Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
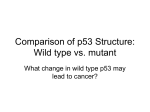
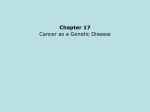
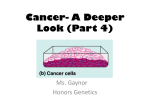
From www.bloodjournal.org by guest on June 18, 2017. For personal use only. Nonhereditary p53 Mutations in T-cell Acute Lymphoblastic Leukemia Are Associated With the Relapse Phase By Michael H. Hsiao, Alice L. Yu, Jo Yeargin, David Ku, and Martin Haas We have previously reported that greater than 60% of human leukemic T-cell lines possess mutations in the p53 tumor suppressor gene. To determine whether T-cell acute lymphoblastic leukemia (T-ALL) patient samples possess p53 mutations, we screened peripheral blood- and bone marrow-derived leukemia samples, taken at diagnosis and at relapse, for p53 mutations. Exons 4 through 9 and selected intron regions of the p53 gene were analyzed using polymerase chain reaction-single-strandconformation polymorphism and direct sequencing. p53 mutations were found in 0 of 15 T-ALL diagnosis samples, as compared with 10 of 36 (28Y0)T-ALL relapse samples. To determine whether p53 mutations play a role in the recurrence (relapse) of T-ALL, t w o special groups of T-ALL patients were studied: (1) a group of 8 relapse patients whosedisease was refractoryt o chemotherapeutic treatment, and (2) a group of 6 "paired" T-ALL cell samples from patients for whom we possess both diagnosis and relapse samples. Three of 8 relapsed patients (37.5Y0) whose disease was refractory t o the reinduction of remission by chemotherapy possessed missense mutations of the p53 gene. All 3 caseshad mutationsin exon 5. Among the paired samples, 3 of 6 patients harbored p53 mutations at disease recurrence, but possessed only wild-type p53 alleles at diagnosis. One case had mutation onexon 4, l case in exon 5, and 1 case in exon 8 with loss of heterozygosity. These data clearly indicate that recurrence of T-ALL is associated with missense mutations in p53. Our results indicate that (1) mutations of p53 do occur in T-ALL in vivo, and such mutations are associated with the relapse phase of the disease; and (2) p53 mutation isinvolved in the progression of T-ALL. This conclusion is supported by our observation that the introduction of T-ALL-derived mutant p53 expression constructs into T-ALL cell lines further increases their growth rate in culture, enhances cell cloning in methylcellulose, and increases tumor formation in nude mice. 0 1994 by The American Societyof Hematology. P have also. been found in the precancerous phasesof adenocarcinomas and in adenomatous polypsof patients with familial polyposis coli,2zsuggesting that p53 mutation may occur as an early event in carcinogenesis as well. In our studies on the role of p53 in the pathogenesis of human T-cell acute lymphoblastic leukemia (T-ALL), we have shown that greater than 60% of T-ALL cell lines, all of which had been grownfrom relapse T-ALL cases, possess mutations on both p53 suggesting that p53 serves a critical role in the generation of the fully tumorigenic leukemic T cells. However, our experiments did not show whether these p53 mutations originated in vivo or whether the p53 gene had been mutated during cell line establishment in vitro, as has been shown to occur during the establishment of some rat embryo fibroblast cell lines.24Gaidano et alZs and Jonveaux and BergerZ6have reported that samples from T-ALL patients obtained at diagnosis harbor no mutations in the p53 gene. In all, these two groups studied 37 T-ALL diagnosis samples, all of which possessed only wild-type p53 alleles. Recently, we reported that T-ALL cell lines established in our laboratory from a patient sample taken at relapse possess the same p53 mutation found in the in vivo sample." Furthermore, no additional mutations of p53 OCcurred during establishment of the cell lines. These results suggest that the establishment of human T-ALL cell lines need not be associated with the induction of p53 mutations. To studywhether p53 mutations may be differentially associated with the relapse versus diagnosis phases of TALL, we used polymerase chain reaction-single-strand conformation polymorphism (PCR-SSCP)*' and direct sequencing of PCR-amplified fragments to study 15 cases of T-ALL at diagnosis and 36 cases at relapse. The results suggest that, in the patients studied, mutation of the p53 gene was associated with the clonal evolution that takes place during recurrence of the disease. 53 BELONGS TO THE tumor suppressor class of genes whose function involves the negative regulation of cell growth. The loss of function of the p53 gene by deletion, mutation, or rearrangement may contribute to the genesis or progression of a wide variety of human cancers.',' Abnormalities in the p53 gene have been demonstrated in human carcinoma of the colorectum,3 l i ~ e r , bladder,8 ~.~ and ovary'; in blast crisis chronic myelogenous and myelocytic leukemias'",''; in progressed adult T-cell le~kemia".'~;and in osteogenic sarcoma^.'