscle glucose transport by distinct mechanisms. Thus, it is not surprising that a variety of animal models of insulin resistance have been studied in an attempt to elucidate the mechanisms for exercise- and insulin-stimulated glucose transport. The obese Zucker rat has severe defects in insulinstimulated glucose uptake (107) and GLUT-4 translocation (61) despite normal levels of total muscle GLUT-4 protein (107). In contrast, these animals have normal increases in contraction-stimulated glucose uptake (8) and GLUT-4 translocation (10, 59). Similarly, shortterm immobilization (120) and high-fat feeding (70), two animal models that result in insulin resistance with preserved muscle GLUT-4 protein concentrations, also have normal rates of exercise-stimulated glucose transport. However, longer periods of immobilization (22, 93) and high-fat feeding (41) that decrease total GLUT-4 protein in the muscle result in significant decreases in exercise-induced muscle glucose transport. Impaired exercise-stimulated glucose transport is also present when severe insulin resistance of muscle glucose transport and decreased muscle GLUT-4 mRNA and protein levels are caused by a short period of denervation (46, 116), treatment with streptozotocin (63, 87, 124), or severe eccentric contractions (65). These animal studies suggest that exercise-stimulated glucose transport is impaired only under conditions in which total muscle GLUT-4 protein is markedly decreased. This is good news for patients with insulin-resistant conditions such as obesity and NIDDM, because these individuals generally have normal muscle GLUT-4 protein levels (42, 90). Indeed, in physiological models of insulin resistance and in patients with NIDDM in whom there is normal muscle GLUT-4 protein, the ability of exercise to increase glucose disposal is preserved. Obese NIDDM patients have a normal increase INVITED REVIEW in peripheral glucose utilization during moderate exercise (83), and recently, by application of the arteriovenous balance technique, the exercise-induced increase in leg glucose uptake was even higher in the nonobese NIDDM compared with the control subjects (79). The latter finding is probably caused by a greater mass action of glucose because of hyperglycemia, i.e., the leg glucose clearance rate in the exercise period was comparable in the nonobese NIDDM and control subjects. In both obese and nonobese NIDDM patients, the exerciseinduced increase in muscle glucose uptake, coupled with an impaired or delayed enhancement of hepatic glucose production, can cause a decrease in plasma glucose concentration (79, 83). The exercise-stimulated increase in glucose uptake in patients with NIDDM is probably a function of normal GLUT-4 translocation, although this question must still be addressed experimentally. On the basis of data from human subjects and the animal data discussed in previous sections, we can now hypothesize that insulin-resistant human patients can increase rates of muscle glucose uptake with exercise, because the muscle is able to bypass the previously described defects in the insulin-signaling molecules (35) and effectively activate the exercise-specific signaling mechanisms. SUMMARY AND FUTURE DIRECTIONS Over the past several years considerable progress has been made in understanding the molecular basis for the clinically important effects of physical exercise on glucose uptake in skeletal muscle. We now know that GLUT-4 plays a major role in regulating glucose transport in muscle during exercise, and although the exercise-induced signaling mechanism that leads to GLUT-4 translocation has not been elucidated, we are beginning to gain an understanding of this phenomenon. It is clear that exercise and insulin utilize distinct signaling pathways that lead to the activation of glucose transport in skeletal muscle, perhaps explaining why patients with insulin resistance can normally activate muscle glucose transport with exercise but not with insulin. Complete elucidation of the molecules involved in signaling the exercise-induced activation of glucose transport will be important, and these proteins are potential sites for future pharmacological intervention. As we learn more about the signaling intermediaries