Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
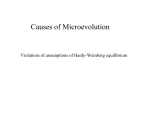
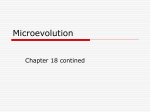
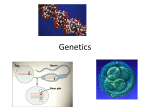
Evolution by Phenotype a biomedical perspective Kenneth M. Weiss *† and Anne V. Buchanan * ABSTRACT Genes are widely assumed to play a major role in the epidemiology of complex chronic diseases, yet attempts to characterize the genetic architecture of such traits have been frustrating. Understanding that evolution works by screening phenotypes rather than genotypes can help explain the source of this frustration. Complex traits are usually the result of long-term, often subtle, gene-environment interactions, such that individual life histories may be as important as population histories in predicting and explaining these traits. Recognizing that the problem is not due to technological limitations can help temper expectations and guide the design of future work in biomedical genetics, by allowing us to focus on better approaches where they exist and on those problems most likely to yield a genetic solution.We may even be forced to re-conceive complex biological causation. “How extremely stupid not to have thought of that!” Thus is Thomas Huxley famously said to have bemoaned his failure to see something so obvious as evolution of species by descent from a common ancestor. It is easy to be so programmed to think in a particular way that, like Huxley, we miss things that, once pointed out, are obvious. Departments of Anthropology* and Biology,† Penn State University, University Park, PA 16802. Email: [email protected]. The authors wish to thank Joe Terwilliger, Charles Sing, and three reviewers for helpful suggestions, whether or not they agree with the authors’ views. Financial support from NIH/NHLBI award HL 58239 is gratefully acknowledged. Perspectives in Biology and Medicine, volume 46, number 2 (spring 2003):159–82 © 2003 by The Johns Hopkins University Press 159 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n The assumption of the primacy of genes has dominated biology for 75 years. Huge investment is being made in working out the genetic basis of common, complex chronic diseases. To date, this attempt has been frustrated, due in large part to excessive genetic determinism resulting from an insufficient appreciation of fundamental aspects of evolutionary biology.The ideas are simple and in principle well known, but they are not yet well integrated into daily practice. Evolution by Phenotype Darwin and Wallace provided a plausible mechanism by which the external environment could generate the dynamic history and pattern of divergence among organisms.This was a theory of evolution by phenotype, the notion that organisms evolved by having spontaneously generated variation screened by natural selection.The theory itself left open the question of what exactly is inherited, and it remained for Mendel to provide leads to the answer. Like Darwin, Mendel studied traits, not genes, but he carefully chose qualitatively varying traits that (we now know) were closely tied to genes. By the early 20th century, it was shown that the contributions of many genes with individually small effect could produce complex or quantitatively distributed phenotypes (like stature or weight), and the genetic theory of evolution, known as the Modern Synthesis, was formulated (e.g., Mayr 1982, 1991). The subsequent discovery of DNA as a ubiquitous protein coding system, expressed in the Central Dogma of the one-way transfer of coding information from nucleic acid to protein, reinforced this view and provided an understanding of the nature of the informational molecule that was transmitted across generations.These advances provided the basis for a powerful systematic genetic research program. Biology today is thoroughly rooted in the Modern Synthesis, a theory in which causation is regarded as ultimately gene-based. The implications of this tenet have been considered in detail over the past century and more, in regard to the varying units of selection, including organisms, populations, and species (e.g., Gould and Lloyd 1999; Lewontin 2000; Mayr 1982, 1997). But while genes are quasi-permanent units of biological information storage, the screening of phenotypes by natural selection is only indirectly reflected in genotypes. Important aspects of evolution by phenotype can be illustrated schematically in Figure 1. Time moves downward from a common ancestor at the top. Each point represents a position occupied by a single individual in phenotype “spacetime.”We won’t enter the endless debate about what appropriately constitutes the “phenotype”: ultimately it is the reproducing organism, but in some cases it may for all practical purposes be a particular trait, or even a community of organisms. An individual phenotype is the result of the interagency of all the internal and external factors encountered by the inherited genotype.The scatter at any given time represents the existing range of diversity, whose viable limits are indicated by ellipses.The bottom scatters show the range of variation in three modern species. 