Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adaptive immune system wikipedia , lookup
DNA vaccination wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Innate immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
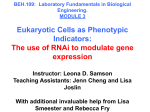
Dan Peer A daunting task: manipulating leukocyte function with RNAi Author’s address Dan Peer1,2 1 Laboratory of NanoMedicine, Department of Cell Research and Immunology, George S. Wise Faculty of Life Science, Tel Aviv, Israel. 2 Center for Nanoscience and Nanotechnology, Tel Aviv University, Tel Aviv, Israel. Summary: RNA interference (RNAi) has advanced into clinical trials. In spite of the progress made in systemic RNAi delivery to the liver and solid tumors, delivery of RNAi to leukocytes remains challenging and less advanced. Manipulating leukocyte function with RNAi holds great promise for streamlining the drug discovery process by facilitating in vivo drug target validation and for facilitating the development of RNAi-based therapy platforms for leukocyte-implicated diseases, such as blood cancer, inflammation, and leukocyte-tropic viral infections. In this review, progress in delivery strategies of RNAi payloads to leukocytes, which are notoriously difficult cells to transduce with RNAi, is discussed with special emphasis on the challenges and potential opportunities for manipulating leukocyte function with RNAi. Correspondence to: Dan Peer Tel Aviv University, Cell Research & Immunology Laboratory of NanoMedicine George S. Wise Faculty of Life Science Britannia Building, room 226 Tel Aviv 69978, Israel Tel.: +972 3640 7925 Fax: +972 3640 5926 e-mail: [email protected] Acknowledgements Dan Peer thanks Ms. Varda Wexler for her help with the graphics and illustrations and the Peer laboratory members for helpful discussions. This work was supported in part by grants from the Lewis Family Trust, Israel Science Foundation (Award #181/10), the Kenneth Rainin Foundation, the Israeli Centers of Research Excellence (ICORE), Gene Regulation in Complex Human Disease, Center No 41/11, the FTA: Nanomedicine for Personalized Theranostics, and by The Leona M. and Harry B. Helmsley Nanotechnology Research Fund awarded to D. P. The author has no conflicts of interest to declare. This article is part of a series of reviews covering RNA Regulation of the Immune System appearing in Volume 253 of Immunological Reviews. Immunological Reviews 2013 Vol. 253: 185–197 Printed in Singapore. All rights reserved © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 0105-2896 Keywords: RNAi, leukocytes, integrins, nanoparticles, liposomes Introduction RNA interference (RNAi) is a natural cellular mechanism for small RNA-guided posttranscriptional suppression of gene expression that is conserved in a wide range of organisms. The endogenous small RNAs responsible for gene regulation are processed to approximately 19–23 nucleotides imperfectly paired, double-stranded RNAs with two unpaired nucleotides at their 5′-phosphorylated ends and unphosphorylated 3′-ends (1–3). RNAi can be activated also exogenously by expressing short hairpin RNAs (shRNA) using viral vectors that are processed in the cell into small RNAs that mimic the endogenous gene-silencing RNAs or by introducing synthetic small interfering RNAs (siRNAs) directly into the cell cytoplasm (4–6). In the cytoplasm, siRNAs are incorporated into the endogenous machinery responsible for gene silencing, the RNAinduced silencing complex (RISC), which removes one strand. The remaining antisense RNA strand then guides the RISC to bind, cleave, and block translation of mRNAs bearing complementary sequences (5, 6). Since the target mRNA is destroyed and the antisense strand is protected from degradation within the RISC, the same RNA template can be used repeatedly to eliminate many transcripts. Indeed, gene knockdown occurs with picomolar concentrations of RNA and can last for several © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 185 Peer Manipulating leukocyte function with RNAi days in dividing cells, where it is diluted with each cell division, and for several weeks in non-dividing cells, even in vivo (7–9). Soon after RNAi was found in mammals (1), synthetic siRNAs were shown to treat disease in mice (10). Small RNAs were quickly proclaimed as the ‘next new class of drugs’. Eagerness sprinted high because of the potential of these molecules to knockdown any gene of interest to treat almost any disease by targeting otherwise ‘undruggable’ targets, such as molecules without ligand-binding domains or enzymatic function. Although initially gene knockdown was thought to be perfectly specific for the target gene, it soon became clear that off-target effects were predominant via suppression of genes harboring non-identical but homologous sequences (such as in the case of endogenous microRNAs) and by recognition of the innate immune RNA sensors that can initiate interferon and cytokine secretion and activate complement and coagulation cascades. Indeed, some of the early demonstrations of RNAi therapeutic effects in small animals may have been due to off-target effects (11, 12). However, chemical modifications of the RNA molecule can largely eliminate off-target effects without compromising target gene knockdown. Silencing of gene expression in vitro is a great tool for functional and validation studies (13, 14). Nevertheless, understanding gene expression in a disease model by validating specific genes’ role in vivo along with the potential to induce therapeutic gene silencing opens new avenues for utilizing RNAi as a novel therapeutic modality and brings the era of personalized medicine a step further from a vision to a potential reality. Introducing RNAi in medicine is achieved by designing specific RNAi molecules such as miRNA mimics and siRNAs. RNAi-induced gene silencing mirrors the inhibitory effects of conventional pharmaceuticals, primarily protein-based drugs such as antibodies and vaccines and small molecules, which mainly block their targets’ function. However, some disease-related molecules do not have enzymatic function or have a conformation that is not accessible to conventional drugs or small molecule compounds, and hence, these molecules are considered ‘non-druggable’ targets. Nondruggable molecules have been successfully targeted by RNAi approaches in vivo (15–19), demonstrating an exclusively allele-specific gene silencing (20, 21). In addition, blocking the target’s gene expression rather than its activity is more efficient, as single mRNA molecule translates multiple copies of protein. Another advantage of RNAi over conventional pharmaceuticals is the ease of synthesis and production of potent regulators. As opposed to proteinbased drugs, RNAi synthesis does not necessitate cellular expression systems or refolding steps. As for small molecule-based drugs, the major disadvantage is the slow and difficult process for identification and optimization (22), whereas the identification of functional and specific RNAi constructs is rapid and involves well-demonstrated strategies and algorithms that facilitate their optimization. Although most proteins and some small molecule-based drugs do not require intracellular access to obtain therapeutic function, RNAi-based therapeutics necessitates intracellular delivery, an additional challenging task for the development of a new efficient RNAi-based therapeutic. Despite the promise, developing RNAi for therapeutics has proven challenging. Like most drug development, there is no rapid solution, and many pharmaceutical companies that invested considerable sums in developing RNA-based drugs have discontinued their investigations. Although many of the hurdles in developing RNAi-based therapeutics have been already addressed, the main challenge is figuring out the way of delivering small RNAs into cells in a therapeutically relevant manner with minimal adverse effects. Small RNAs being considered therapeutic drugs include not only siRNAs but also mimics of endogenous microRNAs for suppressing the expression of many genes. The delivery hurdle that needs to be solved for administering siRNAs and imperfectly paired microRNA mimics is essentially the same, although antagonizing endogenous microRNAs using single-stranded antisense oligonucleotides may be somewhat simpler. When