^^'^ Several lines of evidence suggest that p53 mutatioddeletion is a late event in the development of cancer, because (1) in carcinomas of the colorectum, chromosome 17p deletions are associated with the transition from benign adenoma to malignant carcinoma'6;( 2 ) the progression of brain tumors is associated witha clonal expansion of cells that have acquireda mutation in thep53 gene17;(3) the evolution of chronic-phase chronic myelogenous leukemia (CML) to myeloid blast crisis18-*"is associated with mutation of the p53 gene; and (4)the mutation of p53 and the lossof heterozygosity of chromosome 17pand 10 areassociatedwiththe progression of astrocytomas."However,mutationsin p53 From the Department of Biology/Cancer Center, and the Department of Pediatrics, University of California, San Diego, La Jolla, CA. Submitted September 10, 1993; accepted January 7, 1994. Supported in part by grants from the US Department of Energy (DE-FG03-91 ER611 71), the American Cancer Society (CH456), and the National Cancer Institute, National Institutes of Health (ROICA56075 and UIOCA28439 [to A.L.Y.]), US Department of Health, Education, and Welfare. Address reprint requests to Martin Haas,MD, Department of Biology, UCSD Cancer Center, 0063, University of California, San Diego, 9500 Gilman Dr, La Jolla, CA 92093-0063. The publication costsof this article were defrayedin part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section I734 solely to indicate this fact. 0 1994 by The American Society of Hematology. 0006-4971/94/8310-0015$3.00/0 2922 MATERIALSAND METHODS T-ALL patient samples. Peripheral blood or bone marrow cells from 51 T-ALL patients at diagnosis or at relapse were donated in Blood, Vol 83, No 10 (May 15), 1994: pp 29222930 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 2923 p53 MUTATIONS IN RELAPSEACUTE T LEUKEMIA accordance with a protocol approved by the Committee on Investigation Involving Human Subjects at the University of California, San Diego. Some samples were kindly provided by the tumor cell bank of the Pediatric Oncology Group at St Jude’s Children’s Research Hospital. Peripheral blood or bone marrow cells were collected for the purpose of routine clinical diagnosis, and cells that remained after the diagnostic procedures were frozen live in liquid nitrogen for future use. High molecular weight DNA was extracted from one ampoule (IO7 cells) of each frozen T-ALL patient sample. SSCP ana!\sis. SSCP analysis was adaptedfromthe original SSCP method of Orita et al.” Briefly, 1 0 0 ng of genomic DNA was usedin a PCRamplification.Eachreactionmixturecontained in addition to genomic DNA, 10 pm01 of each primer, 2.5 pmol/L dNTPs, I pCi of [a-”P]dCTP (Amersham; specific activity, 3,000 Ci/mmol; 1 Ci = 37 GBq), 10 mmol/L Tris-HC1 (pH 8.8). 50 mmol/ L KCI, 1 mmoVL MgCI2,0.01% gelatin, and 0.5 U of Taq polymerase, in a final volume of 10 pL. Thirty cycles of denaturation (93°C for 2 minutes), annealing (60°C for exons 4, 5, 6, and 8: 68°C for exon 7; 51°C for exon 9: for 2 minutes), and extension (72°C for 1 minute) were performed. Two microliters of the reaction mixture was diluted 25Xin 0.1% sodium dodecyl sulfate (SDS)/IO mmol/L EDTA and further mixed I: I with a sequencing stop solution containing 20 mmoll L NaOH. Samples were heated to 95°C for 5 minutes and chilled on ice, and 3 pL was immediately loaded onto the gel. Gels were run at 4 W for 16 to 20 hours at room temperature. Autoradiography was performed with an intensifying screen for 6 to 24 hours. Because not all of the mutation bands were easily separated from normal germline bands with good resolution using one gel condition. three gel conditions were used for each sample: (1) 6% acrylamide with 10% (voll vol) glycerol (better separation with poor resolution): (2) 4% MDE (AT Biochem, Malvern. PA) with glycerol (intermediate separation and resolution); and (3) 4% MDE without glycerol (best resolution withleast separation). Mobility shifts that were detected by SSCP were confirmed underatleast two different gel conditions, before sequencing. The following p53 amplification primers were used? MH41 (5‘ exon 4 primer), 5’-ATCTACAGTCCCCCTTGCCG-3’; MH42 (3‘ exon 4 primer), 5‘-GCAACTGACCGTGCAAGTCA-3‘; MH22 (5‘ MH20 (3’ exon 5 primer), 5’-CTGTTCACTTGTGCCCTGAC-3‘; exon 5 primer), 5’-CAACCAGCCCTGTCGTCTCT-3’; MH28 (5’ exon 6 primer), 5‘-GAGACGACAGGGCTGGTT-3’; MH29 (3‘ exon 6 primer), 5’-CCACTGACAACCACCCTT-3‘; MH30 (5‘ exon 7 primer), 5‘-CCAAGGCGCACTGGCCTC-3’: MH3I (3’ exon 7 primer), 5‘-GAGGCAAGCAGAGGCTGG-3’; MH 19 (5‘ exon 8 primer), 5’-GGGACAGGTAGGACCTGATT-3‘; MH23 (3’ exon 8 primer), 5’-CACCGCTTCTTGTCCTGCTT-3’; MH34 (5‘ exon 9 primer), 5‘”ITATGCCTCAGATTCACTTTT-3’; MH25 (3’ exon 9 primer), 5’-CATCGAATTCTGGAAACTTTCCACTTGAT-3”. Direct sequencing of PCR products. Samples that were found by SSCP analysis to possess p53 mutations were sequenced to identify the nature of the mutation. Solid-phase sequencing of in vitro amplified genomic DNA was in which genomic DNA was amplified by PCR using biotinylated primers (Operon, Almeda, CA). One microgram of genomic DNA was used as template in a 100 pL PCR reaction with 12 pm01of biotinylated primer and 36 pm01 of nonbiotinylated primer. Forty microliters of this reaction was incubated with magnetic beads conjugated covalently with streptavidin (Dynabeads M280-streptavidin: Dynal, Oslo, Norway) that were used to selectively immobilize the biotin-labeled PCR product