Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Childhood immunizations in the United States wikipedia , lookup
Atherosclerosis wikipedia , lookup
Germ theory of disease wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Globalization and disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Behçet's disease wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Periodontal disease wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Schistosomiasis wikipedia , lookup
Autoimmunity wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Rheumatic fever wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Infection control wikipedia , lookup
Inflammatory bowel disease wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Innate immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Inflammation wikipedia , lookup
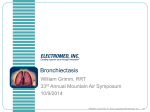
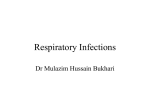
Chapter 3 Histopathology of bronchiectasis M. Goddard HISTOPATHOLOGY Summary The clinical presentation of bronchiectasis occurs after initial irreversible damage to the airway has occurred. The clinician then has to control symptoms and limit the progression of the disease. A clearer understanding of the pathogenesis of this disease will enable the development of better treatment strategies. Bronchiectasis is a multi-factorial disease process in which there are a number of key steps, although they are not always clinically identifiable. There is often an initiator or damaging event such as a viral infection which, in an individual with a predisposing risk such as a degree of immune dysfunction or an impaired mucociliary clearance system, leads to persistent and damaging bacterial infections. These infections go on to provoke an inappropriate and self-damaging inflammatory response in which neutrophil activity leads to progressive tissue damage and a relentless cycle of infection, inflammation and bronchial wall injury. Persistent infection and chronic inflammatory cell infiltration further amplify the local inflammatory milieu and may lead to systemic complications. Keywords: Aetiology, bronchiectasis, histopathology, inflammation, neutrophils, pathogenesis Correspondence: M. Goddard, Dept of Pathology, Papworh Hospital NHS Foundation Trust, Papworth Everard, Cambridge, CB23 3RE, UK, Email [email protected] Eur Respir Mon 2011. 52, 22–31. Printed in UK – all rights reserved. Copyright ERS 2011. European Respiratory Monograph; ISSN: 1025-448x. DOI: 10.1183/1025448x.10003310 B ronchiectasis was first described at the beginning of the 19th century by LAENNEC [1]. He ascribed the term to the pooling of secretions in the airways leading to wall weakening and dilatation. Whilst the term is often used loosely by radiologists to describe any airway dilatation, pathologically the term is used to describe an irreversible dilatation of the airway often associated with chronic suppuration. Aetiology and classification Aetiologically, bronchiectasis may be divided into obstructive and nonobstructive types (table 1). 22 In the obstructive type of bronchiectasis airway dilation may develop from obstruction due to any cause. The disease is confined to the airways distal to the obstruction. Causes of obstruction may be luminal, such as the inhalation of foreign bodies. This is most common in children and shows a The pathogenesis of obstructive bronchiectasis is relatively straightforward, as bronchial secretions accumulate distal to the obstruction and become infected producing inflammation and damage to the bronchial wall which becomes weakened and dilated. This was recognised by LAENNEC [1]. Table 1. Causes of bronchiectasis Bronchial obstruction Foreign bodies Tumours Carcinoid tumours Endobronchial chondromas and lipomas Mucous plugs ABPA Nonobstructive Post-infective Measles Adenovirus Pertussis Tuberculosis Mucociliary abnormalities Cystic fibrosis Ciliary dysmotility syndromes Primary ciliary dyskinesia Immunological abnormalities Hypogammaglobulinaemia IgA and IgG sub-class deficiencies