injected intravenously, RNAi molecules are rapidly cleared by renal filtration and are susceptible to degradation by extracellular RNases. The RNAi half-life can be increased substantially by chemical modifications to eliminate susceptibility to endogenous exonucleases and endonucleases and by incorporating the RNA into a larger moiety, above the molecular weight cutoff for kidney filtration. However, entering the cell is still the biggest hurdle. Because of their large molecular weight (approximately 13.5 kDa), net negative charge, and hydrophilicity, naked RNAi molecules do not cross the plasma membrane (5, 11). Although cells can endocytose many types of modified RNAs, another important bottleneck is getting the RNA efficiently out of the endosomes into the cytosol where the RNAi machinery resides. It has been shown that the amount of siRNAs that can be bursting from the endosomes when lipid-based nanoparticles are used as delivery system is enormously small (1–2%), making this 186 © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Peer Manipulating leukocyte function with RNAi process ineffective (23). In addition, unless modified, siRNAs are recognized by Toll-like receptors (TLRs) (11, 24) and other cellular soluble protein sensors such as MDA5 and RIG-I (25), which activate cellular cascades that stimulate the immune system and cause a global suppression effect on gene expression, generating off-target effects, and causing misinterpretation of the gene expression analysis (14). Many excellent reviews have been published (5, 6, 14, 26, 27) describing these challenges and the use of different strategies to overcome some of these hurdles using innovative nanotechnology and protein engineering. In spite of the progress in systemic RNAi delivery to the liver and solid tumors, systemic delivery of RNAi to leukocytes remains challenging. Delivery of RNAi molecules to leukocytes holds great promise for streamlining drug discovery by facilitating in vivo drug target validation and for facilitating the development of an RNAibased therapy platform for leukocyte-implicated diseases such as inflammation, blood cancers such as leukemia, lymphoma, and myeloma, and leukocyte-tropic viral infections such as human immunodeficiency virus (HIV), ebola, and dengue (14, 28–30). In this review, progress in the delivery of RNAi molecules to leukocytes, which are notoriously difficult to transduce with RNAi, is described. Focus is given to various strategies that have been developed, among them several of the strategies developed by our group to efficiently deliver and transduce subsets of leukocytes for various applications. Special emphasis is made on the challenges and potential opportunities to manipulate leukocyte function with RNAi. A B C D E F G H Multiple strategies for RNAi delivery into leukocytes Fig. 1. RNAi delivery strategies available for leukocytes. (A) siRNA encapsulated in PEGylated polysome nanoparticles with ligand molecules attached to the PEG; (B) a complex of siRNAs with the peptide transduction domain–dsRNA-binding domain (PTD-DRBD) fusion protein; (C) siRNA synthetically linked to an aptamer; (D) siRNA synthetically conjugated to a CpG oligonucleotide; (E) an atelocollagen–siRNA complex; (F) the 9 arginine (9R) strategy is shown with either an integrin-targeted and stabilized nanoparticle (I-tsNP)-entrapping siRNA (G), a single-chain variable fragment (scFv)-protamine fusion protein loaded with siRNAs (H), or with a ligand (data not shown). Leukocytes and hematopoietic cancer cells are among the most challenging targets for RNAi delivery, as these cells are highly resistant to conventional transfection reagents and are dispersed in the body, making it challenging to achieve the successful localization of RNAi molecules (be it single- or double-stranded RNA) to the target cells or to deliver these molecules passively via systemic administration (30, 31). Therefore, active-targeted delivery systems are being developed, in which specific antibodies, ligands, and ligand mimetics are used to mediate the targeting and internalization of the RNAi payloads into cells (Fig. 1). Some of these strategies have been shown to deliver siRNAs into leukocytes in vitro, including PEGylated nanoscale liposomes decorated with ligands that bind to receptors expressed on leukocytes (Fig. 1A). In addition, Huang and King (32) described a P-selectin-coated nanoscale-liposome system that entrapped siRNAs. Their work has shown that these P-selectin-, PEG- coated nanoscale liposomes could be absorbed onto the inner surface of microrenathane tubing. The coated surface could specifically capture targeted cells from physiological shear flow, efficiently deliver encapsulated siRNA into adherent cells, and effectively silence the target gene neutrophil elastase. With this approach, the investigators created a highly localized concentration for RNAi delivery in the circulatory system, providing circulating target cells © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 187 Peer Manipulating leukocyte function with RNAi adequate time to interact with the therapeutic payloads. Another efficient delivery strategy makes use of the peptide transduction domain–double-stranded RNA-binding domain (PTD-DRBD) fusion protein (Fig. 1B). In this approach, the DRBD binds to the siRNAs, thus masking the negative charge of the molecules, whereas the PTD mediates the cellular uptake of the complex (33). Moreover, siRNAs can also be delivered into leukocytes via conjugation to RNA aptamers that bind to specific target molecules, such as glycoprotein 120 (34, 35), without interfering with the binding of the siRNAs to Dicer (Fig. 1C). In addition to these strategies, other approaches have also been demonstrated for delivering RNAi into leukocytes and are discussed below. CpG-conjugated siRNA Unmethylated CpG oligonucleotides (Fig. 1D) internalize efficiently into dendritic cells, myeloid cells, and B-lymphocytes following binding to TLR9. In a study by Kortylewski et al. (36), CpG oligonucleotides were conjugated to an siRNA targeting the immune suppressor gene STAT3. This conjugate was demonstrated to silence Stat3 in mice, leading to the activation of tumor-associated dendritic cells, macrophages, and B-lymphocytes that mediate potent antitumor immune responses, and resulting in tumor cell apoptosis. However, the siRNA in this study was unmodified, and thus its half-life was reduced and its therapeutic effect limited. Atelocollagen-complexed siRNA Atelocollagen is a type I collagen from calf dermis that does not cause antigenicity or toxicity in animals as a result of pepsin digestion of the antigenic telopeptides. The positively charged lysine and hydroxylysine residues, which are rich in collagen, are thought to mediate the formation of the atelocollagen–siRNA complex. Ishimoto et al. (37) demonstrated that when siRNAs were administrated intravenously with atelocollagen (Fig. 1E), the incorporation of the siRNAs into murine macrophages, monocytes, and fibroblasts was facilitated, without causing adverse effects such as the induction of type I interferon or liver and renal damage. Cationic nona-D-arginine peptide fused to antibody fragments and complexed to siRNAs (Fig. 1F). This study demonstrated the ability of an RNAibased therapy to control and suppress HIV replication, without inducing toxicity in target cells. In another study (39), the 9R peptide fused to a dendritic cell-targeting 12-mer peptide delivered siRNAs targeting tumor necrosis factor-a (TNF-a) effectively in vivo, to suppress the production of TNF- a by dendritic cells upon induction in mice. Kim et al. (40) reported that TNF-a -targeted siRNAs, delivered to macrophages in vivo using a 9R peptide fused to the ACh receptorbinding peptide, reduced lipopolysaccharide (LPS)-induced TNF-a levels in the blood and brains of injected mice and led to a significant reduction in neuronal apoptosis. This strategy was used for delivering siRNAs against targets in the brain (41) using the Rabies’ peptide RVG, but strategies for delivering RNAi into the brain are beyond the scope of this review. Antibody–protamine fusion proteins as RNAi delivery vectors to leukocytes The Lieberman laboratory (7) devised one of the first strategies utilizing a receptor-mediated approach to deliver siRNAs directly into specific