160 Perspectives in Biology and Medicine Evolution by Phenotype Figure 1 Evolution in time and phenotype space. Points are individuals in X-Y phenotype space, as this changes over time (vertical axis); ellipses represent acceptable phenotype space for a species at any given time. A, B, C are present-day species. Highly schematic. The denser scatter near the centroids at any time represents the usual pattern, in which at most a few similar states are quite common, and there are numerous variant states (the farther from the centroid, the rarer). Frequency and effect size measured relative to the centroid are frequently confounded, an important point in human genetics, where disease states are often characterized relative to a mean “normal” state, archaically still typically referred to as “the wild type.” The centroids change over time due to the various evolutionary factors at work.The lines suggest the way we use the centroids as rather platonic abstractions in drawing phylogenies, but all that really exist are the more Aristotelian sets of individuals (dots). Perhaps because of this Platonism, related metaphors like “survival of the fittest” and our gene-centered theory lead to a widespread tendency to view natural selection as prescriptive at the gene level. But there are a number of reasons why we should consider selection instead to be more tolerant of variation. The Lamarckian Temptation The fit of organisms to their way of life can make it appear as if they have been heading consistently or even purposefully towards their present state through evolutionary time. This was Lamarck’s famous notion—the impression that there has been a steady history of highly prescriptive genotypic specification. But this can be misleading. The most important reason is the “anthropic” illusion: whatever exists today is the product of a 3.5-billion-year unbroken lineage of ancestors, each of which, by virtue of having reproduced successfully, was “adapted.” As has been noted countless times, were we to look forward to some spring 2003 • volume 46, number 2 161 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n time millions of years from now, any particular future biological outcome would be laughably improbable. But we must remember that of all the essentially unlimited things that might have evolved, something had to do so in order to be here.Yet a strongly adaptationist viewpoint leads to the assumption that essentially every trait must be the product of adaptive natural selection, with a specific genetic explanation. The assumption that everything is being selected all the time at the gene level can lead us to seek functional constraints or to infer strong genetic effects that may not exist. Imperfectly Precise Biological Processes An individual experiences a variety of factors during life that affect his or her phenotype. Individuals with the same inherited genotype, such as identical twins or inbred laboratory animals, are not identical, in part because they do not have identical life histories. Some factors that generate phenotypic variation during life are genetic, caused by mutations that do not get repaired: for example, DNA and RNA polymerases mis-incorporate nucleotides to introduce point mutations; DNA is nicked by UV light and not repaired; and gene duplication or deletion may cause a variety of dose-related stresses. We usually think about genetic variation due to germline mutations, but somatic mutations also occur, turning a multicellular organism into a genotypic mosaic. Some somatic mutations may lead to cancer, but others are not associated with disease. Numerous non-genetic factors may also lead to phenotypic variation. A substantial fraction of newly synthesized polypeptides fold incompletely and thus cannot generate functional protein; cell division can be anomalous; mitosis and other stochastic factors can lead individual cells to have aberrant (low or high) numbers of required structures, which can induce gene expression changes in the cell and its lineal descendants in the organism; and so on. Liability for these kinds of random events to happen may or may not be inherited, but even if there is an inherited effect, these factors add a potentially substantial element of realized variation in organisms. In all of this there is a stochastic element. Chance affects whether an anomalous molecule is detected or a gene turned on in a particular cell; what a dividing cell differentiates into; whether a fertilized crocodile egg develops into a male or female (a process that is temperature-dependent); whether a given plant reproduces (if it depends on successful fertilization by external factors like wind or bees); or whether it germinates at all. Structures like sensory bristles on flies develop when random developmental factors lead one of a number of equally prepared cells to initiate a structure, and to suppress development in a surrounding inhibition zone of cells. This patterning depends on the relative concentrations of transcription factors, as well as of inhibitory gene products, parameters that have stochastic attributes.The role of chance is seen in the variability among identical twins or inbred laboratory animals in traits ranging from fingerprints to disease history to lifespan (Finch and Kirkwood 2000). 