Neutrophil function abnormalities Ataxia telangiectasia Associated with systemic diseases Rheumatoid arthritis Sjögren’s syndrome Ankylosing spondylitis a1-antitrypsin deficiency Pulmonary fibrosis ABPA: allergic bronchopulmonary aspergillosis; There have been several attempts to classify nonIg: immunoglobulin. obstructive bronchiectasis, which are variably based on a mixture of historic bronchographic and, more recently, high-resolution computed tomography (HRCT), appearances (saccular or cystic, fusiform or cylindric) [10] and histological appearances (follicular) with lymphoid follicles in the wall, as defined by WHITWELL [11]. Nonobstructive bronchiectasis is typically more widespread, affecting more than one lobe and most commonly affecting the basal segments of the lower lobes [11–13]. The left lung is more frequently affected than the right and the disease process typically involves the middle-order bronchi (fourth to ninth generations). M. GODDARD predilection for the right lower lobe and posterior segment of the right upper lobe [2–5]. The risk of developing bronchiectasis following foreign body inhalation has been assessed as 3–16% [6]. However, other causes of obstruction include mucus inspissation in allergic bronchopulmonary aspergillosis (ABPA) [7], with central or upper lobe bronchiectasis, and distal to broncholitis. Tumours may also cause obstruction and bronchiectasis but this is more prevalent in the slower growing often polypoid tumours, such as carcinoid tumours, endobronchial lipomas and chondromas [8]. Extrinsic compression of the bronchus may also lead to obstruction, and typically hilar tuberculous lymphadenopathy can lead to bronchiectasis, particularly of the right middle and lower lobes. The middle lobe, because of its relatively narrow lumen, is at particular risk of compression or obstruction, a condition sometimes referred to as middle lobe syndrome [9]. 23 This classification is now probably unsatisfactory and of little pathological significance; although the distribution of changes may provide a clue to the underlying aetiology. Post-infective bronchiectasis is traditionally the most common underlying cause, is most often basal and may be confined to a single lobe. However, nonobstructive bronchiectasis may occur in association with a number of other conditions. In diseases where mucociliary clearance is impaired, bronchiectasis frequently, if not inevitably, develops. In cystic fibrosis [14] and ciliary dysmotility syndromes, such as primary ciliary dyskinesia arising from a defect in the dynein arms [15], bronchiectais is more widespread, sometimes with upper lobe predominance. The association of bronchiectasis with disturbances in mucociliary clearance mechanisms highlights the importance of local defence mechanisms within the airways in aetiological terms and in terms of the pathogenesis of the disease. There may be primary defects in the immune system with abnormalities of neutrophil function, hypogammaglobulinaemia [16], immunoglobulin (Ig)A and IgG sub-class deficiencies [17], and in ataxia telangiectasia. Bronchiectasis may also be associated with some autoimmune conditions including ulcerative colitis [18], rheumatoid disease [19], Sjögren’s syndrome [20] and ankylosing spondylitis. Bronchiectasis is also associated with several noninflammatory conditions within the lung, such as a1-antitrypsin deficiency, and is reported in some cases of pulmonary fibrosis but in these cases may be due to traction effects of the surrounding fibrosis. Of the known causes or associations of bronchiectasis, childhood infection is probably the most common accounting for up to 30% of cases, with immunodeficiencies present in up to 18%. However, in some studies, no underlying abnormality can be detected in .50% of cases. Histopathological appearances Histopathologically, bronchiectatic airways appear dilated and on examination have a crosssectional area that is much larger than the accompanying pulmonary artery (fig. 1). The airway lumen is often filled