cell types in 2005. By fusing Fab antibody fragment (F105) against HIV-1 envelope (gp160) to human truncated protamine, a protein that nucleates DNA in the sperm, Song et al. (7) designed antibody–protamine fusion protein (Fig. 1H) for systemically delivering a mixture of anti-oncogenic siRNAs into mice grafted with gp160-expressing B16 melanoma cells. The fusion protein complexed siRNAs and selectively targeted gp160-expressing B16 cells and suppressed tumor growth (7). This strategy was used later on by us to develop a strategy for targeting activated leukocytes, as discussed below (42). Despite the promising results obtained from these RNAi delivery strategies, the whole spectrum of hematopoietic cells, including subsets of leukocytes, has not been fully addressed. In addition, the low payload delivered with these strategies might undermine their potential clinical efficacy. To circumvent these problems for delivering RNAi payloads to leukocytes, we have utilized leukocyte cell-specific integrins and have developed integrin-targeted stabilized nanoparticles (8) (Fig. 1G). Integrins as receptor targets for RNAi delivery Kumar et al. (38) described a single-chain variable fragment (scFv) form of anti-CD7, a T-cell-specific receptor that was modified with cysteine at its C-terminus to enable its conjugation to the cationic nona-D-arginine (9R) peptide for selective targeted delivery of siRNAs payloads into mouse T cells in vivo Integrins are the largest family of cell adhesion molecules that mediate cell–cell and cell–matrix interactions across a wide range of normal physiological and pathophysiological setting (43, 44). Integrins are a/b heterodimeric cell surface proteins; 15 a-subunits and 8 b-subunits have been 188 © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Peer Manipulating leukocyte function with RNAi identified in vertebrates, forming at least 24 distinct a/b heterodimers. The b2 and b7 integrins are exclusively expressed on the leukocyte surface. Integrins on leukocytes mediate the adhesive interactions critical for cell migration to sites of inflammation. Antibodies to integrins on leukocytes have been used to inhibit inflammatory reactions in the clinical setting. Two humanized antibodies, efalizumab (RaptivaTM) and natalizumab (TysabriTM), have been FDA approved for the treatment of autoimmune diseases (45, 46). In this way, antibodies ‘targeting’ leukocyte integrins have been used to interfere with the adhesive interactions of leukocytes for the treatment inflammatory disorders. To extend the utility of leukocyte integrin targeting across a broad range of leukocyte-implicated diseases (such as inflammation, allergy, blood cancers, and viral infection), we developed a strategy for targeting leukocytes via integrins expressed on hematological cells for siRNA delivery (42). This concept is supported by a number of lines of evidence. (i) Exclusive expression: a subset of integrins (i.e. b2 and b7 integrins) is exclusively expressed on leukocytes (47–49) enabling the selective targeting of hematopoietic cells. (ii) Efficient receptor internalization: integrins are constitutively internalized and recycled in leukocytes. Integrin recycling supports internalization of bound antibodies and peptides (50, 51), a prerequisite for activating RNAi pathway with siRNAs. (iii) Integrins undergo substantial activation-dependent conformational changes. Of the major classes of adhesion receptors, including the immunoglobulin domain superfamily (IgSF), the cadherins, and other transmembrane adhesion receptors (e.g. claudins and occludins), integrins are unique in achieving rapid and reversible upregulation from a basal, inactive state to a maximally adhesive state upon cell stimulation (43, 52, 53). Other adhesion receptors require in-membrane diffusion (both active and passive) and/or regulation of cell surface expression levels to modulate the magnitude of adhesion. The dramatic increase in affinity is obtained by a series of conformational changes that increase the affinity of the integrin for ligand and enhance the accessibility of the ligand-binding site (47, 54) (Fig. 2). The aberrant affinity modulation of integrins has been demonstrated in a variety of leukocyte-associated diseases. Targeting the high-affinity form of integrins is expected to enable selective RNAi delivery for aberrantly activated leukocytes. By leaving naive cells unaffected, selective targeting would be advantageous in reducing iatrogenic immune defects. © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Fig. 2. Model for global conformational changes of the extracellular portion of integrin LFA-1 (aLb2). (Left side) Bent, low-affinity conformation; (Right side) Extended conformation with open headpiece and open high-affinity I domain, the ligand-binding domain (labeled with green). This figure is modified from (124). Using leukocyte function-associated antigen-1 (LFA-1) antibody–protamine fusion protein (Fig. 1H) that complexes siRNAs via positively charged protamine moiety and direct the siRNAs-fusion protein complex to the target, we have shown that integrins can be used for siRNA delivery to activated leukocytes (42) using an activation-dependent conformational monoclonal antibody, AL-57(55), that was converted into a scFv and fused to protamine. A strategy to target only activated leukocytes holds great promise for specific in vivo gene silencing while avoiding delivery to resting leukocytes and thus potentially can mitigate the risk of offtarget effects in general and global immunosuppression in particular. A potential drawback of the antibody–protamine fusion protein approach is a low payload (5 siRNA molecules per delivery carrier) that could undermine its clinical usefulness (7, 42). In addition, each fusion protein needs to be prepared with the use of laborious molecular biology techniques, protein engineering, and purification methods. Thus, to increase the amount of payloads and achieve robust targeted gene silencing in leukocytes in vivo, we have devised a strategy based on lipid nanoparticles that were surface modified with an anti-integrin monoclonal antibody, termed integrin-targeted and stabilized nanoparticles (I-tsNP) (8) (Figs 1G and 3). I-tsNPs as leukocyte-specific vehicles I-tsNPs are prepared from neutral lipids and extruded to about 85 nm in diameter to become unilamellar vesicles (8, 56, 57). These lipid nanoparticles (LNPs) are then surface modified with the glycosaminoglycan hyaluronan 189 Peer Manipulating leukocyte function with RNAi Fig. 3. A schematic illustration of the processes involved in generating I-tsNP. Multilamellar vesicle (MLV) is extruded to form a unilamellar vesicle (ULV) with a diameter of approximately 85 nm. Hyaluronan is covalently attached to ULV. An antibody to the integrin is covalently attached to hyaluronan, generating I-tsNP. siRNAs are encapsulated by rehydrating lyophilized b7 I-tsNP siRNAs. This figure is modified from (8). (HA) (Fig. 3). As cationic lipids and polymers that form lipoplex and polyplex are non-natural and cause multilines of toxic effects (including cytokine induction, interferon response, and liver toxicities) (58–60), the use of a neutral lipid to form LNPs, which will not elevate cytokines, provoke a type I interferon response, activate lymphocytes, or trigger liver enzyme release provides a safer system. In addition, as I-tsNPs are small unilamellar lipid-based vesicles, which posses a defined size, they are easy to downsize by extrusion and provide a reproducible nanoscale system compared with lipoplex and polyplex that self-assemble with the RNAi payload. Coating the LNPs with high molecular weight (HMw) HA endows the carriers with several key advantages. HMw HA is a built-in cryoprotectant that stabilizes the particles during a cycle of lyophilization and rehydration by exchanging hydrogen bonds with water molecules during the lyophilization process (61) and in the circulation when they are administrated intravenously (62–64). HMw HA do not trigger a type I interferon response or cytokine induction and do not activate complement when bound on the surface of LNPs (65). HA also serves as a scaffold for antibody attachment to endow the LNPs’ targeting capabilities (8, 57). Anti-b7 integrin monoclonal antibodies were attached to the HMw HA-coated LNPs. This basically