Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Social immunity wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Globalization and disease wikipedia , lookup
Vaccination policy wikipedia , lookup
Germ theory of disease wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Cysticercosis wikipedia , lookup
Herd immunity wikipedia , lookup
Immunocontraception wikipedia , lookup
Whooping cough wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Vaccination wikipedia , lookup
Poliomyelitis eradication wikipedia , lookup
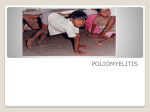
Epidemiology of Poliomyelitis Ashry Gad Mohamed MBchB, MPH, DrPH Prof. of Epidemiology Medical College, KSU • • First described by Michael Underwood in 1789 • Spectrum Polio = grey & Myelitis =marrow (spinal cord) & Itis = inflamation 95% asymptomatic. 4-8% minor non-specific illness (URTI, GIT, influenza like) 1-2% Non paralytic aseptic meningitis. 1% Flaccid paralysis Outcomes of poliovirus infection Asymptomatic Aseptic menigitis 0 20 Minor non-CNS illness Paralytic 40 60 Percent 80 100 Flaccid paralysis • • • • • • Asymmetrical. Affect large muscles. No sensory loss. No changes in recognation. 80% spinal, 19% bulbospinal & 1-2% bulbar Mortality: 2-5% children 15-30% adults 25-75% bulbar type Polio Eradication • Before 1979 whole world • Last case in United States in 1979 • Western Hemisphere certified polio • • • • • free in 1994 1988 350.000 2001 483 2003 784 2006 1999 2007 673 Level 2009 2010 Globally 1606 874 Endemic countries 1256 211 Non endemic countries 350 663 Country 2009 2010 Pakistan 89 134 Afphanistan 38 23 Mauritania 13 5 India 741 41 Chad 64 18 Nigeria 388 13 Congo 3 75 Sudan 45 - Angola 29 30 Russia 0 14 Wild Poliovirus 1988 Poliomyelitis 2004 Poliovirus • Enterovirus (RNA) • Three serotypes: 1, 2, 3 • Minimal heterotypic immunity between serotypes • Rapidly inactivated by heat, formaldehyde, chlorine, ultraviolet light Poliomyelitis Pathogenesis • Entry into mouth • Replication in pharynx, GI tract, local lymphatics • Hematologic spread to lymphatics and central nervous system • Viral spread along nerve fibers • Destruction of motor neurons Poliovirus Epidemiology • Reservoir Human • Transmission Fecal-oral Oral-oral possible • Communicability 7-10 days before onset Virus present in stool 3-6 weeks Poliovirus Vaccine • 1955 Inactivated vaccine • 1961 Types 1 and 2 monovalent OPV • 1962 Type 3 monovalent OPV • 1963 Trivalent OPV • 1987 Enhanced-potency IPV (IPV) Inactivated Polio Vaccine • Contains 3 serotypes of vaccine virus • Grown on monkey kidney (Vero) cells • Inactivated with formaldehyde • Contains 2-phenoxyethanol, neomycin, streptomycin, polymyxin B Oral Polio Vaccine • Contains 3 serotypes of vaccine virus • Grown on monkey kidney (Vero) cells • Contains neomycin and streptomycin • Shed in stool for up to 6 weeks following vaccination Inactivated Polio Vaccine • Highly effective in producing immunity to poliovirus • >90% immune after 2 doses • >99% immune after 3 doses • Duration of immunity not known with certainty Oral Polio Vaccine • Highly effective in producing immunity to poliovirus • 50% immune after 1 dose • >95% immune after 3 doses • Immunity probably lifelong Polio Vaccine Adverse Reactions • Rare local reactions (IPV) • Vaccine associated paralytic poliomyelitis (OPV) Vaccine-Associated Paralytic Polio • Increased risk in persons >18 years • Increased risk in persons with immunodeficiency • No procedure available for identifying persons at risk of paralytic disease • 5-10 cases per year with exclusive use of OPV • Most cases in healthy children and their household contacts Vaccine-Associated Paralytic Polio (VAPP) 1980-1998 • Healthy recipients of OPV • Healthy contacts of OPV recipients • Community acquired • Immunodeficient 41% 31% 5% 24% Polio Vaccine Contraindications and Precautions • Severe allergic reaction to a vaccine component or following a prior dose of vaccine • Moderate or severe acute illness Global Polio Eradication Initiative Objectives: 1-To interrupt transmission of the wild poliovirus ASAP. 2-To achieve certification of global polio eradication. 3-To contribute to health systems development and strengthening routine immunization and surveillance for communicable diseases in a systematic way. Global Polio Eradication Initiative Strategies: 1. high infant immunization coverage with four doses of oral poliovirus vaccine (OPV) in the first year of life; 2. supplementary doses of OPV to all children under five years of age during SIAs; 3. surveillance for wild poliovirus through reporting and laboratory testing of all acute flaccid paralysis (AFP) cases among children under fifteen years of age; 4. targeted “mop-up” campaigns once wild poliovirus transmission is limited to a specific focal area Global Polio Eradication Initiative Before a WHO region can be certified polio-free, three conditions must be satisfied: 1. there are at least three years of zero polio cases due to wild poliovirus; 2. disease surveillance efforts in countries meet international standards; and 3. each country must illustrate the capacity to detect, report and respond to “imported” polio cases Poliomyelitis surveillance • Acute flaccid paralysis All cases of acute flaccid pralysis among children younger than 15 years and all cases of suspected polio in any person at any age. • Performance indicators: 1. Completeness of reporting (80% at least). 2. Sensitivity of surveillance (1/100,000). 3. Completeness of case investigation (80% adequate stool specimen). 4. Complete follow up (80% 60 days). 5. Lab investigation of all cases in WHO ref. lab. The most important aspect of this classification is the collection of 2 adequate stool samples from all cases. Samples are considered adequate if both the specimens (1) are collected within 14 days of paralysis onset and at least 24 hours apart; (2) are of adequate volume (8-10g) and (3) arrives at a WHOaccredited laboratory in good condition (ie, no desiccation, no leakage), with adequate documentation and evidence of cold-chain maintenance References 1-http://www.emro.who.int/PolioFax/ 2-http://www.who.int/topics/poliomyelitis/en/ 3-http://healthcare.utah.edu/healthinfo/adult/infectious/ polio.htm 4- Control of communicable diseases in man, manual. APHA 2005.