with a mucopurulent exudate with neutrophils and macrophages (figs 2 and 3). The respiratory epithelium lining shows variable changes from a reserve cell hyperplasia to squamous metaplasia (fig. 4) with active inflammation shown by epithelial and mucosal infiltration by neutrophils and in severe exacerbations, ulceration (figs 5 and 6). The bronchial wall is often destroyed due to loss of fibromuscular tissues and the elastic framework, and may show erosion and loss of cartilage [21]. There is usually a reduction in submucosal glands. The wall may be thin but is more often greatly thickened with extensive peribronchial fibrosis extending into the adjacent lung parenchyma (fig. 7) [22]. There is an associated chronic inflammatory cell infiltrate within the wall, predominantly lymphocytes and plasma cells, and in some cases lymphoid follicles with germinal centres may be prominent [23]. The presence of B-cell immune activation through the presence of germinal centres and plasma cells in the walls of bronchiectatic airways, would support the role of antibodies in the immune response to persistent infection. However, bronchiectasis is associated with some autoimmune connective tissue diseases, in particular rheumatoid arthritis [19, 24, 25], and a role for autoimmunity in the destruction of the airway has also been suggested. HISTOPATHOLOGY Eosinophils may be seen as part of the infiltrate as with any chronic airways inflammation. Whilst nonspecific, they raise the possibility of an associated fungal infection such as Aspergillus. Although eosinophils are commonly seen in the mucus plugs of ABPA, their presence within the airway wall inflammation is nonspecific. Granulomas and multinucleate giant cells may be seen in the wall and might be a reaction to the inspissated luminal material but the possibility of concomitant fungal or mycobacterial infection should always be considered. In established bronchiectasis, the histological pattern of chronic inflammation within the airway wall with superimposed active inflammation, most likely reacting to concomitant infection, has a fairly uniform appearance and provides little insight into the underlying aetiology or pathogenesis. 24 Figure 1. Low-power view of a bronchiectatic airway; note the airway lumen is much larger than that of the accompanying pulmonary artery. Magnification64. The surrounding lung parenchyma may show a number of changes. Where there is distal luminal obliteration of bronchi and bronchioles, the lung parenchyma may The airways are supplied by the bronchial arteries and the inflammatory destruction and healing processes result in the formation of bronchopulmonary anastamoses, probably due to a mixture of new vessel formation and the re-opening of pre-existing, pre-capillary bronchopulmonary connections (fig. 8). Ulceration of the airways can lead to severe haemorrhage and haemoptysis. The formation of anastamoses and the loss of some of the alveolar capillary bed leads to the development of pulmonary hypertension [27]. Figure 2. Bronchiectatic airway wall with dense chronic inflammatory cell infiltrate, which includes lymphocytes, plasma cells and eosinophils. Magnification620. M. GODDARD show atelectasis due to absorption and collapse. Obliterative changes in small airways are important in contributing to airflow obstruction in bronchiectasis [10, 11]. Destructive inflammation may lead to the formation of an abscess cavity, although this may be difficult to distinguish from a distended, ulcerated airway. There may be accompanying interstitial pneumonitis, particularly in cases of follicular bronchiectasis, and also changes of an organising pneumonia. Small airway changes, such as bronchiolectasis, may be seen as part of the whole disease process or may be part of an underlying disease leading to more proximal dilatation, as has been seen with small airways disease, such as bronchiolitis [18, 26]. Focal proliferations of neuroendocrine cells are also seen and may lead to the formation of multiple tumourlets, small aggregates of neuroendocrine cells in the walls of small airways. These are not specific to bronchiectasis and may be seen in a number of chronic lung conditions [28]. Figure 3. Bronchiectatic airway wall with luminal pus, neutrophil infiltration of the airway epithelium and a dense chronic inflammatory cell infiltrate. Magnification640. 