that regulate the effects of exercise on glucose transport, it will be critical to determine how these molecules adapt with chronic physical training. Because it is now known that long-term regular physical exercise can significantly reduce the risk of developing NIDDM in most populations (44, 76, 77), these studies should ultimately help us define the molecular basis for these important adaptations to skeletal muscle. This work was supported by National Institutes of Arthritis and Musculoskeletal and Skin Diseases Grant AR-42238, a grant from the Juvenile Diabetes Foundation International (both to L. J. Goodyear), and Grant 504–14 from the Danish National Research Foundation (to J. F. P. Wojtaszewski). T. Hayashi was supported by a fellowship grant from the Manpei Suzuki Diabetes Foundation. Address for reprint requests: L. J. Goodyear, Joslin Diabetes Center, Boston, MA 02215. E1047 REFERENCES 1. Aronson, D., M. A. Violan, S. D. Dufresne, D. Zangen, R. A. Fielding, and L. J. Goodyear. Exercise stimulates the mitogen-activated protein kinase pathway in human skeletal muscle. J. Clin. Invest. 99: 1251–1257, 1997. 2. Balon, T. W., A. P. Jasman, E. C. Balon, and J. L. Nadler. Skeletal muscle glucose transport is mediated by nitric oxide via a cGMP-related mechanism (Abstract). Med. Sci. Sports Exerc. 28: S58, 1996. 3. Balon, T. W., and J. L. Nadler. Nitric oxide release is present from incubated skeletal muscle preparations. J. Appl. Physiol. 77: 2519–2521, 1994. 4. Balon, T. W., and J. L. Nadler. Evidence that nitric oxide increases glucose transport in skeletal muscle. J. Appl. Physiol. 82: 359–363, 1997. 5. Bell, G. I., C. F. Burant, J. Takeda, and G. W. Gould. Structure and function of mammalian facilitative sugar transporters. J. Biol. Chem. 268: 19161–19164, 1993. 6. Bogardus, C., P. Thuillex, E. Ravussin, B. Vasquez, M. Narimiga, and S. Ashar. Effect of muscle glycogen depletion on in vivo insulin action in man. J. Clin. Invest. 72: 1605–1610, 1983. 7. Bonen, A., M. H. Tan, and W. M. Watson-Wright. Effects of exercise on insulin binding and glucose metabolism in muscle. Can. J. Physiol. Pharmacol. 62: 1500–1504, 1984. 8. Brozinick, J. T., Jr., G. J. Etgen, Jr., B. B. Yaspelkis III, and J. L. Ivy. Contraction-activated glucose uptake is normal in insulin-resistant muscle of the obese Zucker rat. J. Appl. Physiol. 73: 382–387, 1992. 9. Brozinick, J. T., Jr., G. J. Etgen, Jr., B. B. Yaspelkis III, and J. L. Ivy. The effects of muscle contraction and insulin on glucose-transporter translocation in rat skeletal muscle. Biochem. J. 297: 539–545, 1994. 10. Brozinick, J. T., G. J. Etgen, Jr., B. B. Yaspelkis III, and J. L. Ivy. Glucose uptake and GLUT-4 protein distribution in skeletal muscle of the obese Zucker rat. Am. J. Physiol. 267 (Regulatory Integrative Comp. Physiol. 36): R236–R243, 1994. 11. Cartee, G. D., and J. O. Holloszy. Exercise increases susceptibility of muscle glucose transport to activation by various stimuli. Am. J. Physiol. 258 (Endocrinol. Metab. 21): E390– E393, 1990. 12. Cartee, G. D., D. A. Young, M. D. Sleeper, J. Zierath, H. Wallberg-Henriksson, and J. O. Holloszy. Prolonged increase in insulin-stimulated glucose transport in muscle after exercise. Am. J. Physiol. 256 (Endocrinol. Metab. 19): E494– E499, 1989. 13. Cheatham, B., C. J. Vlahos, L. Cheatham, L. Wang, J. Blenis, and C. R. Kahn. Phosphatidylinositol 3-kinase activation is required for insulin stimulation of pp70 S6 kinase, DNA synthesis, and glucose transporter translocation. Mol. Cell. Biol. 14: 4902–4911, 1994. 14. Clarke, J. F., P. W. Young, K. Yonezawa, M. Kasuga, and G. D. Holman. Inhibition of the translocation of GLUT1 and GLUT4 in 3T3-L1 cells by the phosphatidylinositol 3-kinase inhibitor, wortmannin. Biochem. J. 300: 631–635, 1994. 15. Cleland, P. J., G. J. Appleby, S. Rattigan, and M. G. Clark. Exercise-induced translocation of protein kinase C and production of diacylglycerol and phosphatidic acid in rat skeletal muscle in vivo. Relationship to changes in glucose transport. J. Biol. Chem. 264: 17704–17711, 1989. 16. Coderre, L., K. V. Kandror, G. Vallega, and P. F. Pilch. Identification and characterization of an exercise-sensitive pool of glucose transporters in skeletal muscle. J. Biol. Chem. 270: 27584–27588, 1995. 