162 Perspectives in Biology and Medicine Evolution by Phenotype From zygote to death, organisms have evolved considerable plasticity to respond to what both internal and environmental factors, including chance, may bring. Among these capabilities are a host of repair mechanisms, many of which are so primary that they were probably present in the early evolution of cells (Yasui and McCready 1998). Perhaps 2 percent of a cell’s energy is used in error control (Scriver 2002), and an unknown amount is involved in the production of errors in the first place. Enzymes that repair replication errors, somatic mutations, mitotic errors, or errors caused by environmental degradation (e.g., UV exposure) are ubiquitous in cells. Endonucleases, exonucleases, proteases, tumor suppressors, perhaps even the immune system itself (because its job is to recognize and destroy “foreign” proteins), all keep the error-prone cellular functions in line. Nonetheless, not all errors are prevented or repaired, and tolerance has its limits. Internally produced errors left unchecked can eventually exceed what we would consider normal, or what corrective mechanisms can correct, and appear in the form of disease. Cancers can arise when cell-cycle regulation experiences unrepaired damage, and neurodegenerative diseases such as Alzheimer’s, Parkinson’s, Huntington’s, or Creutzfeld-Jakob, may develop when cells do not rid themselves of accumulations of misfolded proteins (Wickner, Maurizi, and Gottesman 1999). Homeostatic mechanisms work in the short run; an organism has no way to anticipate the eventual damage incurred by environmental exposures that are within homeostatic tolerance at any given moment, but which, over time, become a major risk factor for complex chronic disease.The ultimate risks incurred by decades of over-eating are one such example. Despite these many sources of variation, we are surrounded by organized and recognizable order. Organisms are protected by a kind of “law of large numbers” or “central limit” effect. Even with developmental and somatic mosaicism in cellular phenotypes and genotypes within an individual, most individuals end up close to their population mean for most traits. Billions of years of evolution have kept the underlying genotypic variation, error-protections, and the like within acceptable range (and many of those who fall out of that range never are born to be observed). In this sense, we can say that organisms have considerable self-organizing properties. The fact that phenotypes are often modally distributed, with most organisms near the mode, justifies idealizations such as equating the most common or modal state with the “wild type,” relative to variants or mutants. But this can be misleading, because for some purposes, like understanding variation among individuals within a species (such as with respect to susceptibility to disease), the amount of relevant variability may be high. We acknowledge that in the foregoing we have been quite platonic ourselves. Concepts of error and chance are judged relative to an assumed truth, mode, or known process.Whether anything is truly stochastic, and whether our assessment of “error” is correct, are important questions. In the end, what counts in life is not an “ideal” state but sufficiency. Deterministic processes can for all practical spring 2003 • volume 46, number 2 163 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n purposes appear “random” (Wolfram 2002), but variation of the sort discussed here, whatever its actual cause, will not be genetic in the sense of inheritance. Several Forms of Evolutionary Drift Variation in DNA sequence that has no function, or whose functional effects do not push its bearers out of the part of the phenotype space that is not directly affected by natural selection, is known as selectively “neutral” variation.This variation changes over time by the random aspects of life and death that are known generally as genetic drift. Biologists have become comfortable with the notion of selective neutrality of DNA sequence variation, and even with the fact that chance affects the frequencies of alleles under selection. But despite the fact that similarly incidental variation can be seen in almost every biological trait almost every day, we have been curiously resistant to applying a similar notion to phenotypes. Such a possibility is fully compatible with formal evolutionary theory but is not prominent, and instead there is a widespread tendency to offer adaptive explanations for almost anything. Darwin acknowledged that some phenotypic variants may be selectively neutral, but clearly his main legacy was the notion that “each slight variation, if useful, is preserved, by . . . Natural