25 It has also been recognised that the persistent chronic activation of the immune system in the wall of the airway may lead to the development of bronchus-associated lymphoid tissue (BALT), especially in bronchiectasis associated with Sjögren’s syndrome [29]. Increased incidence of BALTomas, low-grade, B-cell lymphomas, is associated with Sjögren’s syndrome but not specifically related to bronchiectasis [20]. In chronic disease, further complications may arise. Locally, the lung may develop abscesses and even empyema, although this is less common as the pleural space is often obliterated by fibrous adhesions. Bronchiectatic spaces may become colonised by saprophytic fungi, most commonly Aspergillus sp. HISTOPATHOLOGY Systemic dissemination of infection may lead to abscesses in other organs, notably the brain, and chronic suppuration may be complicated by systemic amyloidosis (type AA). The incidence in bronchiectasis is unclear but in one study of patients with systemic amyloidosis requiring haemodialysis, 40% had underlying bronchiectasis [30]. Figure 4. Squamous metaplasia of the epithelium lining in bronchiectasis. Magnification640. Pathogenesis The pathogenesis of bronchiectasis is complex and a number of different mechanisms contribute to the development of a similar morphological appearance and different factors act together to set up a cycle of inflammation and destruction that leads to damage and destruction of the bronchial wall [31]. The initiator to this sequence is usually damage to the bronchial epithelium. This may be due to an external insult or to an intrinsic deficiency within the patient. The most common predisposing factor to the development of bronchiectasis is a severe childhood respiratory infection, which may be viral, such as measles or adenovirus, or bacterial, such as Bordetella pertussis [32–34]. The resultant permanent dilatation of the airways is thought to be due not only to inflammation and destruction of the bronchial wall but also, in part, to a traction effect produced by collapse of the surrounding lung parenchyma. However, the persistence of infection and inflammation are of paramount importance in the progression of the disease. Figure 5. Severely inflamed ulcerated bronchiectatic airway with 26 no epithelium and surface granulation tissue. Magnification620. Whilst an underlying cause is not established in all cases, the number and type of associations for bronchiectasis gives us some indication of what the important underlying pathogenetic mechanisms may be. In post-infectious causes, the initiating viral infection appears to be transitory and, in the case of adenoviruises, it has not been possible to demonstrate the persistence of the virus within bronchiectasis by in situ hybridisation [35]. However, some respiratory viruses have been shown to lead to abnormalities in ciliary function, which may persist for several weeks [36]. In the early stages of bronchiectasis, the most common bacterial isolate is Haemophilus influenzae, which has the capacity to directly damage the airway epithelium and induce the production of inflammatory mediators [37]. The typical immune response to H. influenzae is a T-helper (Th)1 response. However, some bronchiectasis patients with persistent infection have been found to have a Th2 response with a cytokine profile of interleukin (IL)-4 and IL-10. The release of cytokines contributes to the inflammatory response within the airway and at the same time may also result in a failure of the response to satisfactorily remove the organism [38]. Figure 7. A bronchiectatic airway showing an attenuated inflamed epithelium with surrounding inflammation and fibrosis extending into the peribronchial lung parenchyma. Magnification620. 