17. Connett, R. J., and K. Sahlin. Control of glycolysis and glycogen metabolism. In: Handbook of Physiology. Exercise: Regulation and Integration of Multiple Systems. Bethesda, MD: Am. Physiol. Soc., 1996, sect. 12, chapt. 19, p. 870–911. 18. Cormont, M., J.-F. Tanti, A. Zahraoui, E. Van Obberghen, A. Tavitian, and Y. Le Marchand-Brustel. Insulin and okadaic acid induce Rab4 redistribution in adipocytes. J. Biol. Chem. 268: 19491–19497, 1993. 19. Cushman, S. W., and L. J. Wardzala. Potential mechanism of insulin action on glucose transport in the isolated rat adipose E1048 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. INVITED REVIEW cell: apparent translocation of intracellular transport systems to the plasma membrane. J. Biol. Chem. 255: 4758–4762, 1980. Dela, F., K. J. Mikines, M. von Linstow, N. H. Secher, and H. Galbo. Effect of training on insulin-mediated glucose uptake in human muscle. Am. J. Physiol. 263 (Endocrinol. Metab. 26): E1134–E1143, 1992. Devlin, J. T., M. F. Hirshman, E. S. Horton, and E. D. Horton. Enhanced peripheral insulin and spanchnic insulin sensitivity in NIDDM men after single bout of exercise. Diabetes 36: 434–439, 1987. Didyk, R. B., E. E. Anton, K. A. Robinson, D. R. Menick, and M. G. Buse. Effect of immobilization on glucose transporter expression in rat hindlimb muscles. Metabolism 43: 1389–1394, 1994. Douen, A. G., T. Ramlal, G. D. Cartee, and A. Klip. Exercise modulates the insulin-induced translocation of glucose transporters in rat skeletal muscle. FEBS Lett. 261: 256–260, 1990. Douen, A. G., T. Ramlal, A. Klip, D. A. Young, G. D. Cartee, and J. O. Holloszy. Exercise-induced increase in glucose transporters in plasma membranes of rat skeletal muscle. Endocrinology 124: 449–454, 1989. Douen, A. G., T. Ramlal, S. Rastogi, P. J. Bilan, G. D. Cartee, M. Vranic, J. O. Holloszy, and A. Klip. Exercise induces recruitment of the ‘‘insulin-responsive glucose transporter.’’ Evidence for distinct intracellular insulin- and exerciserecruitable transporter pools in skeletal muscle. J. Biol. Chem. 265: 13427–13430, 1990. Draznin, B., K. E. Sussman, M. Kao, and N. Sherman. The existence of an optimal range of cytosolic free calcium for insulin-stimulated glucose transport in rat adipocytes. J. Biol. Chem. 262: 14385–14388, 1987. Etgen, G. J., Jr., A. R. Memon, G. A. Thompson, Jr., and J. L. Ivy. Insulin- and contraction-stimulated translocation of GTP-binding proteins and GLUT4 protein in skeletal muscle. J. Biol. Chem. 20164–20169, 1993. Folli, F., M. J. A. Saad, J. M. Backer, and C. R. Kahn. Insulin stimulation of phosphatidylinositol 3-kinase activity and association with insulin receptor substrate 1 in liver and muscle of the intact rat. J. Biol. Chem. 267: 22171–22177, 1992. Fushiki, T., J. A. Wells, E. B. Tapscott, and G. L. Dohm. Changes in glucose transporters in muscle in response to exercise. Am. J. Physiol. 256 (Endocrinol. Metab. 19): E580– E587, 1989. Gao, J., E. A. Gulve, and J. O. Holloszy. Contraction-induced increase in muscle insulin sensitivity: requirement for a serum factor. Am. J. Physiol. 266 (Endocrinol. Metab. 29): E186–E192, 1994. Gao, J., J. Ren, E. A. Gulve, and J. O. Holloszy. Additive effect of contractions and insulin on GLUT-4 translocation into the sarcolemma. J. Appl. Physiol. 77: 1597–1601, 1994. Garetto, L. P., E. A. Richter, M. N. Goodman, and N. B. Ruderman. Enhanced muscle glucose metabolism after exercise in the rat: the two phases. Am. J. Physiol. 246 (Endocrinol. Metab. 9): E471–E475, 1984. Goodyear, L. J., P.-Y. Chung, D. J. Sherwood, S. D. Dufresne, and D. E. Moller. Effects of exercise and insulin on mitogen-activated protein kinase signaling pathways in rat skeletal muscle. Am. J. Physiol. 271 (Endocrinol. Metab. 34): E403–E408, 1996. Goodyear, L. J., F. Giorgino, T. W. Balon, G. Condorelli, and R. J. Smith. Effects of contractile activity on tyrosine phosphoproteins and PI 3-kinase activity in rat skeletal muscle. Am. J. Physiol. 268 (Endocrinol. Metab. 31): E987–E995, 1995. Goodyear, L. J., F. Giorgino, L. A. Sherman, J. Carey, R. J. Smith, and G. L. Dohm. Insulin receptor phosphorylation, insulin receptor substrate-1 phosphorylation, and phosphatidylinositol 3-kinase activity are decreased in intact skeletal muscle strips from obese subjects. J. Clin. Invest. 