created a platform technology, as one can easily change the monoclonal antibody on the surface of these HA-coated LNPs, and thus it is possible to direct the LNPs and their payloads into subsets of leukocytes, as detailed below. The siRNAs were encapsulated within the I-tsNP upon rehydration of lyophilized particles with deionized water containing protamine-condensed siRNAs, achieving approximately 80% encapsulation efficacy as well as a payload of approximately 4000 siRNA molecules per particle. The siRNAs entrapped in the I-tsNP were protected from degradation and demonstrated effective silencing even after 190 pre-incubation with RNAse A or 50% serum for 2 h prior to the transfection of cells (8). Furthermore, I-tsNP encapsulating siRNA did not induce interferon responses, trigger cytokine induction, or activate lymphocytes in human peripheral blood mononuclear cells (PBMCs) (8). A single intravenous administration of 2.5 mg/kg Ku70-siRNAs, a DNA repair protein that ubiquitously expressed in all cells, served as a model target, induced approximately 80% reduction of protein expression levels in lymphocytes from the lamina propria, Peyer’s Patch, mesenteric lymph nodes, and spleen. Silencing of Ku70 was not observed in gut mononuclear leukocytes driven from b7-integrin knockout mice identically treated, demonstrating the high specificity of the targeting strategy. Ku70 was used as a surrogating marker for validating the I-tsNP as a delivery system for siRNA in gut leukocytes. Using this strategy, we validated the role of cyclin D1 in leukocytes during inflammatory bowel disease (IBD). Manipulating leukocyte function with RNAi: Cyclin D1 as a test case Cyclin D1 (CyD1) is part of the cyclin proteins family, which function as the regulatory subunits of cyclin/cyclindependent kinase (CDK) holoenzymes that regulates entry into and progression through the cell cycle (66–69). CyD1 expression is induced upon stimulation by growth factors, amino acids, hormones, and several oncogenes such as Ras, Src, ErbB2, and SV40 T antigen (66–70). Its binding partners are CDK4 and CDK6, and activated CyD1/CDK4 and CyD1/CDK6 complex phosphorylate the retinoblastoma protein to induce the expression of target genes essential for Sphase entry, resulting in facilitation of the progression from G1 to S phase (66, 70). CyD1 is also known to modulate local chromatin structure and transcription of genes involved in proliferation and differentiation through CDK-independent association with histone acetylases (e.g. CBP, P/CAF) © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Peer Manipulating leukocyte function with RNAi and deacetylases (69, 71). Amplification or overexpression of CyD1 is important in the development of many cancers including breast, prostate, colon parathyroid adenoma, lymphoma, and melanoma (13, 67, 69, 71–73). To suppress aberrant proliferation of leukocytes in inflammation, treatment with b7 I-tsNP-entrapped CyD1-siRNA reduced CyD1 mRNA expression in stimulated splenocytes, leading to potent suppression of proliferation both in vitro and in vivo upon intravenous administration of CyD1-siRNA (2.5 mg/kg) entrapped in b7 I-tsNP (8). Surprisingly, CyD1 knockdown blocked not only the proliferation but also the agonist-enhanced expression of T-helper 1 (Th1) cytokines interferon-c (IFN-c) , interleukin-2 (IL-2), IL-12, and TNFa, but not alter those of the Th2 cytokines IL-4 and IL-10. This specific inhibition in cytokine expression was not observed with other D-type cyclin family members (cyclin D2 or cyclin D3 knockdown) (8). To further understand if this observation is cell cycledependent process, cells were treated with aphidicolin, which blocks the cell cycle. Phorbol myristate acetate (PMA)/ionomycin treatment caused upregulation of CyD1 as well as Th1 and Th2 cytokines. CyD1 knockdown selectively suppressed Th1 cytokines in aphidicolin-treated and PMA/ionomycin-activated cells. This cell cycle-independent suppression of Th1 cytokines was also observed with the individual application of four different CyD1-siRNAs that targeted non-overlapping sequences in CyD1 mRNA (8), thereby ruling out the possibility that the blockade of Th1 cytokines was due to an off-target effect. Thus, CyD1 knockdown could preferentially suppress proinflammatory Th1 cytokine expression independently of any changes in the cell cycle. To validate the anti-inflammatory effects by CyD1 blockade in vivo, we injected ItsNP-entrapped CyD1-siRNA (2.5 mg/kg) into mice with dextran sulfate sodium-induced colitis. I-tsNP-delivered CyD1-siRNA potently reduced CyD1 mRNA as well as TNF-a and IL-12 mRNA levels comparable with that of the uninflamed gut. Remarkably, I-tsNP-delivered CyD1siRNA led not only to a drastic reduction in intestinal tissue damage but also to a potent suppression of leukocyte infiltration into the colon. CyD1-siRNAs entrapped in isotype control particles (IgG-sNP) did not induce silencing in the gut. These data have convincingly demonstrated that entrapment of condensed siRNAs inside these nanoparticles, in tandem with the targeting of the leukocyte integrin, which readily internalizes bound particles, enabled both highly efficient intracellular delivery and gene silencing in vivo in hematopoietic cells. © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 In a recent study (13), we continued to explore the use of RNAi against CyD1 as a potential therapeutic target for blood cancers such as mantle cell lymphoma (MCL). MCL is an incurable B-cell non-Hodgkin’s lymphoma, characterized by the t (11, 14) (q13;q32) translocation that juxtaposes the proto-oncogene CCND1, which encodes CyD1, downstream of the immunoglobulin heavy chain gene promoter. This leads to overexpression of CyD1, which is not expressed in normal B cells (74). CyD1 functions as an important regulator of the cell cycle G1-S transition. Complexes of CyD1 and CDK4 or CDK6 phosphorylate retinoblastoma 1, thus leading to release of E2F transcription factors, which enable the subsequent progression of the cell into S phase (75, 76). These complexes also titrate the CDK inhibitors p27kip1 and p21 away, therefore increase the kinase activity of cyclin ECDK2 complexes, which enhance the transition into S phase (77). The overexpression of CyD1, together with its established role as cell cycle progression regulator, highlights this gene as a potential central player in the pathogenesis of MCL (78). In our recent study (13), we used optimized siRNA or dicer substrates against CyD1 to potently downregulate CyD1 expression in well-characterized MCL cell lines. Knocking down CyD1 resulted in significant growth retardation, cell cycle arrest, and, most importantly, induction of apoptosis. These results mark CyD1 as a target for MCL and emphasize the therapeutic potential hidden in its silencing. I-tsNP: a leukocyte-specific platform technology for delivery of RNAi payloads To explore whether I-tsNPs can be defined as a platform technology for delivering RNAi payloads to leukocytes, we have changed the monoclonal antibody on the surface of the nanoparticles from anti-b7 integrin to anti-aLb2 integrin (LFA-1) that is highly expressed on all leukocytes and evaluated these LFA-1 I-tsNPs for systemic delivery of siRNA in a humanized mouse model (57, 79). We demonstrated that intravenous administration of LFA-1 I-tsNPs resulted in selective uptake of siRNAs by T cells and macrophages, the prime targets of HIV. In addition, intravenous administration of anti-CCR5 siRNA entrapped in LFA-1 I-tsNPs resulted in leukocyte-specific gene silencing that was sustained for 10 days. Finally, humanized mice challenged with HIV after anti-CCR5 siRNA treatment showed enhanced resistance to infection, as assessed by the reduction in plasma viral load and disease-associated CD4+ T-cell loss. This study (57) demonstrated the potential in vivo applicability of LFA-1-targeted 191 Peer Manipulating leukocyte function with RNAi siRNA delivery as anti-HIV prophylaxis but also validated the I-tsNPs as a leukocyte-specific RNAi platform. The potential drawbacks of I-tsNPs Assembly of a leukocyte-specific platform for RNAi delivery is a daunting task. From a chemistry, manufacturing, and controls standpoint, translating the I-tsNPs technology to a clinical setting is challenging. Each step of this assembly should be closely