27 Over time, a number of other organisms have been found to be established within the airways, particularly Streptococcus pneumoniae and Pseudomonas aeruginosa. The initial damage to the epithelium lining allows this secondary bacterial colonisation to occur, which further inhibits ciliary clearance and promotes the persistence of infection and damaging inflammation [39]. The importance of this persistence in bacterial colonisation may be related to the production of heatlabile products by the bacteria, which further damage ciliated cells and inhibit ciliary activity. P. aeruginosa can be a particular problem as it is protected from cellular and humoral attack because it survives in a biofilm on the mucosal surface [40]. Pseudomonas has been shown M. GODDARD Clinically, it is the recurrence and persistence of bacterial infections in the airways with which most patients present that are of most importance and are linked to the progression of the disease. There is a Figure 6. Ulcerated airway with surrounding fibrosis of the wall. prevailing view that bacterial infecMagnification610. tion in the lower respiratory tract provokes an exaggerated and uncontrolled neutrophilic response and that the complex interplay between bacterial infection and airway inflammation, along with the release of tissue damaging substances, leads to the progressive damage which typifies bronchiectasis. to produce phenazine pigments that can inhibit ciliary action through a mechanism which leads to a reduction in cellular cAMP and ATP. Furthermore, pseudomonal pyocyanin can lead to epithelial disruption and rhamnolipids have a ciliostatic effect [41, 42]. Alveolar macrophages are an important mediator of defence against Pseudomonas and stimulated macrophages secrete cytokines that both recruit and activate neutrophils, thus potentially amplifying both the inflammatory response and the potential for further tissue damage [43, 44]. The resultant inflammatory reaction is an important pathogenic mechanwall. Magnification620. ism in the weakening of the bronchial wall. Much of the damage appears to relate to the release of proteolytic enzymes and oxygen free radicals from neutrophils. The severity of an inflammatory response is dependent on the interplay of several cytokines, which may be both pro- and anti-inflammatory [45]. In a well-regulated system, the inflammatory cascade is proportionate to the triggering bacterial stimulation and is switched off. There is evidence that in bronchiectasis the inflammatory response is disproportionate to the infective burden and that the inflammatory response persists [43, 46]. Indeed, in the early phases of bronchiectasis, active airway inflammation has even been reported in the absence of identifiable microbial infection, suggesting a dysregulation of the cytokine network independent of infection [47]. HISTOPATHOLOGY Figure 8. Thick-walled bronchial artery in a bronchiecatic airway Neutrophils are potent effectors in inflammatory responses and secrete anti-microbial substances, as well as reactive oxygen free radicals [48]. Bronchoalveolar lavage (BAL) studies have demonstrated that neutrophils are consistently present in patients with bronchiectasis, even when sterile and clinically stable, but increase in the presence of potential pathogens [49, 50]. Recruitment and migration of neutrophils in airways is facilitated by the activation of neutrophils and the upregulation of adhesion molecules on endothelial cells [51–53]. These changes are regulated by cytokines, particularly IL-1 and tumour necrosis factor (TNF)-a, as well as lipopolysaccharide (LPS), which have been shown to be increased in the airways of patients with bronchiectasis [54, 55]. Activated neutrophils secrete potentially tissue damaging enzymes such as neutrophil elastase, proteinase 3 and metalloproteinases. Levels of these enzymes in BAL samples have been shown to correlate with neutrophil numbers and markers of disease activity such as 24hour sputum