Selection” (Darwin 1859). The usual logic of adaptive explanations is important to state: My Favorite Trait evolved stepwise, from some rudimentary origin, by adaptive selection favoring each step for some reason that may, but need not, have been related to the present function we are trying to explain.Thus, for example, vision evolved stepwise from simple cell-adhesion receptors, to photoreceptors, and ultimately to complex eyes. But let us just look around us. Most variation we see every day has little if anything to do with Darwinian fitness. As with DNA sequences, phenotypic drift can occur, as phenotypic variation changes by chance over generations. We can modify the classical Darwinian argument with the most minor of twists, by removing the adaptive selection from the scenario: My Favorite Trait evolved stepwise, from some rudimentary origin, by drifting in a direction that at each step may, but need not, be related to the present function we are trying to explain. Each step need merely have had what we might call “random suitability” relative to its circumstances. Step-by-step, facultative use of those stages can become behavioral habit—but need not have involved Darwinian turmoil. Again, it is by looking backward over eons of time, and implicitly equating function with origin and assuming it arose via selection, that we experience the Lamarckian temptation, assuming (in ironic agreement with religious fundamentalists) that complexity is simply too improbable to have arisen by chance and must have been molded teleonomically (“for” some function; e.g., Reeve and Sherman 1993; Thornhill 1990). Nothing in the theory of evolutionary biology—including its focus on genes—suggests that phenotypic drift cannot, or did not regularly, occur. Indeed, our hallowed principle of parsimony should restrain us from invoking causal explanations when none are needed. 164 Perspectives in Biology and Medicine Evolution by Phenotype Phenogenetic relationships—that is, between genotype and phenotype—are often many-to-many relationships. A genotype can be associated with a range of phenotypes (e.g., quantitative measures such as blood pressure, or qualitative ones like affected/unaffected); this is due to the imprecision of biological processes discussed above, not to mention environmental effects (Schlichting and Pigliucci 1998). For similar reasons, the same phenotype can be found in individuals with many different genotypes, a phenomenon we can refer to as “phenogenetic equivalence.” When there is phenogenetic equivalence, genetic variation associated with the same phenotype will change over time by drift, even if the phenotype is being maintained by strong natural selection, because genotypes with equivalent fitness are neutral relative to each other (Clark 1998; Hartl and Campbell 1982). This dynamic heterogeneity can be referred to as “phenogenetic drift” (Weiss and Fullerton 2000). Phenogenetic drift refers to the uncoupling of specific relationships between functional genotypes and the same phenotype. Epistasis (gene-gene interaction) and pleiotropy (multiple functions of a gene) may affect the pattern, rate, or nature of phenotypic drift. For example, selection related to one function of a pleiotropic gene can constrain traits associated with its other functions or lead to a balance between the different selective effects. A biomedically important result of phenogenetic equivalence or drift is that it may not be possible to infer the genotype underlying an observed phenotype. Here as before, it is difficult to resist the temptation to think platonically. Like notions of error and chance, ideas of selective neutrality or equivalence may themselves be ephemeral and context-specific. The Amount and Pattern of Variation Most new mutations are unique at the DNA sequence level, either themselves, or because of their haplotype background (the specific set of sequence variants around them on the chromosome on which they arose). A newly arising variant will perforce initially be geographically localized; it may increase in frequency, by chance or by selection, and may diffuse from its native region over subsequent generations. Rare variants thus tend to be geographically localized, while common variants tend to be older. Because humans reproduce slowly, this applies in particular to globally distributed variants, which as a rule were present in our common ancestors in Africa. Natural selection works on phenotypes but can only affect the frequency of local genetic variation associated with those phenotypes. This means that even the same selective force is likely to favor different and/or multiple genetic variants in different geographic regions, or within the same region. As a result, phenotypic convergence (or conservation) is often associated with genotypic divergence. The amount of variation in a given gene depends on demographic history: population size, migration patterns, selective effects, birth and death of individuals, and mutation rates (e.g., Harpending et al. 1998; Hartl and Clark 1997; spring 2003 • volume 46, number 2 165 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Jorde, Bamshad, and Rogers 1998; Jorde,Watkins, and Bamshad 2001; Jorde et al. 2000; von Haeseler, Sajantila, and Paabo 1996). Each of these has a stochastic element. Population bottlenecks and selection reduce variation and simplify the sequence relationships among haplotypes. For single nucleotide positions as well as haplotypes, the frequency distribution in a given population is usually rather “modal,” comprising a small number of relatively common variants and a long tail of rarer ones.These are the general properties expected of variation in selectively neutral DNA sequence, and because of phenogenetic drift similar characteristics generally pertain to sets of alleles that are associated with specific phenotypes (like disease), even if the latter are affected by selection. It is often said that humans are not as variable as other globally distributed species.This appears to be due to our history as a species recently formed from a small initial population, rather than to a history of strong natural selection. On average, if the sequences of two copies of a human chromosome region are compared, they will differ about once every 1,300 nucleotides.This may seem small, but in a genome of 3.3 billion nucleotides, it comprises roughly 2 to 3 million differences. If even a modest number of copies of the region are compared, rather than just two, one may see a variant every hundred positions; most sites may show variation in some human somewhere.The lack of variation in the human genome relative to that in other species does not imply that we have insufficient variation for there to be complex heterogeneity in genetic effects related to disease. Biomedical Implications We have considered various aspects of biological variation from the general perspective that evolution screens organisms by phenotype rather than by genotype. Nothing in evolutionary theory guarantees extensive variation (except for special cases such as immune diversity), but mutational pressure and the tolerant nature of selection suggest that variation can be expected, and that is consistent with experience. Phenogenetic relationships are consequently likely to be less precise and deterministic than seems generally appreciated.These simple principles are not new but are often overlooked, and they can help explain many of the complexities and frustrations encountered by efforts to map and understand genes associated with disease. Biomedical ascertainment screens populations in interesting ways that resemble natural selection itself. Like natural selection, we screen our population by phenotypes, via their appearance in clinics and registries. This effectively identifies the tail of the phenotype distribution (abnormal, early onset, hyper- or hypometabolic values or risk), and it is worth reflecting on just how distorted a view from the tail of life can be.The biomedical ascertainment systems of the wealthiest countries of North America, Europe, and Asia screen at least a half-billion people in whom a serious disease might be detected. When N = 500,000,000, alleles that are very rare indeed get noticed. 166 Perspectives in Biology and Medicine Evolution by Phenotype table 1 N UMBERS OF A LLELES AT S ELECTED D ISEASE -R ELATED G ENES Gene (Trait) TP53 (colon, other cancers) CFTR (cystic fibrosis) LDL receptor (heart disease) PAH (PKU = phenylketonuria) BRCA1 (br, ovarian cancer) DMD (muscular dystrophy) GBA (Gaucher’s disease) BRCA2 (br, ovarian cancer) Pax6 (eye problems) TSD (Tay-Sachs disease) Pax3 (hearing, pigmentation) Mutations ~1,300 1,001 771 336 319 186 157 154 115 91 44 SOURCE: HGMD (2002). Genetic effects in such individuals may not have the same properties as those found in the bulk of the population.We can see the difference by comparing the genetics of relatively “simple” traits, which tend to be rare, with that of “complex” traits, which may be common and where the ascertainment system is somewhat different. The Genetic Basis of Highly Deleterious Pediatric Diseases An allele whose effects are strong and hence rare will generally be the only such allele segregating in a given family.“Strong effect” is another way of saying there is a high probability of an allelle’s being detected if present, or a large effect on the phenotype relative to the mean, so that the trait will appear to be “Mendelian” (closely tied to the segregation of the underlying allele in families), and causation will appear relatively straightforward. Such traits are easy to map genetically, and genes responsible for hundreds of them have been mapped (OMIM 2002).Yet even in these instances there are complex phenogenetic relationships and considerable genetic heterogeneity (HGMD 2002). Phenylketonuria (PKU) is a familiar and well-studied example. PKU is a disease of amino acid metabolism.That PKU is genetic in nature has been known for decades, based on its classically Mendelian appearance in families. Most cases result from reduced activity of a single gene