monitored (80, 81). More specifically, the I-tsNPs platform has several building blocks: lipids that form the LNPs; the glycosaminoglycan, HA, that stabilizes the nanoparticles and acts as a built-in cryoprotectant and as a scaffold for mAb binding; monoclonal antibodies that act as targeting moieties; human recombinant protamine that condense the nucleic acids; and the RNAi payloads. In addition to these challenges, risk of exposed monoclonal antibody Fc portion on the I-tsNP surface may cause potential immune toxicity and uptake by innate immune cells and antigen-presenting cells in a non-specific manner. Clustering of receptors by anti-integrin monoclonal antibody can trigger outside-in signaling event, which may cause immune stimulation and trigger proliferation. To reduce these risks, we are currently developing F(ab′)2 fragments that are coupled with different chemistries to the I-tsNP surface. In addition, we are using as internal controls non-blocking integrin monoclonal antibodies as F(ab′)2 fragments and probing for lymphocyte activation, interferon response, and cytokine induction, as well as exploring complement activation in human sera. Currently, we have not observed any signs of immunotoxicity with these novel systems. Hyaluronan as a targeting agent to tumors highly expressing CD44 we chose these cells as representative cells to examine the ability of the GAGs to deliver RNAi and induce potent and specific gene silencing. We first determined the expression level of CD44, HA ligand in these AML cells and found, as expected, a very high expression level of CD44 (CD44high; data not shown). Next, we labeled the HA, the GAG’s shell, with Alexa 488 and entrapped Cy3-siRNAs (Fig. 4A) in the particles’ clusters. Confocal microscopy analysis was done 45 min post transfection, revealing high transfection efficiency in all cells with co-localization of the siRNAs and the GAGs within the cytoplasm of the AML cells (Fig. 4A). We then wanted to verify that indeed functional knockdown could be detected using qualitative polymerase chain reaction (QPCR). As control cells, we used CV-1 cells that lack CD44 (62), verified by flow cytometry analysis (data not shown). CyD1-siRNAs A B We have recently shown that the HA coating on lipid nanoclusters, termed gagomers (GAGs), which are lipid clusters that do not form bilayer structures but hexagonal tubes, endow these carriers the ability to distinguish between cancerous and non-cancerous cells taken from the same patient with head and neck tumors (82). These particles were also efficient in entrapping and delivering RNAi payloads and inducing gene silencing in human lung adenocarcinoma cells (83). To determine whether these GAGs can also target primary acute myeloid leukemia (AML), fluorescence-assisted cell sorting-purified AML cells from two patients were used (This study protocol was approved by the ethics board of Sheba Medical Center in Ramat Gan, Israel). AML cells represent notoriously difficult cells to transduce with RNAi, so Fig. 4. Gagomers (GAGs) uptake and RNAi efficacy in primary acute myeloid leukemia (AML) cells. (A). Representative confocal microscopy analysis showing staining of GAGs (HA-labeled with Alexa 488 and entrapping Cy3-siRNAs) of primary FACS-sorted AML cells, which are CD44high from a patient that was newly diagnosed with AML. Microscopy was done 45 min post transfection after extensive washing and without cell fixation. (B). Representative relative gene expression of primary AML cells and CV-1 control cells (CD44 ) that were incubated with 50 nM CyD1-siRNA or control siRNA entrapped in the GAGs. After 24-h transfection, total RNA was isolated using EZRNA kit (biological industries, Israel) and cDNA was generated with high capacity cDNA kit (Life Technologies, Carlsbad, CA, USA) according to the manufacturers’ protocols. qRT-PCR was performed with Fast SYBRâ Green Master Mix and the ABI StepOnePlusTM instrument (Life Technologies).CCND1 (F:GAGGAGCCCCAACAACTTC C, R:GTCCGGGTCACACTTGATCAC) expression was normalized to the housekeeping genes eIF3a (F:TCCAGAGAGCCAGTCCATGC, R:CCTGC CACAATTCA TGCT) and eIF3c (F: ACCAAGAGAGTTGTCCGCAGTG, R: TCATGGCATTACG GATGGTCC). Analysis was done with the StepOneTM software V 2.1 (Life Technologies) using the multiple endogenous controls option. 192 © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Peer Manipulating leukocyte function with RNAi were used as surrogated markers or control, non-targeted siRNAs. All siRNAs were used at a concentration of 50 nM. QPCR was performed 24 h post transfection. Representative bars are shown in Fig. 4B. Although CyD1 is not the target of choice in this highly complex disease, the expression level of CyD1 in the patient sample was quite high compared with the normalized housekeeping genes. Knocking down CyD1 in the patient sample was specific, as evidenced by the control siRNA, and specific to these cells, as CV-1 that lacking the receptor CD44 did not reduce the expression level of CyD1 in a significant manner. These results support this new delivery strategy for RNAi that can be widely used for both leukocytes and non-leukocyte cells, but more experiments are needed to validate and examine potential adverse effects in human PBMCs and in vivo in mouse models. Challenges in delivery of RNAi payloads to leukocytes Immunostimulatory effects of the RNAi payloads and their carriers Double-stranded RNA induces an immune response as a defense mechanism against viral infection (4) upon interaction with RNA-binding proteins such as TLRs and protein kinase receptor (PKR). This recognition occurs on the cell surface or within the cell (in the cytoplasm or endosome compartments) and leads to innate immunity activation, i.e. production of pro-inflammatory cytokines, such as IL-6 and TNF-a, and triggering type I IFN responses (84). siRNAs can stimulate the immune system in a sequence-independent manner such as induction of TLR3 (85) and IFN pathways (86), as well as in a sequence-dependent way as in the case of uridine (U) or guanosine adenine/uridine (GA/GU)-rich regions recognition via TLR7 and TLR8 (87– 89). Immunostimulatory effects can also be length dependent. Whereas short siRNAs (12 and 16 nt long) have been reported to poorly stimulate immune cells, longer constructs increased significantly cytokine production – independent of their sequence (88). It is important to note that immunostimulation by siRNA is cell type dependent (87, 90), for example, although non-immune cells do not express TLRs or express them at low levels, they retain the ability to recognize exogenous RNAs via alternative pathways such as the PKR pathway (91). Besides optimizing the sequence (92), structure (93, 94), or length (88) of the siRNA, chemical modifications can also be applied for mitigating immunogenicity (95). Of note, immunogenic siRNA sequences could be deliberately applicable in specific treatments such as viral © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 infections or cancer (91), where activation of the immune system is required to ameliorate the disease. Among non-viral delivery systems for RNAi, cationic lipids have been widely used as part of the formulation (96– 98). Cationic lipids are lipid bilayer-forming vesicles with a positive surface charge. Common cationic lipids that were extensively studied included 1,2-dioleoyl-3-trimethylammonium-propane (DOTAP) and N-(1-(2,3- Dioleoyloxy)propyl) -N,N,N-trimethyl-ammoniummethyl sulfate (DOTMA), 3b-[N-(N’, N’-Dimethy lainin(ethyl) carbamoyl cholesterol (DC-Chol), and Dimethyldioctadecylammonium bromide, but the variety of cationic lipids and lipid-like novel materials is enormous (99, 100). Cationic liposomes showed a superior adjuvant effect compared with anionic or neutral liposomes as demonstrated in vivo in animal models (101, 102). As cationic liposomes can activate the complement system and cause rapid clearance by macrophages of the mononuclear phagocytic system (97), these cationic particles can be used to enhance and modulate the immune response in a desirable direction and represent an efficient tool when designing tailor-made adjuvant for a specific disease target. The use of cationic liposomes in vivo elicited dose-dependent toxicity, as demonstrated by the multivalence cationic liposome LipofectAMINE2000 in a comparison with the monovalence cationic lipids, such as DOTAP (103, 104). Although it was found that DOTAP-based cationic liposomes also caused severe damage to the mitochondria (105), the specific mechanism by which this cytotoxicity occurs remains unknown and might involve different cellular pathways depending on the particular cell type. In addition, mice treated with positively charged LNPs containing DOTAP showed increased liver enzyme release and mild body weight loss compared with mice treated with neutral or negatively charged LNPs (30, 58). Intravenous administration of cationic LNPs induced type I IFN response and elevated mRNA levels of interferon responsive genes 15- to 25-fold higher than neutral and negatively charged NPs in mouse splenocytes. Treatment with cationic LNPs provoked a dramatic pro-inflammatory response by inducing Th1 cytokine expression (IL-2, IFN c, and TNFa) 10- to 75-fold higher than treatment with control particles (neutral or negatively charged particles). Using TLR4 knockout mice, it was shown that the induction of cytokines and IFN response to cationic liposomes decreased dramatically (58), strengthening the hypothesis suggested by Russchart (106) several years ago that cationic liposomes can agonize TLR4. 