production [56]. These enzymes can directly damage the structural integrity of the airway via damage to the basement membrane and elastin framework [57–60]. Neutrophils are also an important source of oxygen free radicals. Release of oxygen free radicals are an important part of the defence against infection and are regulated by a protective anti-oxidant system. However, the excessive release of these oxidants can overwhelm the defence mechanisms and cause tissue damage via lipid peroxidation. Furthermore, reactive oxygen species may amplify the inflammatory response through the induction of cytokine and chemokine production by the stimulation of genes regulated by nuclear factor-kB. Studies in bronchiectatic patients have shown increased levels of exhaled H2O2 correlating with neutrophil counts and disease activity [61, 62]. 28 Macrophages also play a role in the disease progression as they secrete TNF-a, which promotes neutrophil recruitment, as well as other inflammatory mediators including IL-8, monocyte chemotactic protein-1 and chemokines [23, 63]. Lymphocytes are also typically present in bronchial biopsies within the lamina propria and may also infiltrate the overlying epithelium. Studies assessing the relative proportions of CD4+ and CD8+ have produced mixed and, at times, conflicting results. Nonetheless, their presence indicates a cell-mediated immune response contributing to the overall inflammatory process [22]. Whilst the epithelial layer may be seen as a protective barrier through mucociliary clearance and generation of anti-bacterial substances, it also contributes to the inflammatory process through the direct generation of pro-inflammatory cytokines [64]. Exposure to LPS leads to the generation of IL-8 and TNF-a which, as stated previously, are important in neutrophil recruitment. Bronchial epithelial cells are also able to upregulate surface adhesion molecules, such as intracellular adhesion molecule-1, aiding the migration of neutrophils [65, 66]. Thus, a number of pathways lead to the activation and recruitment of neutrophils into the airways which, if not adequately regulated and controlled, results in the destruction of local tissue and the persistence and progression of bronchiectasis. Individual variability in this innate response may help to explain why not all individuals exposed to predisposing triggers will go on to develop bronchiectasis and offers potential targets for therapeutic intervention. Statement of interest None declared. 29 1. Laennec RTH. De l’Auscultation Mediatle ou Traite du Diagnostic des Maladies des Poumons et du Couer. [On Mediate Auscultation or Treatise on the Diagnosis of the Lungs and Heart.] Paris, Brosson and Claude, 1819. 2. Weissberg D, Schwartz T. Foreign bodies in the tracheobronchial tree. Chest 1987; 91: 730–733. 3. Limper AH, Prakash UB. Tracheobronchial foreign bodies in adults. Ann Intern Med 1990; 112: 604–609. 4. Scala R, Aronne D, Palumbo U, et al. Prevalence, age, distribution and aetiology of bronchiectasis: a retrospective study on 144 symptomatic patients. Monaldi Arch Chest Dis 2000; 55: 101–105. 5. Tsao PC, Lin CY. Clinical spectrum of bronchiectasis in children. Act Paeditr Taiwan 2002; 43: 271–275. 6. Barker AF, Bardana EJ. Bronchiectasis: update of an orphan disease. Am Rev Respir Dis 1988; 137: 969–978. 7. Bosten C, Myer J, Greenberger P, et al. Pathologic features of allergic bronchopulmonary aspergillosis. Am J Surg Pathol 1988; 12: 216–222. 8. Box K, Kerr KM, Jefferey RR, et al. Endobronchial lipoma associated with lobar bronchiectasis. Repsir Med 1991; 85: 71–72. 9. Kwon KY, Myers JL, Swensen SJ, et al. Middle lobe syndrome: a clinicopathological study of 21 patients. Hum Pathol 1995; 26: 302–307. 10. Reid LM. Reductions in bronchial subdivisions in bronchiectasis. Thorax 1950; 5: 223–247. 11. Whitwell F. A study of the pathology and pathogenesis of bronchiectasis. Thorax 1952; 7: 213–239. 12. Ogilvie AG. The natural history of bronchiectasis. A clinical, roentgenologic and pathologic study. Arch Intern Med 1941; 68: 395–465. 