95: 2195–2204, 1995. Goodyear, L. J., M. F. Hirshman, and E. S. Horton. Exerciseinduced translocation of skeletal muscle glucose transporters. Am. J. Physiol. 261 (Endocrinol. Metab. 24): E795–E799, 1991. Goodyear, L. J., M. F. Hirshman, P. A. King, E. D. Horton, C. M. Thompson, and E. S. Horton. Skeletal muscle plasma 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. membrane glucose transport and glucose transporters after exercise. J. Appl. Physiol. 68: 193–198, 1990. Goodyear, L. J., M. F. Hirshman, R. J. Smith, and E. S. Horton. Glucose transporter number, activity and isoform content in plasma membranes of red and white skeletal muscle. Am. J. Physiol. 261 (Endocrinol. Metab. 24): E556–E561, 1991. Goodyear, L. J., P. A. King, M. F. Hirshman, C. M. Thompson, E. D. Horton, and E. S. Horton. Contractile activity increases plasma membrane glucose transporters in absence of insulin. Am. J. Physiol. 258 (Endocrinol. Metab. 21): E667– E672, 1990. Gulve, E. A., G. D. Cartee, J. Zierath, V. M. Corpus, and J. O. Holloszy. Reversal of enhanced muscle glucose transport after exercise: roles of insulin and glucose. Am. J. Physiol. 259 (Endocrinol. Metab. 22): E685–E691, 1990. Han, X., T. Ploug, and H. Galbo. Effect of diet on insulin- and contraction-mediated glucose transport and uptake in rat muscle. Am. J. Physiol. 269 (Regulatory Integrative Comp. Physiol. 38): R544–R551, 1995. Handberg, A., A. Vaag, P. Damsbo, H. Beck-Nielsen, and J. Vinten. Expression of insulin regulatable glucose transporters in skeletal muscle from type 2 (non-insulin-dependent) diabetic patients. Diabetologia 33: 625–627, 1990. Hansen, P., E. Gulve, J. Gao, J. Schluter, M. Mueckler, and J. Holloszy. Kinetics of 2-deoxyglucose transport in skeletal muscle: effects of insulin and contractions. Am. J. Physiol. 268 (Cell Physiol. 37): C30–C35, 1995. Helmrich, S. P., D. R. Ragland, R. W. Leung, and R. S. Paffenbarger. Physical activity and reduced occurrence of non-insulin-dependant diabetes mellitus. N. Engl. J. Med. 325: 147–152, 1991. Henriksen, E. J., K. J. Rodnick, and J. O. Holloszy. Activation of glucose transport in skeletal muscle by phospholipase C and phorbol ester. Evaluation of the regulatory roles of protein kinase C and calcium. J. Biol. Chem. 264: 21536–21543, 1989. Henriksen, E. J., K. J. Rodnick, C. E. Mondon, D. E. James, and J. O. Holloszy. Effect of denervation or unweighting on GLUT-4 protein in rat soleus muscle. J. Appl. Physiol. 70: 2322–2327, 1991. Henriksen, E. J., M. D. Sleeper, J. R. Zierath, and J. O. Holloszy. Polymyxin B inhibits stimulation of glucose transport in muscle by hypoxia or contractions. Am. J. Physiol. 256 (Endocrinol. Metab. 19): E662–E667, 1989. Hirshman, M. F., L. J. Goodyear, L. J. Wardzala, E. D. Horton, and E. S. Horton. Identification of an intracellular pool of glucose transporters from basal and insulin-stimulated rat skeletal muscle. J. Biol. Chem. 265: 987–991, 1990. Hirshman, M. F., H. Wallberg-Henriksson, L. J. Wardzala, E. D. Horton, and E. S. Horton. Acute exercise increases the number of plasma membrane glucose transporters in rat skeletal muscle. FEBS Lett. 238: 235–239, 1988. Holloszy, J. O., S. H. Constable, and D. A. Young. Activation of glucose transport in muscle by exercise. Diabetes Metab. Rev. 1: 409–424, 1986. Holloszy, J. O., and P. A. Hansen. Regulation of glucose transport into skeletal muscle. Rev. Physiol. Biochem. Pharmacol. 128: 99–193, 1996. Holloszy, J. O., and H. T. Narahara. Changes in permeability to 3-methylglucose associated with contraction of isolated frog muscle. J. Biol. Chem. 240: 3493–3500, 1965. Holloszy, J. O., and H. T. Narahara. Enhanced permeability to sugar associated with muscle contraction: studies of the role of Ca11. J. Gen. Physiol. 