and allow melting of the DNA duplex, followed by elution of the nonlabeled single strand. The immobilized single-strand DNA was then used as sequencing template using the Sequenase (US Biochemical CO, Cleveland, OH) protocol and an internal primer. RESULTS p53 mutation is a frequent genetic change in relapse ALL T- We used PCR-SSCP analysis to screen for p53 muta- Exon 5 Exon 4 P L P L A C A C E N C H A F O T E A S A N A M N N N N E N S T M A N ri6 P L A C E C N F G E T M C M A N N U yI1 W h Yr Fig 1. PCR-SSCP analysis of p53 mutations in T-ALL patient M m ples. Human placenta DNA was used as normal control. DNA extracted from thecell line CEM was used as a positive control for exon 5. Gel conditions: exon 4,6% acrylamide gel with 10% glycerol; exon 5 (left panel), 4% MDE gel; exon 5 (right panell, 6% acrylarnide gel with 10% glycerol. Note that 6% acrylamide gel with 10% glycerol provides the best separation but poor resolution. 4% MDE gel without glycerol provides the best resolution with least single-strand band separation. tions in the genomic DNAof 51 patients with childhood acute lymphoblastic leukemia at different clinical stages (15 diagnosis T-ALL, 36 relapse T-ALL). Significant electrophoretic mobility shifts were detected in 10 of the 36 relapse T-ALL samples (28%),and in none (0 of 15) of the diagnosis T-ALL samples (0%). Figure 1 shows examples ofPCRSSCP analyses of exons 4 and 5 . DNA extracted from a normal human placenta was used as normal control to show the germline bands. The T-ALL cell line CEM, which harbors a mutation in p53 codon 175,*” was used as a mutant control of exon 5 to show different mobility shift patterns under two different gel conditions (see legend to Fig 1 and Materials and Methods). Direct sequence analysis was performed onthe 10 samples found to be positive for p53 mutations based on significant SSCP shifts. Mostof the mutations foundweremissense mutations with single-base changes thatencoded single amino acid substitutions in the p53 protein (Table 1). The majority of the mutations found are located in exon 5. One patient, PJN, had an intron 4 mutation. Although its biologic significance has not been studied further, its detection shows that cells harboring this mutation were selected for; hence, From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 2924 HSlAO ET AL Table 1. Frequency and Nature of p53 Mutations in Primary l-ALL Samples Identification of Mutation T-ALL Patient Sample SSCP Codon Seq Change Genotype aa Change % Blasts Diagnosis 0/15 (0%) Relapse 10/36 (28%) SMN FAN ONN ASN GCN SRN FMN HAN BTN PJN Ex 4 110 Ex 5 135 Ex 5 135 Ex 5 135 Ex 5 141 Ex 5 161 Ex 5 167 170 Ex 5 175 Ex 8 282 ln4$ CGT TGC TGC TGC TGC GCC CAG ACG CGC CGG C-T - ClT -- AGC -- AGC TAC TC -- lACC CGG - ATG - GGC - GGG Arg Cys Cys Cys Cys Ala Gln Thr Arg Arg -- - --- Heterozygous Heterozygous Heterozygous Homozygous" Heterozygous Heterozygous Leu Ser Ser Tyr Phe Thr Arg Met Gly Gly Homozygous" Heterozygous Homozygoust 95 92 90 91 90 93 Wild-type allele at this locus undetectable on sequencing gel, but no LOH by codon 72 polymorphism (see Fig 7). t Homozygous mutation verified by LOH determination (see Fig 7). * C - T mutation occurs in intron 4 at position 13049 (Ref: Genebank sequence accession no. X54156). this intronic mutation may possess biologic significance. Figures 2 and 3 showrepresentativeexamples of thedirect sequencing data. Figure2 demonstrates two relapse T-ALL samples (GCN and HAN, respectively) with heterozygous missense mutations in exon 5. Interestingly, three separate cases possess mutations at codon 135. Two of these cases (FAN and ONN) possess a heterozygous mutation with nucleotide changefrom TGC to A/TGC ( 13YY6"?, whereas a homozygous mutation with nucleotide change from TGC TAC ( 13YYs "3 was found in the peripheral blood-derived leukemic cells of patient ASN (Fig 3). The apparent heterozygous nature of the mutations summarized in Table 1 may be caused by contamination of the leukemia samples with normal cells. Table 1 shows that at the time of DNA extraction the percent blast cells present in the patients' cell samples was at least 90%.The minority (wild-type) alleles detected could not have been caused by contamination with normal cells at the less than 10% level, - because in a mixture of mutant and wild-type DNA molecules the minority component is detectable on SSCP or sequencing gels only when present at 20% the level or higher.'" Hence, we conclude that the heterozygous natureof the mutations presented in Table 1 and in the corresponding figures representmutations in oneallele of theleukemiacells, whereas the other allele remains wild-type. To verify this conclusion, we have tested whether unrearranged (ie, germline) T-cell receptor (TCR) @-chainDNA could be demonto stratedinthesamplestested.Southernblotscontaining BumHI-digestedgenomicT-ALLDNAwerehybridized with a probe specific for the human T@ locus. All 6 samples showed rearranged TCR@ bands, whereas in only one (ONN) patient sample could a band of apparent germline size be shown (data not shown). Hence, the p53 mutations shown in Table 1 represent bona fide heterozygous mutations that are not caused by contamination of the