Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
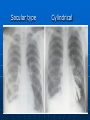
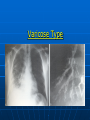
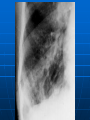
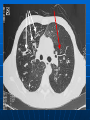
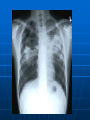
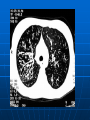
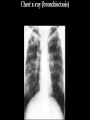
This young man has long history of productive cough and wheezing. He is afebrile and chest auscultation reveals coarse crackles at right lower chest BRONCHIECTASIS Bronciectasis (Greek word) •Bronkos ---- Wind pipe •Ektesis ---- Stretching HOW DO YOU DEFINE BRONCHIECTASIS ? BRONCHIECTASIS Abnormal and permanent dilatation of bronchi and bronchioles greater than 2 mm CLASSIFICATION REID’S CLASSIFICATION (1950) • Based on Pathology & Bronchography Cylindrical Varicose Saccular (Cystic) Sacular type Cylindrical Varicose Type MUCOUS PLUGS DILATED BRONCHIOLE PATHOGENESIS NORMAL HOST RESPONSE TO BRONCHIAL INSULT BRONCHIAL INSULT RETURN TO HEALTH MUCOCILLIARY CLEARENCE INFLAMMATION ABNORMAL HOST RESPONSE TO BRONCHIAL INSULT BRONCHIAL INSULT BRONCHIECTASIS INFLAMMATION BRONCHIAL DAMAGE IMPAIRED MUCOCILLIARY CLEARENCE FURTHER INFLAMMATION BRONCHIAL OBSTRUCTION PATHOGENESIS OBSTRUCTION INFLAMMATION ETIOLOGY OF BRONCHIECTASIS Congenital Acquired Case Study While doing clinical elective in UK, you happen to see a young man, who has been regularly visiting chest clinic since birth with multiple admissions. He c/o productive cough and shortness of breath. His brother also suffers from the same disease. His chest x-ray is What is the diagnosis ? What is mode of inheritance ? What do you see on this chest x-ray. What is pathology CYSTIC FIBROSIS What is the diagnosis ? What is mode of inheritance ? What do you see on this chest x-ray. What is pathology Case Study 30 Years old gentleman comes to you with chronic sinusitis and productive cough. His x-ray of sinuses and chest are What is the diagnosis ? Kartageyner Syndrome Primary ciliary dyskinesia (PCD) or Kartagener Syndrome (KS), is a rare, ciliopathic, autosomal recessive gene tic disorder that causes a defect in the action of the cilia lining the respiratory tract (lower and pper, sinuses, Eustachian tube,middle ear) and fallopian tube. Kartageyner Syndrome It is combination of Ciliary Dyskinesia and situs inversus (complete or incomplete) Infertility What are the congenital causes of Bronchiectasis ? ETIOLOGY: CONGENITAL Cystic Fibrosis Primary Ciliary Dyskinesia Kartagener’s Syndrome Immunodeficiency States Intralobular Lung Sequestration AQUIRED CAUSES POST INFECTIOUS BRONCHIAL OBSTRUCTION MISCELLANEOUS CONDITIONS AQUIRED CAUSES POST INFECTIOUS Bacterial Mycobacterium tuberculosis Pseudomonas aureginosa Hemophillus influenzae Staphylococcus aureus AQUIRED CAUSES: POSTINFECTIOUS Viral Adenovirus Influenza HIV Fungal Aspergillus fumigatus (ABPA) Allergic Bronchopulmonary Aspergillosis (ABPA) Mainly in Asthmatics Sensitization to aspergillous Raised IgE level Tubular Bronchiectasis ETIOLOGY : BRONCHIAL OBSTRUCTION Tumour Foreign Bodies Mucous Plugs ETIOLOGY: OTHER CAUSES Rheumatoid Arthritis Inflammatory Bowel Disease Systemic Lupus Erythematosus Post transplant CLINICAL PRESENTATION SYMPTOMS Persistent cough Purulent sputum (green and foul smelling) Hemoptysis Dyspnea Wheeze Fever Severe Pneumonia Asymptomatic Non Productive Cough WET TYPE DRY TYPE CLINICAL PRESENTATI0N SIGNS • On GPE Digital Clubbing Cyanosis Plethora Muscle wasting • On Auscultation Crackles Wheeze Ronchi COMPLICATIONS Recurrent pneumonia Empyema Haemoptysis Pneumothorax Lung abscess Brain abscess Amyloidosis Cor pulmonale DIAGNOSIS CLINICAL PRESENTATION SPUTUM ANALYSIS RADIOLOGY DIRECT VISUALISATION ESTABLISHMENT OF CAUSE CLINICAL PRESENTATION HISTORY CLINICAL EXAMINATION RULE OUT Pneumonia Emphysema Lung abscess SPUTUM ANALYSIS Amount of sputum 24 hr Sputum Production Mild Moderate Severe < 10 ml/day <150 ml/day >150 ml/day Visual Impression Microbiology Streptococcus pneumoneae Hemophillus influenzae Aspergillus Psedomonas E. coli LAB TESTS Blood complete picture Quantitative immunoglobulin Alpha-1 anti-trypsin level RADIOLOGY Chest X-ray PA view Cylindrical Varicose Saccular Bronchography CT Scan DIRECT VISUALISATION Bronchoscoy Flexible Rigid ESTABLISHMENT OF CAUSE Serum Protein electrophoresis Serum Immunoglobulins Pilocarpine Iontophoresis (Sweat Test) Aspergillus Precipitin Test Electron Microscopy MANAGEMENT 4 GOALS Elimination of Problem Clear Tracheo-bronchial Secretions Control Infections Reverse Airflow Obstruction MANAGEMENT POSTURAL DRAINAGE BRONCHODIALATORS CORTICOSTEROIDS TREAT INFECTIONS Antibiotics (according to C&S) Amoxicillin 250mg -------Co-amoxiclav 325mg -------Levofloxacin 500mg -------Ceftazidime Preventive and suppressive antibiotics TDS TDS BD Other treatment Inhaled Broncho dilators Inhaled aerosolized aminoglycosides Surgery Reserved for patients with localised bronchiectasis and adequate lung functions Sometime in massive haemoptysis PREVENTION VACCINATION Influenza vaccine Pneumococcal vaccine AVOID EXACERBATING FACTORS Regular chest physiotherapy Stay together