50: 551–562, 1967. Holman, G. D., I. J. Kozka, A. E. Clark, C. J. Flower, J. Saltis, A. D. Habberfield, I. A. Simpson, and S. W. Cushman. Cell surface labeling of glucose transporter isoform GLUT4 by bis-mannose photolabel. Correlation with stimulation of glucose transport in rat adipose cells by insulin and phorbol ester. J. Biol. Chem. 265: 18172–18179, 1990. Hong, D. H., J. Huan, B. R. Ou, J. Y. Yeh, T. C. Saido, P. R. Cheeke, and N. E. Forsberg. Protein kinase C isoforms in INVITED REVIEW 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. muscle cells and their regulation by phorbol ester and calpain. Biochim. Biophys. Acta 1267: 45–54, 1995. Ishizuka, T., D. R. Cooper, H. Hernandez, D. Buckley, M. Standaert, and R. V. Farese. Effects of insulin on diacylglycerol-protein kinase C signaling in rat diaphragm and soleus muscles and relationship to glucose transport. Diabetes 39: 181–190, 1990. Ivy, J. L., and J. O. Holloszy. Persistent increase in glucose uptake by rat skeletal muscle following exercise. Am. J. Physiol. 241 (Cell Physiol. 10): C200–C203, 1981. Kayano, T., C. F. Burant, H. Fukumoto, G. W. Gould, Y. Fan, R. L. Eddy, M. G. Byers, T. B. Shows, S. Seino, and G. I. Bell. Human facilitative glucose transporters. Isolation, functional characterization, and gene localization of cDNAs encoding an isoform (GLUT5) expressed in small intestine, kidney, muscle, and adipose tissue and an unusual glucose transporter pseudogene-like sequence (GLUT6). J. Biol. Chem. 265: 13276–13282, 1990. King, P. A., J. J. Betts, E. D. Horton, and E. S. Horton. Exercise, unlike insulin, promotes glucose transporter translocation in obese Zucker rat muscle. Am. J. Physiol. 265 (Regulatory Integrative Comp. Physiol. 34): R447–R452, 1993. King, P. A., M. F. Hirshman, E. D. Horton, and E. S. Horton. Glucose transport in skeletal muscle membrane vesicles from control and exercised rats. Am. J. Physiol. 257 (Cell Physiol. 26): C1128–C1134, 1989. King, P. A., E. D. Horton, M. F. Hirshman, and E. S. Horton. Insulin resistance in obese Zucker rat (fa/fa) skeletal muscle is associated with a failure of glucose transporter translocation. J. Clin. Invest. 90: 1568–1575, 1992. Klip, A., and M. R. Paquet. Glucose transport and glucose transporters in muscle and their metabolic regulation. Diabetes Care 13: 228–242, 1990. Klip, A., T. Ramlal, P. J. Bilan, G. D. Cartee, E. A. Gulve, and J. O. Holloszy. Recruitment of GLUT-4 glucose transporters by insulin in diabetic rat skeletal muscle. Biochem. Biophys. Res. Commun. 172: 728–736, 1990. Klip, A., T. Ramlal, D. Young, and J. O. Holloszy. Insulininduced translocation of glucose transporters in rat hindlimb muscles. FEBS Lett. 224: 224–230, 1987. Kristiansen, S., S. Asp, and E. A. Richter. Decreased muscle GLUT-4 and contraction-induced glucose transport after eccentric contractions. Am. J. Physiol. 271 (Regulatory Integrative Comp. Physiol. 40): R477–R482, 1996. Kristiansen, S., F. Darakhshan, E. A. Richter, and H. S. Hundal. Fructose transport and GLUT-5 protein in human sarcolemmal vesicles. Am. J. Physiol. 273 (Endocrinol. Metab. 36): E543–E548, 1997. Kristiansen, S., M. Hargreaves, and E. A. Richter. Exerciseinduced increase in glucose transport, GLUT-4, and VAMP-2 in plasma membrane from human muscle. Am. J. Physiol. 270 (Endocrinol. Metab. 33): E197–E201, 1996. Kristiansen, S., M. Hargreaves, and E. A. Richter. Progressive increase in glucose transport and GLUT-4 in human sarcolemmal vesicles during moderate exercise. Am. J. Physiol. 272 (Endocrinol. Metab. 35): E385–E389, 1997. Kubo, K., and J. E. Foley. Rate-limiting steps for insulinmediated glucose uptake into perfused rat hindlimb. Am. J. Physiol. 250 (Endocrinol. Metab. 13): E100–E102, 1986. Kusunoki, M., L. H. Storlien, J. MacDessi, N. D. Oakes, C. Kennedy, D. J. Chisholm, and E. W. Kraegen. Muscle glucose uptake during and after exercise is normal in insulinresistant rats. Am. J. Physiol. 264 (Endocrinol. Metab. 27): E167–E172, 1993. Langfort, J., L. Budohoski, H. Kaciuba Uscilko, K. Nazar, J. R. Challiss, and E. A. Newsholme. Effect of endurance and sprint exercise on the sensitivity of glucose metabolism to insulin in the epitrochlearis muscle of sedentary and trained rats. Eur. J. Appl. Physiol. Occup. Physiol. 62: 145–150, 1991. Lee, A. D., E. A. Gulve, M. Chen, J. Schluter, and J. O. Holloszy. Effects of Ca21 ionophore ionomycin on insulinstimulated and basal glucose transport in muscle. Am. J. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. E1049 Physiol. 268 (Regulatory Integrative Comp. Physiol. 