leukemia cell samples with normal cells. EXON 5 PLACENTA GCN C T ACGT A G PLACENTA C T A G HAN C T A G c\ G T f I I * CODON 141 CODON 175 Fig 2. DNA sequence identification of exon 5 mutations detected by SSCP. Shown are codon 141 and 175 heterozygous mutations. Human placenta DNA sewves as normal control. From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 2925 p53 MUTATIONS IN RELAPSEACUTE T LEUKEMIA EXON 5 PLACENTA ASN Fig 3. Verificationofmutations in exon 5 that were found by SSCP analysis. Shown are three codon 135 mutations in T-ALL patient samples ASN, ONN, and FAN, as determined by directsequencing of PCR-amplified DNA. Patient ASN was homozygous for the mutation; patient samples ONN and FAN possess the same heterozygous mutations. CODON 135 p53 mutation i s somatically acquired and is associated with the recurrence of T-ALL. Ten of 36 relapse T-ALL cases studied (28%) possess p53 mutations in the p53 gene. Because these are random T-ALL patient samples collected during a 5-year period. there is no means of determining whether the mutations found are germline or somatically acquired, nor what role, if any, p53 mutations play in the recurrence of T-ALL. To determine the pathologic significance of p53 mutations in the recurrence (relapse) of TALL, a group of 6 "paired" T-ALL cell samples from patients for whom we possess both diagnosis and relapse samples were studied. PCR-SSCP and direct sequencing showed that none of the samples taken at diagnosis possessed p53 mutations, whereas 3 of 6 (50%) of the "paired" T-ALL samples studied harbored missense mutations at the relapse phase of the disease (Table 2). Figure 4 shows that a mutation was present in the leukemic cells of patient SMN at relapse. This mutation was absent from SMN's leukemic cells at diagnosis. PCR-direct sequencing data identify the nature of this mutation as a heterozygous missense mutation with a nucleotide change from CGT to CTT ( 1 IOArE+ Leu). A heterozygous missense mutation with a nucleotide change from GCC to ACC (161"" was found in the leukemic cells of patient SRN at relapse but not at diagnosis (Fig 5). Furthermore, a homozygous missense mutation was detected in the leukemic cells of patient BTN at relapse but not at diagnosis. Figure 6 shows this mutation as found by SSCP (arrow). Direct sequencing data establish the nucleotide change at relapse, a codon change from CGG to GGG (282Arg "ly). We also studied whether p53 mutations were present in the cells of a group of 8 T-ALL relapse patients whose - - Table 2. p53 Mutations in Paired Diagnosis/Relapse T-ALL Patient Samples Identification of Mutation SSCP (exon1 Patient AHNlD AHNIR BTNID BTNIR LMNID LMNIR SZNID SZN/R SRNID SR NIR SMNID SMNm 4 5 6 7 Sequencing 8 I + + 9 Codon Sequence 282 CGG - GGG 161 GCC - ACC 110 CGT - ClT Abbreviations: /D, patient sample obtained at diagnosis; /R, patient sample obtained at relapse. Homozygouslheterozygous mutations, genotype verified by codon 72 polymorphism (see Fig 7). aa Change Arg - Gly - Thr Arg - Leu Ala Genotype' Homozygous Heterozygous Heterozygous From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 2926 HSIAO ET AL Exon 4 P L A C E N T A/ B T N D/ B T N R/ L M N D/ L M N R/ S M N D/ S M N R/ A H N D/ A H N R Fig 4. Identificationand localization of mutations in exon SMN/D G A T C P v l c r - Y L - SMN/R G A T C =x, - " " --=S" ~ r T, = -= r -/cT UT\ CODON 110 diseasewasrefractorytochemotherapeutictreatment.30.3' p53 exons 4 through 9 were screened for mutations using PCR-SSCPanddirectsequencing.Threeof 8 patients (37.5%) in this group possess p53 mutations as detectedby PCR-SSCP. The p53 mutations in the groupof refractory TALL cases all mapped to exon 5. Direct sequencing showed a homozygous missense mutation in codon 135 witha nucleotide change from TGC to TAC (135cys'Ty? in patient ASN (Table 3). Leukemic cells of patients SRN andHANharbored heterozygous missense mutations in codon 161 (GCC to ACC,161 A'r ' and in codon175(CGCtoGGC, 175Arg'C'y), respectively (Table 3). Taken together, the presence of p53 mutations in 33%to 50% of relapse T-ALL cells in the different groups of patient samples studied suggests that p53 gene mutation is associated with the tumorigenic progression of relapse T-ALL cells. - 4. in "paired" diagnosislrelapse T-ALL samples, and verification of the mutation in codon 110 in patient SMN at relapse by direct sequencing of PCR-amplifiedgenomic DNA. DNA extracted from e human normal placenta was used as control. Gel conditions for SSCP analysis: 6% acrylamide gel with 10% glycerol. /D and /R refer t o DNA samples extracted the from T-ALL cells of same patients at diagnosis and at relapse, respectively. c Loss of heterozygosity at the p53 locus is an infrequent event in relapse T-ALL.. In human solid tumors, mutations of the p53 gene are frequently accompanied by the loss of heterozygosity of chromosome 17~13.1,the locus to which thep53genemaps.Wehavepreviouslyreportedthat, in leukemia cell lines, both alleles of the p53 gene were often independently mutated without concomitant loss of heterozygosity at the 17~13.1locus. To investigate whether loss of heterozygosity of p53 is a frequent event during recurrence of T-ALL, we used