product, the enzyme phenylalanine hydroxylase (PAH).This leads to levels of phenylalanine that can be toxic, especially to the brain, and can result in severe mental retardation. The mutational spectrum and phenogenetic relationships of PAH are typical of most simple Mendelian diseases (Table 1; see OMIM 2002). Hundreds of alspring 2003 • volume 46, number 2 167 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Figure 2 Relative frequency of disease-associated PAH alleles. Distribution of 444 different observed alleles. S OURCE : PAH DB (2002). leles at the PAH locus have been seen in patients, including a small number of relatively common alleles and many rare ones (Figure 2). The presence and frequency of alleles vary among populations, with many alleles being specific to a given regional origin (e.g., part of Europe).These characteristics reflect the geographically localized nature of most new mutations, as well as population history and phenogenetic drift among alleles associated with similar phenotypes that are roughly equivalent in the face of selection. PKU is generally considered to be a “recessive” disease, but this is a legacy term from Mendel’s two-state world that can have misleading connotations. Classic PKU segregates in Mendelian ways in families, but we now know that at the genetic level most persons affected with PKU are not homozygotes, but heterozygotes with two different alleles whose combination leads to clinically elevated phenylalanine levels. Now that we can go beyond a classical two-allele (abnormal, wild-type) classification, we have discovered a quasi-continuous genotype-phenotype distribution (Table 2), with considerable phenogenetic equivalence, among the huge number of diploid genotypes that can result from hundreds of alleles (Guldberg et al. 1996; Kayaalp et al. 1997; Scriver and Waters 1999). Recognition of variable severity has led to the specification of a second clinical category, non-PKU hyperphenylalananemia (HPA), which arises in genotypes whose alleles have less severe average effects. However, even the revised clinical categories represent rather arbitrary subdivisions of a more continuous phenotype distribution, and are far from perfectly predictable, as the table shows. Indeed, most effects are probably difficult even to estimate with replicable accuracy. 168 Perspectives in Biology and Medicine Evolution by Phenotype table 2 PAH G ENOTYPE -P HENOTYPE R ELATIONSHIPS : O BSERVED E XPECTED M ETABOLIC P HENOTYPES IN 184 I NDIVIDUALS PAH D EFICIENCY VERSUS WITH OBSERVED PHENOTYPE PKU Genotype Score 1 Expected Phenotype 2 2 Classic PKU 42* 11 3 Moderate PKU 10 13* 4 Moderate/mild PKU 1 5 and 6 Mild PKU 1 Classic Moderate Mild Total 4 — 57 73.7 6 — 29 44.8 6* 6* — 13 92.3 3 23* 2 29 79.3 10* 20 100.0 35* 36 97.2 47 184 8 Mild PKU/MHP — — 10* 9–16 MHP — — 1 54 33 50 TOTAL Obs=Exp (%) MHP 1 Sum of estimated effects of individual alleles, where 1 = classic PKU, 2 = moderate PKU, 4 = mild PKU, 8 = mild HPA (MHP) symptoms. 2 Determined, for each patient, on the basis of the sum of the observed alleles of the two PAH mutations. *Groups in which the observed matched the expected phenotype. SOURCE: GULDBERG, ET AL. (1996). Because clinics (like natural selection) concentrate on persons with health problems, the population distribution of severity is not well-known, but Figure 3 shows in schematic terms what such distributions may look like. Some genotypes have strong (PKU) and others, milder (HPA) effects. Genotypes with even lesser and probably less predictive effects must exist in the unaffected population, but we have no way to know a priori how frequent and complex these might be, nor how many additional alleles or other risk factors may exist. Clinical samples aggregate all the sources of risk present in the population and hence may make poor material from which to estimate these things. Different sets of PKU-related alleles have arisen in Europe and Asia (Scriver et al. 1996). PKU is very rare in sub-Saharan Africans (and their descendant populations, such as African-Americans).That there are hundreds of such mutations in Eurasians suggests that there may have been some selection on phenotypes related to PAH that elevated the frequency of the sets of relevant mutations occurring independently in the history of Europe and Asia, leading to a kind of phenotypic convergence with genotypic divergence.What the selective factor(s) may have been is unknown. Strong Selection over Time: The Hemoglobinopathies Under some circumstances strong natural selection can maintain mutations with very harmful effect at high frequency in a population. The classic case is genetic variation related to malaria. Mutations in the alpha- and beta-globin gene spring 2003 • volume 46, number 2 169 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Figure 3 Frequency and effect size for PAH. Schematic of the distribution of the frequency and severity of phenotypes associated with blood levels of phenylalanine. Most cases of true PKU are in the tail of the allelic effects