37): R997– R1002, 1995. Lee, A. D., P. A. Hansen, and J. O. Holloszy. Wortmannin inhibits insulin-stimulated but not contraction-stimulated glucose transport activity in skeletal muscle. FEBS Lett. 361: 51–54, 1995. Le Marchand-Brustel, Y., N. Gautier, M. Cormont, and E. Van Obberghen. Wortmannin inhibits the action of insulin but not that of okadaic acid in skeletal muscle: comparison with fat cells. Endocrinology 136: 3564–3570, 1995. Lund, S., G. D. Holman, O. Schmitz, and O. Pedersen. Contraction stimulates translocation of glucose transporter GLUT4 in skeletal muscle through a mechanism distinct from that of insulin. Proc. Natl. Acad. Sci USA. 92: 5817–5821, 1995. Manson, J. E., D. M. Nathan, A. S. Krolewski, M. J. Stampfer, W. C. Willett, and C. H. Hennekens. A prospective study of exercise and incidence of diabetes among US male physicians. JAMA 268: 63–67, 1992. Manson, J. E., E. B. Rimm, M. J. Stampfer, G. A. Colditz, W. C. Willett, A. S. Krolewski, B. Rosner, C. H. Hennekens, and F. E. Speizer. Physical activity and incidence of noninsulin dependent diabetes mellitus in women. Lancet 338: 774–778, 1991. Marette, A., E. Burdett, A. Douen, M. Vranic, and A. Klip. Insulin induces the translocation of GLUT4 from a unique intracellular organelle to transverse tubules in rat skeletal muscle. Diabetes 41: 1562–1569, 1992. Martin, I. K., A. Katz, and J. Wahren. Splanchnic and muscle metabolism during exercise in NIDDM patients. Am. J. Physiol. 269 (Endocrinol. Metab. 32): E583–E590, 1995. Mastick, C. C., R. Aebersold, and G. E. Lienhard. Characterization of a major protein in GLUT4 vesicles. J. Biol. Chem. 269: 6089–6092, 1994. Mayfield, R. K., N. Shimojo, and A. A. Jaffa. Skeletal muscle kallikrein. Potential role in metabolic regulation. Diabetes 45, Suppl. 1: S20–S23, 1996. Mikines, K. J., B. Sonne, P. A. Farrell, B. Tronier, and H. Galbo. Effect of physical exercise on sensitivity and responsiveness to insulin in humans. Am. J. Physiol. 254 (Endocrinol. Metab. 17): E248–E259, 1988. Minuk, H. L., M. Vranic, E. B. Marliss, A. K. Hanna, A. M. Albisser, and B. Zinman. Glucoregulatory and metabolic response to exercise in obese non-insulin-dependent diabetes. Am. J. Physiol. 240 (Endocrinol. Metab. 3): E458–E464, 1981. Moxham, C. M., A. Tabrizchi, R. J. Davis, and C. C. Malbon. Jun N-terminal kinase mediates activation of skeletal muscle glycogen synthase by insulin in vivo. J. Biol. Chem. 271: 30765–30773, 1996. Murai, H., M. Okazaki, and A. Kikuchi. Tyrosine dephosphorylation of glycogen synthase kinase-3 is involved in its extracellular signal-dependent inactivation. FEBS Lett. 392: 153–160, 1996. Narahara, H. T., P. Ozand, and C. F. Cori. Studies of tissue permeability. VII. The effect of insulin on glucose penetration and phosphorylation in frog muscle. J. Biol. Chem. 235: 3370– 3378, 1960. Nesher, R., I. E. Karl, and D. M. Kipnis. Dissociation of effects of insulin and contraction on glucose transport in rat epitrochlearis muscle. Am. J. Physiol. 249 (Cell Physiol. 18): C226–C232, 1985. Nishimura, H., F. V. Pallardo, G. A. Seidner, S. Vannucci, I. A. Simpson, and M. J. Birnbaum. Kinetics of GLUT1 and GLUT4 glucose transporters expressed in Xenopus oocytes. J. Biol. Chem. 268: 8514–8520, 1993. Nolte, L. A., J. Rincon, E. O. Wahlstrom, B. W. Craig, J. R. Zierath, and H. Wallberg-Henriksson. Hyperglycemia activates glucose transport in rat skeletal muscle via Ca21dependent mechanism. Diabetes 44: 1345–1348, 1995. Pedersen, O., J. F. Bak, P. H. Andersen, S. Lund, D. E. Moller, J. S. Flier, and B. B. Kahn. Evidence against altered expression of GLUT1 or GLUT4 in skeletal muscle of patients with obesity or NIDDM. Diabetes 39: 865–870, 1990. E1050 INVITED REVIEW 91. Perseghin, G., T. B. Price, K. F. Petersen, M. Roden, G. W. Cline, K. Gerow, D. L. Rothman, and G. L. Shulman. Increased glucose transport-phosphorylation and muscle glycogen synthesis after exercise training in insulin-resistant subjects. N. Engl. J. Med. 335: 1357–1362, 1996. 92. Ploug, T., H. Galbo, and E. A. Richter. Increased muscle glucose uptake during contractions: no need for insulin. Am. J. Physiol. 247 (Endocrinol. Metab. 10): E726–E731, 1984. 93. Ploug, T., T. Ohkuwa, A. Handberg, J. Vissing, and H. Galbo. Effect of immobilization on glucose transport and glucose transporter expression in rat skeletal muscle. Am. J. Physiol. 