193 Peer Manipulating leukocyte function with RNAi PEGylated liposomes, which are mildly negatively charged under physiological conditions (107), have been used extensively as drug delivery carriers. Their advantage in improving circulation time of the entrapped therapeutic payload is well known (108, 109). However, it was observed that when PEGylated liposomes were injected into mice, rats, and rhesus monkeys repeatedly, they lost this long circulation feature and accumulated in the liver, a phenomenon termed accelerated blood clearance (ABC) (110, 111). Ishida et al. (112) suggested a possible mechanism of action for the ABC phenomenon demonstrating an PEG-specific IgM response by splenocytes isolated from animals following the first injection of empty PEGylated liposomes. These antibodies were found to bind to the PEG on a second injected liposome dose, subsequently activating the complement system. An opsonization of liposomes by C3 fragment occurred, which led to an enhanced uptake of the liposomes by specialized macrophages in the liver known as the Kupffer cells (112). The surface charge of the LNPs affects also the tissue specificity of the particle uptake. Macrophages seem to preferentially take up negatively charged LNPs (107, 113, 114). Different malignant cell lines have different uptake patterns with respect to positive, neutral, or negative charges, and in vivo uptake patterns can differ further (114). Anionic liposomes interact with a limited fraction of dendritic cells in vitro, whereas cationic liposomes interact with a high percentage of the dendritic cells, probably by means of electrostatic binding to the negatively charged surface heparane sulfate proteoglycans resulting in intracellular localization (115). 1,2-dioleoyl-sn-glycero-3-phosphatidylcholine (DOPC), a neutral phospholipid-forming liposome, was used to deliver siRNAs payloads in vivo into tumor cells (96, 116–119) 10and 30-fold more effectively than cationic, DOTAP-based liposomes, and naked siRNA, respectively (120). DOPCbased nanoscaled liposomes (approximately 100 nm in diameter) did not induce any detectable toxicity and were found to be safe in orthotopic mouse models, making them highly attractive for further therapeutic development (121). Phagocytic cells fervently take up anionic liposomes via an unclear mechanism. When entrapping siRNAs, the loading efficiency into these liposomes is quite low, probably due to the negative charge of these molecules (6, 30, 114). A complete understanding of the best liposomal design for delivery of therapeutic substances is still evolving. It is possible that with RNAi delivery, the use of a neutral lipid, such as DOPC, which will enter the cells via a mechanism that will not involve endosomes, will allow a balance between efficient uptake of the therapeutic payload into a liposome at preparation, uptake of the liposome into a particular cell type, and the release of the payload from the liposome inside the cell cytoplasm, as was demonstrated for multiple targets using siRNAs entrapped in DOPC-based particles (118, 119, 122). From challenge to cautious optimism Understanding the complicated nature of the immune system with its unique arms can open the door for utilizing different RNAi delivery platforms to manipulate the immune response. In a recent study (123), it was demonstrated that hydrophobicity can dictate the immune response. A small library of gold NPs was synthesized and characterized. These gold NPs had increased hydrophobic carbon chains on their surface and had almost a linear behavior (both in vitro and in vivo) when interacting with subsets of leukocytes. LNPs are one of the most veteran delivery vehicles used already in clinical practice for many years, and several new classes of LNPs including hybrid systems (lipid polymers) are under clinical evaluation with therapeutic and imaging payloads. Adequate and comprehensive understanding of the specific interaction between LNPs with T cells, B cells, dendritic cells, macrophages, and monocytes at the cellular and molecular level and appropriate assays to probe immune suppression or stimulation, such as cytokine induction, interferon response, lymphocyte activation, coagulation cascades, and complement activation, will aid in designing safer vehicles for discovery, validation, and therapeutic applications in leukocytes. The arsenal of RNAi delivery platforms already available for use in leukocytes is increasing, but it will be wise to use next generation sequencing methods and microarrays to globally examine what effects these delivery platforms may have on subsets of leukocytes before we use those strategies to manipulate leukocyte function. References 1. Elbashir SM, Harborth J, Lendeckel W, Yalcin A, Weber K, Tuschl T. Duplexes of 21nucleotide RNAs mediate RNA interference in cultured mammalian cells. Nature 2001;411:494–498. 194 2. Amarzguioui M, Rossi JJ, Kim D. Approaches for chemically synthesized siRNA and vectormediated RNAi. FEBS Lett 2005;579:5974–5981. 3. Dykxhoorn DM, Lieberman J. Knocking down disease with siRNAs. Cell 2006;126:231–235. 4. Sledz CA, Williams BR. RNA interference in biology and disease. Blood 2005;106:787–794. 5. de Fougerolles A, Vornlocher HP, Maraganore J, Lieberman J. Interfering with disease: a progress © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Peer Manipulating leukocyte function with RNAi 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. report on siRNA-based therapeutics. Nat Rev Drug Discov 2007;6:443–453. Peer D, Lieberman J. Special delivery: targeted therapy with small RNAs. Gene Ther 2011;18:1127–1133. Song E, et al. Antibody mediated in vivo delivery of small interfering RNAs via cell-surface receptors. Nat Biotechnol 2005;23:709–717. Peer D, Park EJ, Morishita Y, Carman CV, Shimaoka M. Systemic leukocyte-directed siRNA delivery revealing cyclin D1 as an antiinflammatory target. Science 2008;319:627–630. Palliser D, et al. An siRNA-based microbicide protects mice from lethal herpes simplex virus 2 infection. Nature 2006;439:89–94. Song E, et al. RNA interference targeting Fas protects mice from fulminant hepatitis. Nat Med 2003;9:347–351. Robbins M, et al. Misinterpreting the therapeutic effects of small interfering RNA caused by immune stimulation. Hum Gene Ther 2008;19:991–999. Kleinman ME, et al. Sequence- and targetindependent angiogenesis suppression by siRNA via TLR3. Nature 2008;452:591–597. Weinstein S, et al. RNA inhibition highlights cyclin d1 as a potential therapeutic target for mantle cell lymphoma. PLoS ONE 2012;7: e43343. Daka A, Peer D. RNAi-based nanomedicines for targeted personalized therapy. Adv Drug Deliv Rev 2012;64:1508–1521. Zimmermann TS, et al. RNAi-mediated gene silencing in non-human primates. Nature 2006;441:111–114. Dorn G, et al. siRNA relieves chronic neuropathic pain. Nucleic Acids Res 2004;32:e49. Shen J, et al. Suppression of ocular neovascularization with siRNA targeting VEGF receptor 1. Gene Ther 2006;13:225–234. Filleur S, et al. SiRNA-mediated inhibition of vascular endothelial growth factor severely limits tumor resistance to antiangiogenic thrombospondin-1 and slows tumor vascularization and growth. Cancer Res 2003;63:3919–3922. Gaudilliere B, Shi Y, Bonni A. RNA interference reveals a requirement for myocyte enhancer factor 2A in activity-dependent neuronal survival. J Biol Chem 2002;277:46442–46446. Miller VM, et al. Allele-specific silencing of dominant disease genes. Proc Natl Acad Sci USA 2003;100:7195–7200. Gonzalez-Alegre P, Bode N, Davidson BL, Paulson HL. Silencing primary dystonia: lentiviral-mediated RNA interference therapy for DYT1 dystonia. J Neurosci 2005;25:10502– 10509. Bumcrot D, Manoharan M, Koteliansky V, Sah DW. RNAi therapeutics: a potential new class of pharmaceutical drugs. Nat Chem Biol 2006;2:711–719. Bramsen JB, et al. A large-scale chemical modification screen identifies design rules to generate siRNAs with high activity, high stability and low toxicity. Nucleic Acids Res 2009;37:2867–2881. 