13. Percy KMA, King DC. Bronchiectasis: A study of prognosis based on a follow-up of 400 cases. Am Rev Tuber 1940; 41: 531–548. 14. Ogninc G, Kampalath B, Tomashefski JF. Destruction and loss of bronchial cartilage in cystic fibrosis. Hum Pathol 19888, 29: 65–73. 15. Rossman CM, Forrest JB, Lee RM, et al. The dyskinetic cilia syndrome. Ciliary motility in immotile cilia syndrome. Chest 1980; 78: 580–582. 16. Watts WJ, Watts MD, Dai W, et al. Respiratory dysfunction in patients with common variable hypogammaglobulinaemia. Am Rev Respir Dis 1986; 134: 699–703. 17. Gracia JD, Rodrigo MJ, Morrell F, et al. IgG subclass deficiencies associated with bronchiectasis. Am J Respir Crit Care Med 1996; 153: 650–655. 18. Butland RJ, Cole P, Citron KM, et al. Chronic bronchial suppuration and inflammatory bowel disease. Q J Med 1981; 50: 63–75. 19. Tahanami I, Imamuma T, Yamamoto Y, et al. Bronchiectasis complicating rheumatoid arthritis. Respir Med 1995; 89: 453–454. 20. Strimlan CV, Rosenow EC, Diverite MB, et al. Pulmonary manifestations of Sjogren’s syndrome. Chest 1976; 70: 354–361. 21. Hayward J, Reid ML. The cartilage of intra-pulmonary bronchi in normal lungs, in bronchiectasis and in massive collapse. Thorax 1952; 7: 98–110. M. GODDARD References HISTOPATHOLOGY 30 22. Silva JR, Jones JA, Cole PJ, et al. The immunological component of the cellular inflammatory infiltrate in bronchiecatsis. Thorax 1989; 44: 668–673. 23. Gaga M, Bentley AM, Humbert M, et al. Increases in CD4+ T lymphocytes, macrophages, neutrophils and interleukin 8 positive cells in the airways of patients with bronchiectasis. Thorax 1998; 53: 685–691. 24. Solanki E, Neville E. Bronchiectasis and rheumatoid disease. Is there an association? Br J Rheumatol 1992; 31: 691–693. 25. Mahon MJ, Swinson DR, Shettar S, et al. Bronchiectasis and rheumatoid arthritis: a clinical study. Ann Rheum Dis 1993; 52: 776–779. 26. Moles KM, VArjhess G, Hayes JR. Pulmonary involvement in ulcerative colitis. Br J Dis Chest 1988; 82: 79–83. 27. Liebow AA, Hales MR, Linskog GE. Enlargement of the bronchial arteries and their anastomoses with the pulmonary arteries in bronchiectasis. Am J Pathol 1949; 25: 211–231. 28. Whitwell F. Tumourlets of lung. J Pathol Bact 1955; 70: 529–541. 29. Yousem SA, Colby TV, Carrington CB. Follicular bronchitis/bronchiolitis. Hum Pathol 1985; 16: 700–706. 30. Akcay S, Akman B, Ozdemir H, et al. Bronchiectasis related amyloidosis as a cause of chronic renal failure. Ren Fail 2002; 24: 815–823. 31. Cole PJ. Inflammation: a two edged sword – the model of bronchiectasis. Eur J Respir Dis Suppl 1986; 147: 6–15. 32. Warne WP. Factors causing bronchiectasis. JAMA 1935; 105: 1666–1670. 33. Glauser EM, Cook CD, Harris GBC. Bronchiectasis: a review of 187 cases. Acta Pediatr Scand 1966; 165: 1–15. 34. Whooping cough in the United States and Britain. N Engl J Med 1983; 309: 108–109. 35. Hogg JC, Irving WL, Porter H, et al. In situ hybridisation studies of adenoviral infections of the lung and their relationship to follicular bronchiectasis. Am Rev Respir Dis 1989; 139: 1531–1535. 36. Rayner CFJ, Rutman A, Dewar A, et al. Ciliary disorientation in patients with chronic reparatory tract inflammation. Am J Respir Crit Care Med 1995; 151: 800–804. 37. Starner TD, Zhang N, Kim G, et al. Haemophilus influenzae forms biofilms on airways epithelia: implications in cystic fibrosis. Am J Respir Crit Care Med 2006; 174: 213–230. 38. King PT, Hutchinson PE, Johnson PD, et al. Adaptive immunity to non typeable Haemophilus influenzae. Am J Respir Crit Care Med 2003; 167: 587–592. 39. Wilson R, Dowlin RB, Jackson AD. The biology of bacterial colonisation and invasion of the respiratory mucosa. Eur Respir J 1996; 9: 1523–1530. 40. Mathee K, Ciofu O, Sternberg C, et al. Mucoid conversion of Pseudomonas aeruginosa by hydrogen peroxide: a mechanism for virulence activation in the cystic fibrosis lung. Microbiology 1999; 145: 1349–1357. 41. Lau GW, Hasset DJ, Ran H. The role of pyocyanin in Pseudomonas aeruginosa infection. Trends Mol Med 2004; 10: 599–606. 