268 (Endocrinol. Metab. 31): E980–E986, 1995. 94. Ploug, T., J. Wojtaszewski, S. Kristiansen, P. Hespel, H. Galbo, and E. A. Richter. Glucose transport and transporters in muscle giant vesicles: differential effects of insulin and contractions. Am. J. Physiol. 264 (Endocrinol. Metab. 27): E270–E278, 1993. 95. Richter, E. A. Glucose utilization. In: Handbook of Physiology. Exercise: Regulation and Integration of Multiple Systems. Bethesda, MD: Am. Physiol. Soc., 1996, sect. 12, chapt. 20, p. 912–951. 96. Richter, E. A., P. J. F. Cleland, S. Rattigan, and M. G. Clark. Contraction-associated translocation of protein kinase C in rat skeletal muscle. FEBS Lett. 217: 232–236, 1987. 97. Richter, E. A., L. P. Garetto, M. N. Goodman, and N. B. Ruderman. Muscle glucose metabolism following exercise in the rat: increased sensitivity to insulin. J. Clin. Invest. 69: 785–793, 1982. 98. Richter, E. A., L. P. Garetto, M. N. Goodman, and N. B. Ruderman. Enhanced muscle glucose metabolism after exercise: modulation by local factors. Am. J. Physiol. 246 (Endocrinol. Metab. 9): E476–E482, 1984. 99. Richter, E. A., K. J. Mikines, H. Galbo, and B. Kiens. Effect of exercise on insulin action in human skeletal muscle. J. Appl. Physiol. 66: 876–885, 1989. 100. Richter, E. A., T. Ploug, and H. Glabo. Increased muscle glucose uptake after exercise: no need for insulin during exercise. Diabetes 34: 1041–1048, 1985. 101. Rodnick, K. J., J. W. Slot, D. R. Studelska, D. E. Hanpeter, L. J. Robinson, H. J. Geuze, and D. E. James. Immunocytochemical and biochemical studies of GLUT4 in rat skeletal muscle. J. Biol. Chem. 267: 6278–6285, 1992. 102. Roy, D., and A. Marette. Exercise induces the translocation of GLUT4 to transverse tubules from an intracellular pool in rat skeletal muscle. Biochem. Biophys. Res. Commun. 223: 147– 152, 1996. 103. Ruderman, N. B., T. Balon, A. Zorzano, and M. Goodman. The postexercise state: altered effects of insulin on skeletal muscle and their physiologic relevance. Diabetes Metab. Rev. 1: 425–444, 1986. 104. Sadoshima, J., Y. Xu, H. S. Slayter, and S. Izumo. Autocrine release of angiotensin II mediates stretch-induced hypertrophy of cardiac myocytes in vitro. Cell 75: 977–984, 1993. 105. Schwartz, N. S., and J. E. McKenzie. Adenosine and active hyperemia in soleus and gracilis muscle of cats. Am. J. Physiol. 259 (Heart Circ. Physiol. 28): H1295–H1304, 1990. 106. Sherman, L. A., M. F. Hirshman, M. Cormont, Y. Le Marchand-Brustel, and L. J. Goodyear. Differential effects of insulin and exercise on Rab4 distribution in rat skeletal muscle. Endocrinology 137: 266–273, 1996. 107. Sherman, W. M., A. L. Katz, C. L. Cutler, R. T. Withers, and J. L. Ivy. Glucose transport: locus of muscle insulin resistance in obese Zucker rats. Am. J. Physiol. 255 (Endocrinol. Metab. 18): E374–E382, 1988. 108. Shibata, H., W. Omata, Y. Suzuki, T. Tankaka, and I. Kojima. A synthetic petide corresponding to the Rab4 hypervariable carboxyl-terminal domain inhibits insulin action on glucose transport in rat adipocytes. J Biol. Chem. 271: 9704–9709, 1996. 109. Simons, K., and M. Zerial. Rab proteins and the road maps for intracellular transport. Neuron 11: 789–799, 1993. 110. Sowell, M. O., M. K. Treutelaar, C. F. Burant, and M. G. Buse. Minimal effects of phorbol esters on glucose transport 111. 112. 113. 114. 115. 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. 126. 127. 128. and insulin sensitivity of rat skeletal muscle. Diabetes 37: 499–506, 1988. Stephens, J. M., and P. F. Pilch. The metabolic regulation and vesicular transport of GLUT4, the major insulin-responsive glucose transporter. Endocr. Rev. 16: 529–546, 1995. Sternlicht, E., R. J. Barnard, and G. K. Grimditch. Mechanism of insulin action on glucose transport in rat skeletal muscle. Am. J. Physiol. 254 (Endocrinol. Metab. 17): E633– E638, 1988. Sternlicht, E., R. J. Barnard, and G. K. Grimditch. Exercise and insulin stimulate skeletal muscle glucose transport through different mechanisms. Am. J. Physiol. 256 (Endocrinol. Metab. 