the known polymorphism at codon 72 the human of p53 This polymorphism enis coded by sequences in exon 4 of the p53 gene.The frequency of the 72"9- and the 72P"-encoding alleles (CGC and CCC, respectively) in the human population is 0.68 and 0.32, respectively.36 Thus,44% of the human population are heterozygous at this locus, whereas 46% and 10%encode homozy- Exon 5 P Fig 5. Identificationand localization of mutations in exon 5, in "paired" diagnosislrelapse T-ALL samples, and verification of the mutationin codon 161 in patient SRN at relapse by direct sequencing of PCR-amplified genomic DNA. DNA extracted from a normalhuman placenta and DNA extracted from CEM cells were used as normal and mutant controls in SSCP analysis. Gel condition for SSCP 4% MDE gel with 10% glycerol. L A C E S N C Z T E N A M D S Z N ~ A H N D A B B S S H T T R R N N N N N ~ D / R D I R SRN/D SRNm G A TGCA T C C C GA CODON 161 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. p53 MUTATIONS ACUTE IN RELAPSE 2927 T LEUKEMIA EXON 8 H T B 2 G Fig 6. SSCP analysis and direct sequencing of mutations in exon 8 of ”paired” diagnosislrelapse T-ALL samples. Human placenta DNA was used asa normal control (not shown) and DNA extracted from the breast carcinoma line MDA-MB-231 (HTB-26),“ which carries a mutation in p53 exon 8, was used as a positive control for SSCP. Gel condition for SSCP:4% MDE gel. B T N ~ B T N R A H N ~ A H N R L L S M M Z N N N I D R I ’,,LamL4U S Z N D S R N R S R N I S M N D S M N R I DGATC R m . m””. ”WvomqUBB, “ ” - ” . - m GATC I d - .. L+* CODON 282 gous (arg/arg)- or homozygous(pro/pro)-containingp53 relapse T-ALL patients, frequently harbor mutations in the proteins, respectively. p53 gene.23In contrast, T-ALL patient samples have been We applied PCR-SSCP analysis of exon 4 to determine r e p ~ r t e d ~to ’ . lack ~ ~ such mutations. This suggested that p53 in “paired” diagnosis the polymorphic status at codon 72 mutations that are foundin cell linesmay have been induced and relapse leukemia samples taken from the same patients. during in vitro establishmentof the lines. However, in vitro Five of the 6 “paired” leukemia samples were heterozygous mutation of p53 during the establishment of acute leukemia at codon 72 (4 of these are shown in Fig 7), whereas 1 of cell lines seemed unlikely because we have found in other the 6 “paired” patient samples,LMN, showed the homozyexperiments that, during establishment of multiple T-ALL gous arg/arg genotype at this position (Fig 7). Only1 of the cell lines, the p53 gene remained stably unaltered when com3 leukemia cases that harbored a p53 mutation at relapse pared with its state in the patients’ leukemia cells.27 This (Table 2), patientBTN,also underwent loss of heterozygosin thecurrentexperimentsby discrepancywasresolved ity upon leukemia relapse, by losing the arg-encoding p53 screening 15 untreated (“diagnosis”) and 36 recurrent (“reallele. As can be seen, the band of the amplified 72P”’-encod-lapse”) T-ALL cases, 12 of which were donated, pairwise, ingallelesofpatient BTN’s relapsesampleis of double bythesamepatientsatthediagnosisandattherelapse intensity compared with the cases that were heterozygous at phases of their disease. this codon. The status of codon 72 in the alleles carried by Among the 15 diagnosis T-ALL cases studied here, none the leukemia cell lines MOLT-4 (arg/arg) and CEM (arg/ possess p53 mutations in exons 4 through 9. Adding these pro), which we have previously shown by immunoprecipita- 15 diagnosis cases to those reported by a total of tion to harbor alleles encoding homozygous (arg/arg) and 52 diagnosis T-ALL cases have now been reported to lack heterozygous(arg/pro)p53proteins,respectively,” are p53 mutations, supporting the notion that mutation of the shown as internal controls. Subsequent DNA sequencing has p53 gene is not a causal event in the induction of childhood shown that the arginine allele was indeed lost during the T-ALL. In contrast to diagnosis T-ALL cases, among 36 recurrence (relapse)of disease in patient BTN (Fig 7, right). relapse cases studied, 10 (28%) harbored mutations in the p53 gene. Most(9 of 10)of these mutant p53 alleles specified DISCUSSION missense mutations that gave rise to nonconservative amino Wehave previously shown that acute lymphoblastic Tacid exchanges, whereas1 occurred in intron 4. The majority cellleukemiacelllines,all ofwhichwerederivedfrom of these mutations were mapped to the highly conserved, TTable 3. p53 Mutation inT-ALL Cases Refractoryto Chemotherapy Identification of Mutation SSCP (exon) Patient ASN CJN GENt HAN HJN HMN JRN SRN 4 5 + 6 Change 7 Sequencing 8a8 Change 9 Sequence Codon TGC135 CysTAC - Homozygous Tyr CGC175 -ArgGGC Heterozygous Gly 161 Ala GCC - - ACCHeterozygous - Thr HomozygouJheterozygous mutations, verified by status of codon72 polymorphism. t This patient‘s leukemia was refractow to chemotherapy, but relapse was not formally established. Genotype* From www.bloodjournal.org by guest on June 18, 2017. For personal use only. HSlAO ET AL 2928 Exon 4 M B B L C T T T E N N 4 M I D I R I 0 A H N D / A H N R I L M N D / L M N R I S R N D / S R N R / S Z N D / S Z N R BTNlD CTAG m CTAG CODON 72 antigen binding region