Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
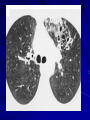
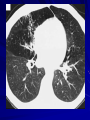
Bronchiectasis Hu Suping Pulmonary Department 1st clinical college, Wuhan University Definition an acquired disorder of the major bronchi and bronchioles characterized by permanent abnormal dilation and destruction of bronchial walls the most common symptoms are chronic cough with large amounts of purulent sputum and/or recurrent hemoptysis it involves chronic respiratory tract infection and an up-regulation of the host inflammatory response Enhanced cellular and mediator responses bronchial mucosal biopsies reveal infiltration by neutrophils and T lymphocytes; expectorated sputum has increased concentrations of elastase and the chemoattractants IL-8, TNFa, and prostanoids Pathological changes Cylindrical or tubular bronchiectasis: dilated airways alone, sometimes seen as a residual effect of pneumonia Varicose bronchiectasis: focal constrictive areas along the dilated airways that result from defects in the bronchial wall Saccular or cystic bronchiectasis: progressive dilatation of the airways, which end in large cysts, saccules, or grape-like clusters (the most severe form ) The lumen of the bronchus is dilated and there is prominent chronic inflammation in the bronchial wall Bronchiectasis can present in either of two forms — a local or focal obstructive process of a lobe or segment of a lung or a diffuse process involving much of both lungs and often accompanied by other sinopulmonary diseases, such as sinusitis and asthma Pathophysiology and Etiology Three types of focal airway obstruction (1) luminal blockage by a foreign body, broncholith, or slowly growing benign tumor (2) extrinsic narrowing due to enlarged lymph nodes (middle lobe syndrome) (3) twisting or displacement of the airways after a lobar resection or chronic infection Pathophysiology and Etiology Infections Childhood respiratory tract infections (pertussis or whooping cough) Chronic infections( chronic lung abscess, TB) Primary Ciliary Dyskinesia an autosomal recessive syndrome, estimated frequency at birth is 1 in 15,000 to 1 in 40,000 half have Kartagener’s syndrome (bronchiectasis, sinusitis, and situs inversus viscerum) Pathophysiology and Etiology Immunodeficiency humoral immunodeficiency syndromes (deficiencies of IgG, IgM, and IgA) at risk for recurrent suppurative sinopulmonary infections and bronchiectasis immune globulin replacement reduces the frequency of infectious episodes and prevents further destruction of the airways Clinical findings Symptoms: daily cough productive of mucopurulent phlegm intermittent hemoptysis recurrent lung infections shortness of breath Physical findings: crackles, cyanosis Chest radiography High-resolution computed tomographic scanning (HRCT) the defining modality for diagnosis of bronchiectasis Specific abnormalities found on HRCT include (1) dilatation of an airway lumen > 1.5 times as wide as a nearby vessel (2) lack of tapering of an airway toward the periphery (3) varicose constrictions along airways (4) ballooned cysts at the end of a bronchus Normal lung Bronchiectasis Normal Lung and the Lung of a Patient with Bronchiectasis. Bronchiectasis is primarily in the lower lobe, which is the most common distribution. The saccular dilatations and grapelike clusters with pools of mucus are signs of severe bronchiectasis. Bronchoscopy an important diagnostic tool to examine for obstruction ( foreign body, tumor, structural deformity, or extrinsic compression from lymph nodes) and to help localize the bleeding,to identify pathogen Pulmonary function tests obstructive impairment ( low FEV1 and/or low FEV1/FVC) airway hyperresponsiveness ( 40% with a positive reversibility test result, and 30% to 69% with a positive bronchial provocative test result) Diagnostic evaluation (1) to confirm the diagnosis of bronchiectasis (2) to identify potentially treatable underlying causes (3) to provide functional assessment Imaging of the chest is always necessary to confirm the diagnosis Differential diagnosis Chronic bronchitis Lung abscess Pulmonary tuberculosis Congenital bronchocele Diffuse panbronchiolitis Therapy Control infections:administration of antibiotics Treatment of underlying conditions Promotion of bronchial hygiene Control of bronchial hemorrhage Surgical therapy Acute Exacerbations An exacerbation: including four of the nine symptoms change in sputum production; increased dyspnea; increased cough; fever (>38.0°C); increased wheezing; malaise, fatigue, lethargy, or decreased exercise tolerance; changes in chest sounds; reduced pulmonary function; radiographic changes Early antibiotic therapy: fluoroquinolone as levofloxacin or ciprofloxacin for at least 7 to 10 days Sputum culture and sensitivity testing: who fail to respond to the initial antibiotic or who have repeated symptomatic attacks in a short interval Bronchopulmonary Hygiene Postural drainage, chest physiotherapy, thinning and loosening of secretions, the administration of a bronchodilator and of inhaled corticosteroids –part of maintenance therapy and treatment for acute exacerbations Hemoptysis life-threatening hemoptysis: > 600 ml/ day bronchoscopy or CT of the chest is warranted to help determine which lobe or side is bleeding interventional radiology: selective bronchial arteries embolization surgery may be required to resect an area suspected of bleeding Surgery Removal of an obstructing tumor or residue of a foreign body Elimination of the segments or lobes the most damaged and suspected of contributing to acute exacerbations, overwhelming viscous secretions, mucous impaction, and plugs Elimination of areas that are subject to uncontrolled hemorrhage Removal of damaged lung suspected of harboring problematic organisms such as multidrug-resistant M. tuberculosis or M. avium Double-lung transplantation is now considered for patients with cystic fibrosis and respiratory failure (one year survival rate 75% and 48% at five years)