24. Robbins M, Judge A, MacLachlan I. siRNA and innate immunity. Oligonucleotides 2009;19:89– 102. 25. Behlke MA. Chemical modification of siRNAs for in vivo use. Oligonucleotides 2008;18:305–319. 26. Dykxhoorn DM, Palliser D, Lieberman J. The silent treatment: siRNAs as small molecule drugs. Gene Ther 2006;13:541–552. 27. Kim DH, Rossi JJ. Strategies for silencing human disease using RNA interference. Nat Rev Genet 2007;8:173–184. 28. Behlke MA. Progress towards in vivo use of siRNAs. Mol Ther 2006;13:644–670. 29. Dykxhoorn DM, Lieberman J. The silent revolution: RNA interference as basic biology, research tool, and therapeutic. Annu Rev Med 2005;56:401–423. 30. Goldsmith M, Mizrahy S, Peer D. Grand challenges in modulating the immune response with RNAi nanomedicines. Nanomedicine 2011;6:1771–1785. 31. Goffinet C, Keppler OT. Efficient nonviral gene delivery into primary lymphocytes from rats and mice. FASEB J 2006;20:500–502. 32. Huang Z, King MR. An immobilized nanoparticle-based platform for efficient gene knockdown of targeted cells in the circulation. Gene Ther 2009;16:1271–1282. 33. Eguchi A, et al. Efficient siRNA delivery into primary cells by a peptide transduction domaindsRNA binding domain fusion protein. Nat Biotechnol 2009;27:567–571. 34. Zhou J, Li H, Li S, Zaia J, Rossi JJ. Novel dual inhibitory function aptamer-siRNA delivery system for HIV-1 therapy. Mol Ther 2008;16:1481–1489. 35. Zhou J, et al. Selection, characterization and application of new RNA HIV gp 120 aptamers for facile delivery of Dicer substrate siRNAs into HIV infected cells. Nucleic Acids Res 2009;37:3094–3109. 36. Kortylewski M, et al. In vivo delivery of siRNA to immune cells by conjugation to a TLR9 agonist enhances antitumor immune responses. Nat Biotechnol 2009;27:925–932. 37. Ishimoto T, et al. Downregulation of monocyte chemoattractant protein-1 involving short interfering RNA attenuates hapten-induced contact hypersensitivity. Mol Ther 2008;16:387– 395. 38. Kumar P, et al. T cell-specific siRNA delivery suppresses HIV-1 infection in humanized mice. Cell 2008;134:577–586. 39. Subramanya S, et al. Targeted delivery of small interfering RNA to human dendritic cells to suppress dengue virus infection and associated proinflammatory cytokine production. J Virol 2010;84:2490–2501. 40. Kim SS, et al. Targeted delivery of siRNA to macrophages for anti-inflammatory treatment. Mol Ther 2010;18:993–1001. 41. Kumar P, et al. Transvascular delivery of small interfering RNA to the central nervous system. Nature 2007;448:39–43. 42. Peer D, Zhu P, Carman CV, Lieberman J, Shimaoka M. Selective gene silencing in activated leukocytes by targeting siRNAs to the integrin © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. lymphocyte function-associated antigen-1. Proc Natl Acad Sci USA 2007;104:4095–4100. Springer TA. Adhesion receptors of the immune system. Nature 1990;346:425–434. Hynes RO. Integrins: bidirectional, allosteric signaling machines. Cell 2002;110:673–687. Lebwohl M, et al. A novel targeted T-cell modulator, efalizumab, for plaque psoriasis. N Engl J Med 2003;349:2004–2013. Sandborn WJ, et al. Natalizumab induction and maintenance therapy for Crohn’s disease. N Engl J Med 2005;353:1912–1925. Shimaoka M, Springer TA. Therapeutic antagonists and conformational regulation of integrin function. Nat Rev Drug Discov 2003;2:703–716. Shimaoka M, et al. Structures of the alpha L I domain and its complex with ICAM-1 reveal a shape-shifting pathway for integrin regulation. Cell 2003;112:99–111. Peer D. Induction of therapeutic gene silencing in leukocyte-implicated diseases by targeted and stabilized nanoparticles: a mini-review. J Control Rel 2010;148:63–68. Fabbri M, et al. Dynamic partitioning into lipid rafts controls the endo-exocytic cycle of the alphaL/beta2 integrin, LFA-1, during leukocyte chemotaxis. Mol Biol Cell 2005;16:5793–5803. Coffey GP, et al. In vitro internalization, intracellular transport, and clearance of an antiCD11a antibody (Raptiva) by human T-cells. J Pharmacol Exp Ther 2004;310:896–904. Springer TA. Traffic signals for lymphocyte recirculation and leukocyte emigration: the multistep paradigm. Cell 1994;76:301–314. Butcher EC, Picker LJ. Lymphocyte homing and homeostasis. Science 1996;272:60–66. Shimaoka M, Takagi J, Springer TA. Conformational regulation of integrin structure and function. Annu Rev Biophys Biomol Struct 2002;31:485–516. Shimaoka M, et al. AL-57, a ligand-mimetic antibody to integrin LFA-1, reveals chemokineinduced affinity up-regulation in lymphocytes. Proc Natl Acad Sci USA 2006;103:13991–13996. Ben-Arie N, Kedmi R, Peer D. Integrin-targeted nanoparticles for siRNA delivery. Methods Mol Biol 2012;757:497–507. Kim SS, et al. RNAi-mediated CCR5 silencing by LFA-1-targeted nanoparticles prevents HIV infection in BLT mice. Mol Ther 2010;18:370– 376. Kedmi R, Ben-Arie N, Peer D. The systemic toxicity of positively charged lipid nanoparticles and the role of Toll-like receptor 4 in immune activation. Biomaterials 2010;31:6867–6875. Peer D. Immunotoxicity derived from manipulating leukocytes with lipid-based nanoparticles. Adv Drug Deliv Rev 2012;64:1738–1748. Landesman-Milo D, Peer D. Altering the immune response with lipid-based nanoparticles. J Control Rel 2012;161:600–608. Peer D, Florentin A, Margalit R. Hyaluronan is a key component in cryoprotection and formulation of targeted unilamellar liposomes. Biochim Biophys Acta 2003;1612:76–82. 195 Peer Manipulating leukocyte function with RNAi 62. Peer D, Margalit R. Loading mitomycin C inside long circulating hyaluronan targeted nanoliposomes increases its antitumor activity in three mice tumor models. Int J Cancer 2004;108:780– 789. 63. Peer D, Margalit R. Tumor-targeted hyaluronan nanoliposomes increase the antitumor activity of liposomal Doxorubicin in syngeneic and human xenograft mouse tumor models. Neoplasia 2004;6:343–353. 64. Mizrahy S, Peer D. Polysaccharides as building blocks for nanotherapeutics. Chem Soc Rev 2012;41:2623–2640. 65. Mizrahy S, et al. Hyaluronan-coated nanoparticles: the influence of the molecular weight on CD44-hyaluronan interactions and on the immune response. J Control Rel 2011;156:231–238. 66. Stacey DW. Cyclin D1 serves as a cell cycle regulatory switch in actively proliferating cells. Curr Opin Cell Biol 2003;15:158–163. 67. Lee YM, Sicinski P. Targeting cyclins and cyclindependent kinases in cancer: lessons from mice, hopes for therapeutic applications in human. Cell Cycle 2006;5:2110–2114. 68. Knudsen KE, Diehl JA, Haiman CA, Knudsen ES. Cyclin D1: polymorphism, aberrant splicing and cancer risk. Oncogene 2006;25:1620–1628. 69. Fu M, Wang C, Li Z, Sakamaki T, Pestell RG. Minireview: Cyclin D1: normal and abnormal functions. Endocrinology 2004;145:5439–5447. 70. Tashiro E, Tsuchiya A, Imoto M. Functions of cyclin D1 as an oncogene and regulation of cyclin D1 expression. Cancer Sci 2007;98:629– 635. 71. Kozar K, Sicinski P. Cell cycle progression without cyclin D-CDK4 and cyclin D-CDK6 complexes. Cell Cycle 2005;4:388–391. 72. Jing N, Tweardy DJ. Targeting Stat3 in cancer therapy. Anticancer Drugs 2005;16:601–607. 73. Arnold A, Papanikolaou A. Cyclin D1 in breast cancer pathogenesis. J Clin Oncol 2005;23:4215–4224. 74. Jares P, Colomer D, Campo E. Genetic and molecular pathogenesis of mantle cell lymphoma: perspectives for new targeted therapeutics. Nat Rev Cancer 2007;7:750–762. 