of the p53 protein,3*suggesting that the mutations were biologically significant by conveying a selective growth advantage to the cells so endowed. In recent work (M. Hsiao. E. Dorn, J. Yeargin, and M. Haas, manuscript submitted), we have observed that mutated p53 genes thathadbeen cloned from relapse T-ALL cells and constructed into retroviral expression vectors indeed possess dominant oncogenic activity whenintroduced into T-ALL cells, as assayed by in vitro and in vivo criteria. Thus, p53 mutations in relapse T-ALL cells most probably play a biologically significant role in the disease. The lack of p53 mutations in any of the "diagnosis" samples suggests, but does not prove beyond a reasonable doubt, that mutation of the p53 gene in relapse samples is specifically associated with the progression of the leukemic phenotype. To prove that p53 mutations in relapse leukemia represent clonal evolution events, we compared the status of the p53 gene in diagnosis and in relapse samples in a pairwise fashion. Six pairs of leukemia cell samples, each derived from the same patients at different points in the clinical course, were studied for the status of the p53 gene. All six diagnosis samples lacked detectable p53 mutations in exons 4 through 9, whereas in 3 of the 6 relapse samples (50%)a mutation had occurred in the p53 gene (Table 2 ) . Clearly, p53 mutation is associated with the clonal evolution of relapse leukemia in a significant fraction of cases. This result supports our previous finding that a significant fraction of acute leukemia cell lines, all derived from relapse cases, possess mutations in the p53 gene. In some human solid tumors mutation of one p53 allele is often accompanied by the loss of the other p53 However, in acute leukemia cell lines loss of heterozygosity is an infrequent finding:3 and in the acute leukemia patient samples reported here, only 1 patient (BTN) among the 47 evaluable polymorphic cases displayed loss of heterozygosity of the p53 locus, as determined by the status of the polymorphic marker at codon 72. Although in greater than 50% of acute leukemia cell lines each p53 allele carried an independent mutation, in the current set of patient samples only 1 relapse case possessed two independent mutations Fig 7. Detection of allelic loss at the p53 locus in "paired" diagnosislrelapse patient samples by SSCP analysis of the polymorphic marker at codon 72. Cell linesMOLT4 and CEMwere usedascontrols. MOLT-4 cells are homozygous I~odon72'~'"~). whereas CEM cells are heterozygous172"g/72p") for thispolymorphic marker?' The leukemic cells of patient BTN were observed to undergo loss of heterozygosity at the p53locus (left panel), which was verified by direct sequencing(right panel).Gel conditionsfor SSCP: 4% MD€ gel. (FMN,Table 1). These two mutations occurred on the same allele, as determined by molecular cloning (not shown). This discrepancy between leukemia cell lines and patient relapse samples suggests either that relapse leukemia cells possessing independent mutations in both alleles are favored during establishment in vitro, or that, in the lines, the second allele became mutated upon establishment. Because the failure of chemotherapeutic treatment of acute childhood leukemia is often caused by the development of a drug-resistant clone, acute leukemias of patients who are refractory to the induction of remission might possess mutated p53 genes, as suggested by work of Cabanillas et 81'" and Chin et aL3' To test the possible correlation between refractoriness toremission induction and p53 mutation in acute T-cell leukemia, we tested a set of 8 refractory cases for the status of p53. Three of the 8 cases (37%) possess a mutation in the p53 gene (Table 3). Interestingly, in these 3 refractory cases, the mutations were all located in exon 5, a hotspot of p53 mutations in human ~ancer.~" The possibility that these exon 5 mutations specifically affect the drug-resistant status of the leukemia cells raises interesting questions. In each of the groups of relapse leukemia cases examined, the incidence of cases found to harbor p53 mutations probably represents a lower limit. Both the SSCP and the direct sequencing techniques fail to detect mutations that are present in less than 20% of the cell populations:' In addition, mutations maybepresentin exons other than exons 4 through 9 examined, or in introns. Alternatively, the frequency of mutations that we have found in relapse leukemias may represent only a fraction of the cases in which the wildtype suppressor function of p53 is inactivated. Relapse cases that lack detectable p53 mutations may have lost some of the p53 functions by inactivation of the p53 protein through complex formation with other cellular proteins, eg, mdm2.42.43 Studies of the inactivation of p53 function in relapse leukemias by means other than mutations are in progress. It is important to consider why acute leukemia patient samples as well as cell lines infrequently display LOHat the p53 locus, whereas human solid tumors often show LOH at the p53 locus on chromosome 17p. The difference may From www.bloodjournal.org by guest on June 18, 2017. For personal use only. p53 MUTATIONS IN RELAPSE ACUTE T