19): E227–E230, 1989. Suzuki, K., and T. Kono. Evidence that insulin causes translocation of glucose transport activity to the plasma membrane from an intracellular storage site. Proc. Natl. Acad. Sci. USA 77: 2542–2545, 1980. Treadway, J. L., D. E. James, E. Burcel, and N. B. Ruderman. Effect of exercise on insulin receptor binding and kinase activity in skeletal muscle. Am. J. Physiol. 256 (Endocrinol. Metab. 19): E138–E144, 1989. Turinsky, J. Glucose and amino acid uptake by exercising muscles in vivo: effect of insulin, fiber population, and denervation. Endocrinology 121: 528–535, 1987. Vandenburgh, H. H. Mechanical forces and their second messengers in stimulating cell growth in vitro. Am. J. Physiol. 262 (Regulatory Integrative Comp. Physiol. 31): R350–R355, 1992. Van der Sluijs, P., M. Hull, L. A. Huber, P. Male, B. Goud, and I. Mellman. Reversible phosphorylation-dephosphorylation determines the localization of rab4 during the cell cycle. EMBO J. 11: 4379–4389, 1992. Vergauwen, L., P. Hespel, and E. A. Richter. Adenosine receptors mediate synergistic stimulation of glucose uptake and transport by insulin and by contractions in rat skeletal muscle. J. Clin. Invest. 93: 974–981, 1994. Vissing, J., T. Ohkuwa, T. Ploug, and H. Galbo. Effect of prior immobilization on muscular glucose clearance in resting and running rats. Am. J. Physiol. 255 (Endocrinol. Metab. 18): E456–E462, 1988. Volchuk, A., Y. Mitsumoto, L. He, Z. Liu, E. Habermann, W. Trimble, and A. Klip. Expression of vesicle-associated membrane protein 2 (VAMP-2)/synaptobrevin II and cellubrevin in rat skeletal muscle and in a muscle cell line. Biochem. J. 304: 139–145, 1994. Vranic, M., D. Wasserman, and L. Bukowiecki. Metabolic implications of exercise and physical fitness in physiology and diabetes. In: Diabetes Mellitus: Theory and Practice, edited by H. Rifkin and D. Porte. New York: Elsevier, 1990, p. 198–219. Wallberg-Henriksson, H., S. H. Constable, D. A. Young, and J. O. Holloszy. Glucose transport into rat skeletal muscle: interaction between exercise and insulin. J. Appl. Physiol. 65: 909–913, 1988. Wallberg-Henriksson, H., and J. O. Holloszy. Activation of glucose transport in diabetic muscle: responses to contraction and insulin. Am. J. Physiol. 249 (Cell Physiol. 18): C233–C237, 1985. Wilson, C. M., and S. W. Cushman. Insulin stimulation of glucose transport activity in rat skeletal muscle: increase in cell surface GLUT4 as assessed by photolabelling. Biochem. J. 299: 755–759, 1994. Wojtaszewski, J. F. P., B. F. Hansen, B. Kiens, and E. A. Richter. Insulin signaling in human skeletal muscle: time course and effect of exercise. Diabetes. In press. Wojtaszewski, J. F. P., B. F. Hansen, B. Ursø, and E. A. Richter. Wortmannin inhibits both insulin- and contractionstimulated glucose uptake and transport in rat skeletal muscle. J. Appl. Physiol. 81: 1501–1509, 1996. Yamada, K., A. Avignon, M. L. Standaert, D. R. Cooper, B. Spencer, and R. V. Farese. Effects of insulin on the translocation of protein kinase C-u and other protein kinase C isoforms in rat skeletal muscles. Biochem. J. 308: 177–180, 1995. INVITED REVIEW 129. Yeh, J. I., E. A. Gulve, L. Rameh, and M. J. Birnbaum. The effects of wortmannin on rat skeletal muscle. Dissociation of signaling pathways for insulin- and contraction-activated hexose transport. J. Biol. Chem. 270: 2107–2111, 1995. 130. Youn, J. H., E. A. Gulve, and J. O. Holloszy. Calcium stimulates glucose transport in skeletal muscle by a pathway independent of contraction. Am. J. Physiol. 260 (Cell Physiol. 29): C555–C561, 1991. 131. Young, J. C., T. G. Kurowski, A. M. Maurice, R. Nesher, and N. B. Ruderman. Polymyxin B inhibits contractionstimulated glucose uptake in rat skeletal muscle. J. Appl. Physiol. 70: 1650–1654, 1991. E1051 132. Young, M. E., G. K. Radda, and B. Leighton. Nitric oxide stimulates glucose transport and metabolism in rat skeletal muscle in vitro. Biochem. J. 322: 223–228, 1997. 133. Zorzano, A., T. W. Balon, L. P. Garetto, M. N. Goodman, and N. B. Ruderman. Muscle a-aminoisobutyric acid transport after exercise: enhanced stimulation by insulin. Am. J. Physiol. 248 (Endocrinol. Metab. 11): E546–E552, 1985. 134. Zorzano, A., T. W. Balon, M. N. Goodman, and N. B. Ruderman. Additive effects of prior exercise and insulin on glucose and AIB uptake by rat muscle. Am. J. Physiol. 251 (Endocrinol. Metab. 14): E21–E26, 1986.