42. Caldwell C, Chen Y, Goetzmann HS, et al. Pseudomonas aeruginosa exotoxin pyocyanin causes cystic fibrosis airway pathogenesis. Am J Pathol 2009; 175: 2473–2488. 43. Chmiel JF, Davis PB. State of the art: why do the lungs of patients with cystic fibrosis become infected and why can’t they clear infection? Respir Res 2003; 4: 8. 44. Lu W, Hisatsume A, Koga T, et al. Cutting edge: enhanced pulmonary clearance of Pseudomonas aeruginosa by Muc1 knockout mice. J Immunol 2006; 176: 3890–3894. 45. Wouters EFM. Local and systemic inflammation in chronic obstructive pulmonary disease. Proc Am Thorac Soc 2005; 2: 26–33. 46. Aldallal N, Mc Naughton EE, Manzel LJ, et al. Inflammatory response in airway epithelial cells isolated from patients with cystic fibrosis. Am J Respir Crit Care Med 2002; 166: 1248–1256. 47. Angrill J, Agusti C, De Celis R, et al. Bronchial inflammation and colonisation in patients with clinically stable bronchiectasis. Am J Respir Crit Care Med 2001; 164: 1628–1632. 48. Liu Y, Shaw Sk, Ma S, et al. Regulation of leucocyte transmigration: cell surface interactions and signalling events. J Immunol 2004; 172: 7–13. 49. Eller J, Lap e Silva JR, Poulter LW, et al. Cells and cytokines in chronic bronchial infection. Ann NY Acad Sci 1994; 725: 331–345. 50. Loukides S, Bouros D, Papatjheodorou G, et al. Exhaled H2O2 in steady-state bronchiectasis: relationship with cellular composition in induced sputum, spirometry, and extent and severity of disease. Chest 2002; 121: 81–87. 51. Adams DH, Shaw S. Leucocyte-endothelial interactions and regulation of leucocyte migration. Lancet 1994; 343: 831–836. 52. Hogg JC. Leukocyte traffic in the lung. Ann Rev Physiol 1995; 57: 97–114. 53. Zheng L, Tipoe G, Lam WK, et al. Upregulation of circulating adhesion molecules in bronchiectasis. Eur Respir J 2000; 16: 691–696. 54. Carlos T, Kovach N, Schwarz B, et al. Human monocytes bind to two cytokine induced adhesive ligands on cultured human endothelial cells: endothelial-leukocyte adhesion molecule-1 and vascular cell adhesion molecule-1. Blood 1991; 77: 2266–2271. 55. Dustin ML, Rothlein R, Bhan AF, et al. Induction by IL-1 and interferon-c: tissue distribution, biochemistry and function of a nature adherence molecule (ICAM-1). J Immunol 1986; 137: 245–254. 56. Pang JA, Cheng A, Chan HS, et al. The bacteriology of bronchiectasis in Hong Kong investigated by protected catheter brush and bronchoalveolar lavage. Ann Rev Respir Dis 1988; 139: 14–17. 31 M. GODDARD 57. Sepper R, Kontinnen YT, Ding Y, et al. Human neutrophil collagenase (MMP-8) identified in bronchiectasis BAL fluid, correlates with severity of disease. Chest 1995; 107: 1641–1647. 58. Zheng L, Lam WK, Tipoe GL, et al. Overexpression of matrix metalloproteinases-8 and -9 in bronchiectasis airways in vivo. Eur Respir J 2002; 20: 170–176. 59. Sepper R, Kontinnen YT, Sorsa T, et al. Gelatinolytic and type-IV collagenolytic activity in bronchiectasis. Chest 1994; 106: 1129–1133. 60. Doring G. The role of neutrophil elastase in chronic inflammation. Am J Respir Crit Care Med 1994; 150: S114–S117. 61. Lloberes P, Monserrat E, Monserrat JM, et al. Sputum sol phase proteins and elastase activity in patients with clinically stable bronchiectasis. Thorax 1992; 47: 88–92. 62. Loukides S, Horvath I, Wodehouse T, et al. Elevated levels of expired breath hydrogen peroxide in bronchiectasis. Am J Respir Crit Care Med 1998; 158: 991–994. 63. Simpson JI, Grissell TV, Gibson PG. Innate immune activation in bronchiectasis. Eur Respir J 2004; 24: Suppl. 48, 210S. 64. Devalia JL, Davies RJ. Airway epithelial cells and mediators of inflammation. Respir Med 1993; 87: 405–408. 65. Look DC, Rapp SR, Keller BT, et al. Selective induction of intercellular adhesion molecule-1 by interferon-c in airway epithelial cells. Am J Physiol 1992; 263: L79–L87. 66. Humlicek AL, Pang L, Look DC. Modulation of airway inflammation and clearance by epithelial ICAM-1. Am J Physiol Lung Cell Mol Physiol 2004; 287: L598–L607.