LEUKEMIA lie in the nature of acute leukemia cells as compared with cells of malignant solid tumors. The generation of malignant human solid tumors requires a series of 6 to 8 or more genetic alterations in the same ce11“; the malignant cells are “transformed” and transplantable, and possess many in vitro characteristics of “tumor cells.” In contrast, in acute leukemias, malignancy is engendered by cells that have undergone fewer genetic alterations4 and that have few, if any, characteristics of “tumor cells.”47 Specifically, acute leukemia cells are “malignant,” ie, life-threatening, even though they merely display the characteristics of differentiation-inhibited, proliferating precursor cells (ibid), and may lack many or most of the in vitro criteria of “tumor cells,” We propose that, in acute leukemia cells, mutation of each p53 allele provides the leukemic cell with a growth advantage through the e l i n a t i o n of normal suppressor functions and, especially, through the acquisition of dominant oncogenic functions (M. Hsiao, E. Dom, J. Yeargin, and M. Haas, manuscript submitted, and Dittmer et ala). Thus, whereas the acquisition of each dominantly acting mutated p53 allele is significant for the potentiation of the leukemic phenotype of acute leukemia cells, in solid tumors a fully tumorigenic and metastatic phenotype necessitates the loss of each functional p53 allele, hence the frequent loss of the functional allele through LOH. REFERENCES 1. Bishop JM: The molecular genetics of cancer. Science 235:305, 1987 2. Finlay CA, Hinds PW, Levine AJ: The p53 proto-oncogene can act as a suppressor of transformation. Cell 57:1083, 1989 3. Nigro JM, Baker SJ, Preisinger AC, Jessup JM, Hostetter R, Cleary K, Bigner SH, Davidson N, Baylin S, Devilee P, Glover T, Collins FS, Weston A, Modali R, Harris CC, Vogelstein B: Mutations in the p53 gene occur in diverse human tumour type. Nature 342:705, 1989 4. Iggo R, Gatter J, Bartek J, Lane D, Harris AL: Increased expression of mutant forms of p53 oncogene in primary lung cancer. Lancet 355:675, 1990 5. Takahashi T, Nau MM, Chiba I, Birrer MJ, Rosenberg RK, Vinocour M, Levitt M, Pass H, Gazdar AF, Minna JD: P53: A frequent target for genetic abnormalities in lung cancer. Science 246:491, 1989 6. Bressac B,KewM, Wands J, Ozturk M: Selective G to T mutations of p53 gene in hepatocellular carcinoma from Southern Africa. Nature 350429, 1991 7.Hsu IC, Metcalf RA, Sun T, Welsh JA, Wang NJ, Hanis CC: Mutational hotspot in the p53 gene in human hepatocellular carcinomas. Nature 350:427, 1991 8. Sidransky D, Von Eschenbach A, Tsai YC, Jones P, Summerhayes I, Marshall F, Paul M, Green P, Hamilton SR, Frost P, Vogelstein B: Identification of p53 gene mutations in bladder cancers and urine samples. Science 252:706, 1991 9. Marks JR, Davidoff A M , Kerns BJ, Humphrey PA, Pence JC, Dodge RK, Clarke-Pearson DL, Iglehart JD, Bast RC, Berchuck A: Overexpression and mutation of p53 in epithelial ovarian cancer. Cancer Res 51:2979, 1991 10. Ahuja H, Bar-Eli D, Advani SH, Benchimol S, Cline MJ: Alteration in the p53 gene and the clonal evolution of the blast crisis of CML. Proc Natl Acad Sci USA 86:6783, 1989 11. Kelman Z , Prokocimer M, Peller S, Kahn Y, Rechavi G , Manor Y, Cohen A, Rotter V: Rearrangement in the p53 gene in 2929 Philadelphia chromosome positive chronic myelogeneous leukemia. Blood 74:2318, 1989 12. Sakashita A, Hattori T, Miller CW, Suzushima H, Asou N. Takatsuki K, Koeffler HP: Mutations of the p53 gene in adult Tcell leukemia. Blood 79:477, 1992 13. Sugito S, Yamato K, Sameshima Y, Yokota J, Yano S, Miyoshi I: Adult T-cell leukemia: Structures and expression of the p53 gene. Int J Cancer 495380, 1991 14. Diller L, Kassel J, Nelson CE, Gryka MA, Litwak G, Gebhardt M, Bressac B, Ozturk M, Baker SJ, Vogelstein B, Friend SH: P53 functions as a cell cycle control protein in osteosarcomas. Mol Cell Biol 105772, 1990 15. Masuda H, Miller C, Koeffler HP, Battifora H, Cline MJ: Rearrangement of the p53 gene in human osteogenic sarcomas. Proc Natl Acad Sci USA 84:7716, 1987 16. Baker SJ, Fearon ER, Nigro JM, Hamilton SR, Preisinger AC, Jessup JM, vanhinen P, Ledbetter DH, Barker DF, Nakemura Y, White R, Vogelstein B: Chromosome 17 deletions and p53 gene mutations in colorectal carcinomas. Science 244:217, 1989 17. Sidransky D, Mikkelsen T, Schwechheimer K, Rosenblum ML, Cavanee W, Vogelstein B: Clonal expansion of p53 mutant cells is associated withbrain tumor progression. Nature 3552346, 1992 18. Mashal R, Shtalrid M, Talpaz M, Kantarjian H, Smith L, Beran M, Cork A, Trujillo J, Gutterman J, Deisseroth A: Rearrangement and expression of p53 in the chronic phase and blast crisis of chronic myelogenous leukemia. Blood 75:180, 1990 19. Ahuja H, Bar-Eli M, Advani SH, Benchimol S, Cline MJ: Alterations in the p53 gene and the clonal evolution of the blast crisis of chronic myelocytic leukemia. Proc Natl Acad Sci USA 86:6783, 1989 20. Soussi T, Jonveaux P p53 gene alterations in human hematological malignancies: A review. Nouv Rev Fr Hematol 33:477, 1991 21. Fults D, Brockmeyer D, Tullous MW, Pedone CA, Cawthon RM: p53 mutation and loss of heterozygosity on chromosome 17 and 10 during human astrocytoma