75. Hunter T, Pines J. Cyclins and cancer. II: Cyclin D and CDK inhibitors come of age. Cell 1994;79:573–582. 76. Sherr CJ. Cancer cell cycles. Science 1996;274:1672–1677. 77. Sherr CJ, McCormick F. The RB and p53 pathways in cancer. Cancer Cell 2002;2:103– 112. 78. Fernandez V, Hartmann E, Ott G, Campo E, Rosenwald A. Pathogenesis of mantle-cell lymphoma: all oncogenic roads lead to dysregulation of cell cycle and DNA damage response pathways. J Clin Oncol 2005;23:6364– 6369. 79. Kim SS, Subramanya S, Peer D, Shimaoka M, Shankar P. Antibody-mediated delivery of siRNAs for anti-HIV therapy. Methods Mol Biol 2011;721:339–353. 80. Szoka F. Molecular biology. The art of assembly. Science 2008;319:578–579. 196 81. Maclachlan I. siRNAs with guts. Nat Biotechnol 2008;26:403–405. 82. Bachar G, et al. Hyaluronan-grafted particle clusters loaded with Mitomycin C as selective nanovectors for primary head and neck cancers. Biomaterials 2011;32:4840–4848. 83. Landesman-Milo D, et al. Hyaluronan grafted lipid-based nanoparticles as RNAi carriers for cancer cells. Cancer Lett 2012. doi: 10.1016/j. canlet.2012.08.024. 84. Agrawal S, Kandimalla ER. Antisense and siRNA as agonists of Toll-like receptors. Nat Biotechnol 2004;22:1533–1537. 85. Kariko K, Bhuyan P, Capodici J, Weissman D. Small interfering RNAs mediate sequenceindependent gene suppression and induce immune activation by signaling through toll-like receptor 3. J Immunol 2004;172:6545–6549. 86. Sledz CA, Holko M, de Veer MJ, Silverman RH, Williams BR. Activation of the interferon system by short-interfering RNAs. Nat Cell Biol 2003;5:834–839. 87. Judge AD, Sood V, Shaw JR, Fang D, McClintock K, MacLachlan I. Sequence-dependent stimulation of the mammalian innate immune response by synthetic siRNA. Nat Biotechnol 2005;23:457–462. 88. Hornung V, et al. Sequence-specific potent induction of IFN-alpha by short interfering RNA in plasmacytoid dendritic cells through TLR7. Nat Med 2005;11:263–270. 89. Forsbach A, et al. Identification of RNA sequence motifs stimulating sequence-specific TLR8dependent immune responses. J Immunol 2008;180:3729–3738. 90. Sioud M. Induction of inflammatory cytokines and interferon responses by double-stranded and single-stranded siRNAs is sequence-dependent and requires endosomal localization. J Mol Biol 2005;348:1079–1090. 91. Schlee M, Hornung V, Hartmann G. siRNA and isRNA: two edges of one sword. Mol Ther 2006;14:463–470. 92. Robbins M, Judge A, Liang L, McClintock K, Yaworski E, MacLachlan I. 2′-O-methyl-modified RNAs act as TLR7 antagonists. Mol Ther 2007;15:1663–1669. 93. Puthenveetil S, Whitby L, Ren J, Kelnar K, Krebs JF, Beal PA. Controlling activation of the RNAdependent protein kinase by siRNAs using sitespecific chemical modification. Nucl Acids Res 2006;34:4900–4911. 94. Judge AD, Bola G, Lee AC, MacLachlan I. Design of noninflammatory synthetic siRNA mediating potent gene silencing in vivo. Mol Ther 2006;13:494–505. 95. Morrissey DV, et al. Potent and persistent in vivo anti-HBV activity of chemically modified siRNAs. Nat Biotechnol 2005;23:1002–1007. 96. Ozpolat B, Sood AK, Lopez-Berestein G. Nanomedicine based approaches for the delivery of siRNA in cancer. J Intern Med 2010;267:44–53. 97. Christensen D, Korsholm KS, Rosenkrands I, Lindenstrom T, Andersen P, Agger EM. Cationic liposomes as vaccine adjuvants. Expert Rev Vaccines 2007;6:785–796. 98. Buyens K, et al. Liposome based systems for systemic siRNA delivery: Stability in blood sets the requirements for optimal carrier design. J Control Rel 2012;158:362–370. 99. Shirazi RS, Ewert KK, Leal C, Majzoub RN, Bouxsein NF, Safinya CR. Synthesis and characterization of degradable multivalent cationic lipids with disulfide-bond spacers for gene delivery. Biochim Biophys Acta 2011;1808:2156–2166. 100. Akinc A, et al. A combinatorial library of lipidlike materials for delivery of RNAi therapeutics. Nat Biotechnol 2008;26:561–569. 101. Nakanishi T, et al. Positively charged liposome functions as an efficient immunoadjuvant in inducing immune responses to soluble proteins. Biochem Biophys Res Commun 1997;240:793– 797. 102. Vangasseri DP, Cui Z, Chen W, Hokey DA, Falo LD Jr, Huang L. Immunostimulation of dendritic cells by cationic liposomes. Mol Membr Biol 2006;23:385–395. 103. Chen Y, Bathula SR, Li J, Huang L. Multifunctional nanoparticles delivering small interfering RNA and doxorubicin overcome drug resistance in cancer. J Biol Chem 2010;285:22639–22650. 104. Spagnou S, Miller AD, Keller M. Lipidic carriers of siRNA: differences in the formulation, cellular uptake, and delivery with plasmid DNA. Biochemistry 2004;43:13348–13356. 105. Solmesky LJ, Shuman M, Goldsmith M, Weil M, Peer D. Assessing cellular toxicities in fibroblasts upon exposure to lipid-based nanoparticles: a high content analysis approach. Nanotechnology 2011;22:494016. 106. Lonez C, Vandenbranden M, Ruysschaert JM. Cationic liposomal lipids: from gene carriers to cell signaling. Prog Lipid Res 2008;47:340–347. 107. Harel-Adar T, Ben Mordechai T, Amsalem Y, Feinberg MS, Leor J, Cohen S. Modulation of cardiac macrophages by phosphatidylserinepresenting liposomes improves infarct repair. Proc Natl Acad Sci USA 2011;108:1827–1832. 108. Allen TM, Hansen C, Martin F, Redemann C, Yau-Young A. Liposomes containing synthetic lipid derivatives of poly(ethylene glycol) show prolonged circulation half-lives in vivo. Biochim Biophys Acta 1991;1066:29–36. 109. Klibanov AL, Maruyama K, Torchilin VP, Huang L. Amphipathic polyethyleneglycols effectively prolong the circulation time of liposomes. FEBS Lett 1990;268:235–237. 110. Ishida T, Maeda R, Ichihara M, Irimura K, Kiwada H. Accelerated clearance of PEGylated liposomes in rats after repeated injections. J Control Rel 2003;88:35–42. 111. Ishida T, Masuda K, Ichikawa T, Ichihara M, Irimura K, Kiwada H. Accelerated clearance of a second injection of PEGylated liposomes in mice. Int J Pharm 2003;255:167–174. 112. Ishida T, Wang X, Shimizu T, Nawata K, Kiwada H. PEGylated liposomes elicit an anti-PEG IgM response in a T cell-independent manner. J Control Rel 2007;122:349–355. 113. Gutman D, Epstein-Barash H, Tsuriel M, Golomb G. Alendronate liposomes for antitumor therapy: © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 Peer Manipulating leukocyte function with RNAi activation of gammadelta T Cells and inhibition of tumor growth. Adv Exp Med Biol 2012;733:165–179. 114. Miller CR, Bondurant B, McLean SD, McGovern KA, O’Brien DF. Liposome-cell interactions in vitro: effect of liposome surface charge on the binding and endocytosis of conventional and sterically stabilized liposomes. Biochemistry 1998;37:12875–12883. 115. Foged C, Arigita C, Sundblad A, Jiskoot W, Storm G, Frokjaer S. Interaction of dendritic cells with antigen-containing liposomes: effect of bilayer composition. Vaccine 2004;22:1903–1913. 116. Gray MJ, et al. Therapeutic targeting of neuropilin-2 on colorectal carcinoma cells implanted in the murine liver. J Natl Cancer Inst 2008;100:109–120. 117. Halder J, et al. Focal adhesion kinase targeting using in vivo short interfering RNA delivery in neutral liposomes for ovarian carcinoma therapy. Clin Cancer Res 2006;12:4916–4924. 118. Landen CN Jr, et al. Therapeutic EphA2 gene targeting in vivo using neutral liposomal small interfering RNA delivery. Cancer Res 2005;65:6910–6918. 119. Merritt WM, et al. Effect of interleukin-8 gene silencing with liposome-encapsulated small interfering RNA on ovarian cancer cell growth. J Natl Cancer Inst 2008;100:359– 372. 120. Gewirtz AM. On future’s doorstep: RNA interference and the pharmacopeia of tomorrow. J Clin Invest 2007;117:3612–3614. © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd Immunological Reviews 253/2013 121. Tanaka T, et al. Sustained small interfering RNA delivery by mesoporous silicon particles. Cancer Res 2010;70:3687–3696. 122. Villares GJ, et al. Targeting melanoma growth and metastasis with systemic delivery of liposome-incorporated protease-activated receptor-1 small interfering RNA. Cancer Res 2008;68:9078–9086. 123. Moyano DF, et al. Nanoparticle hydrophobicity dictates immune response. J Am Chem Soc 2012;134:3965–3967. 124. Salas A, Shimaoka M, Kogan AN, Harwood C, von Andrian UH, Springer TA. Rolling adhesion through an extended conformation of integrin alphaLbeta2 and relation to alpha I and beta Ilike domain interaction. Immunity 2004;20:393– 406. 197