progression. Cancer Res 52:674, 1992 22. Shirasawa S, Urabe K, Yanagawa Y, Toshitani K, Iwama T, Sasazuki T p53 gene mutations in colorectal tumors from patients with familial polyposis coli. Cancer Res 51:2874, 1991 23. Cheng J, Haas M: Frequent mutations in the p53 tumor suppressor gene in human leukemia T-cell lines. Mol Cell Biol 105502, 1990 24. Harvey DM, Levine AJ: p53 alteration is a common event in the spontaneous immortalization of primary BALBlc murine embryo fibroblasts. Genes Dev 5:2375, 1991 25. Gaidano G , Ballerini P, Gong JZ, Inghirami G , Neri A, Newcomb EW, Magrath IT,Knowles DM, Dalla-Favera R: p53 mutations in human lymphoid malignancies: Association with Burkitt lymphoma and chronic lymphocytic leukemia. Proc Natl Acad Sci USA 88:5413, 1991 26. Jonveaux P, Berger R: Infrequent mutations in the p53 gene in primary human T-cell acute lymphoblastic leukemia. Leukemia 5339, 1991 27. Yeargin J, Cheng J, Yu AL, Gjerset R, Bogart M, Haas M: p53 mutation in acute T-cell lymphoblastic leukemia is of somatic origin and is stable during establishment of T-ALL cell lines. J Clin Invest 91:2111, 1993 28. Orita M, Suzuki Y, Sekiya T, Hayashi K: Rapid and sensitive detection of point mutations and DNApolymorphism using the polymerase chain reaction. Genomics 5874, 1989 29. Buchman VL, Chumakov PM, Ninkina NN, Samarrina OP, Georgiev G P A variation in the structure ofthe protein-coding region of the human p53 gene. Gene 70:245, 1988 30. Cabanillas F, Pathak S, Grant G, Hagemaister FB, McLaugh- From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 2930 lin P, Swan F, Rodrigues MA, Trujillo J, Cork A, Butler JJ, Katz R, Freireich EJ: Refractoriness to chemotherapy and poor survival related to abnormalities of chromosomes 17and 7 in lymphoma. Am J Med 87:167, 1989 3 1. Chin KV, Ueda K, Pastan I, Gottesman MM: Modulation of activity of the promoter of the human MDRl gene by ras and p53. Science 255:459, 1992 32. Hams N, Brill E, Shohat 0, Prokocimer M, Wolf D, Arai N , Rotter V: Molecular basis for heterogeneity of the human p53 protein. Mol Cell Biol 64650, 1986 33. Matlashewski GJ, Tuck S, Pim D, Lamb P, Schneider J, Crawford LV: Primary structure polymorphism at amino acid residue 72 of human p53. Mol Cell Biol 7:961, 1987 34. Buchman VL, Chumakov PM, Ninkina NN, Samarina OP, Georgiev GP: A variation in the structure of the protein-coding region of the human p53 gene. Gene 70945, 1988 35. Ahuja HG, Testa MP, Cline MJ: Variation in the protein coding region of the human p53 gene. Oncogene 5 :1409, 1990 36. Calle-Martin 0, Fabregat V, Romero M, Soler J, Vives J, Yague J: AccII polymorphism of the p53 gene. Nucleic Acids Res 18:4963, 1991 37. Yeargin J, Cheng J, Haas M: Role of the p53 tumor suppressor gene in the pathogenesis and in the suppression of acute lymphoblastic T-cell leukemia. Leukemia 6:85S, 1992 (suppl 3) 38. Soussi T, Caron de Fromentel C, Sturtzbecher HW, Ullrich S, Jenkins J, May P Evolutionary conservation of the biochemical properties of p53: Specific interaction ofXenopus laevis p53 with SV40 large T antigen and mammalian heat shock proteins 70. J Virol 63:3894, 1989 39. Cavenee WK. Dryja TP, Phillips RA, Benedict WF, Godbout HSIAO ET AL R, Gallie BL, Murphree AL, Strong LC, White RL: Expression of recessive alleles by chromosomal mechanisms in retinoblastoma. Nature 305:779, 1983 40. Caron de Fromentel C, Soussi T: TP53 tumor suppressor gene: A model for investigating human mutagenesis. Genes Chromosom Cancer 4:1, 1992 41. Cheng J, Haas M: Sensitivity of detection of heterozygous point mutations in p53 cDNA by direct PCR sequencing. PCR Methods Applications 1:199, 1992 42. Momand J, Zambetti GP, Olson DC, George D, Levine AJ: The mdm-2 oncogene product forms a complex with the p53 protein and inhibits p53-mediated transactivation. Cell 69:1237, 1992 43. Oliner JD, Kinzler KW, Meltzer PS, George DL, Vogelstein B: Amplification of a gene encoding a p53-associated protein in human sarcomas. Nature 35830, 1992 44. Fearon ER, Vogelstein B: A genetic model for colorectal tumorigenesis. Cell 61:759, 1990 45. Folkman J, Hanahan D: Expression of angiogenic phenotype during development of murine and human cancer, in Bntgge J (ed): Origins of Human Cancer: A Comprehensive Review. Cold Spring Harbor, NY, Cold Spring Harbor Laboratory, 1991, p 803 46. Renan MJ: How manymutations are required for tumorigenesis? Implications from human cancer data. Mol Carcinog 7: 139, 1993 47. Gjerset RA, Arya J, Volkman S, Haas M. Association of induction of a fully tumorigenic phenotype in murine radiationinduced T-lymphoma cells with loss of differentiation antigens, gain of CD44, and alterations in p53 protein levels. Mol Carcinog 5: 190, 1992 48. Dittmer D,Pati S, Zambetti G, Chu S, Tereslu AK, Moore M, Finlay C, Levine AJ: Gain of function mutations in p53. Nature Genet 442, 1993 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1994 83: 2922-2930 Nonhereditary p53 mutations in T-cell acute lymphoblastic leukemia are associated with the relapse phase MH Hsiao, AL Yu, J Yeargin, D Ku and M Haas Updated information and services can be found at: http://www.bloodjournal.org/content/83/10/2922.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.