distribution. Many individuals have modestly elevated phenylalanine levels. Many other individuals in the population have genotypes that may have small but subclinical and hence rarely seen effects. clusters can cause anemias of various types by interfering with oxygen—carbon dioxide transport in red blood cells (Scriver et al. 2001). In the canonical instance of balancing selection, homozygosity for the sickle-cell mutation in the beta-globin gene leads to severe anemia, which is strongly selected against, but homozygotes for the “normal” allele are severely affected by malaria which is also strongly selected against; however, heterozygotes are relatively resistant to both malaria and anemia.The result is an intermediate frequency of the two alleles. This classical view suggests that selection works directly via genotype, but the truth is more complex in view of evolution by phenotype. There is extensive phenogenetic equivalence among individuals with the phenotype “malaria resistance,” involving coding as well as regulatory variation in many different genes, including glucose 6-phosphate dehydrogenase (G6PD) and the Duffy blood type gene, as well as the genes in the alpha- and beta-globin clusters (Scriver et al. 2001;Vogel and Motulsky 1997; Weatherall 2001; Weiss 1999). As expected, this observed variation is geographically coherent, reflecting the local histories of each mutation. There are many mutations in the beta-globin genes. Sickle-cell hemoglobin (HbS) is found from Africa across to western India, but Africa is also home to HbD and HbC, and a variety of mutations and deletions in the other genes in 170 Perspectives in Biology and Medicine Evolution by Phenotype the cluster.The predominant mutations in Asian populations—HbE in the betaglobin gene and a variety of mutations in the alpha-globin cluster—are essentially absent in Africa. At other loci, the relevant Duffy allele has reached very high frequency in Africa, as G6PD mutations have in the Mediterranean. Thus, even strong selection favoring a specific phenotype closely tied to specific genes does not usually purify allelic variation, even within a specific population. It might be objected that we are here lumping together different forms of malaria to which there are different adaptations.That is so—and it is well known that, in general, the more precisely or narrowly defined a phenotype is, the closer it is to specific physiological pathways more likely to involve a limited number of genes. That was Mendel’s trick, too. This knowledge is often honored in the breach, in regard to the search for genes related to vaguely defined traits like diabetes, obesity, epilepsy, schizophrenia, or heart disease. Still, even for a given form of malaria, it is common to find multiple genetic responses. And genetic resistance to malaria is at least as complex in mice (Fortin, Stevenson, and Gros 2002). The Genetic Basis of “Complex” Diseases We should always view with caution reasoning about a phenomenon that is based on its extreme. But success in mapping rare pediatric diseases has given human genetics hope that the same methods will work for common complex chronic diseases like cancers, hypertension, and heart disease. From a genetic point of view, complex traits involve many loci. In the simplest model for this, innumerable loci termed polygenes contribute in a dose-like way to underlying risk of qualitative outcomes (heart attack) or quantitative phenotypes (blood pressure) (Hartl and Clark 1997). In this model, many genotypes will be associated with similar phenotypes; adding environmental effects completes the many-to-many picture of phenotypic equivalence noted earlier. Observation and experiment have long supported this general model (e.g., Wright 1968–1978). However, alleles at some of the loci may have relatively stronger individual effect (i.e., high penetrance) (Mackay 2001a, 2001b).These genes have become known as quantitative trait loci (QTL), and in the disease context may be associated with early onset, high severity, or idiosyncratic pathology. Because of the confounding of frequency and effect size, such alleles are typically rare, act in families as “Mendelian” alleles, and account for successful applications of gene-mapping approaches to complex diseases.The alleles also tend to be geographically localized; when the loci are examined in detail, a large number of additional alleles are usually found, with effects typically smaller and often difficult to estimate precisely. Examples are the BRCA genes associated with breast cancer, and TP53, which is associated with various cancers. Despite a number of successes of this sort, many if not most complex diseases have not been cracked even in this limited way. A common experience is that different mapping studies identify a number of apparently relevant loci, but the findings are difficult to replicate and the initial effect estimates are biased upspring 2003 • volume 46, number 2 171 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Figure 4 Many layers between genotype and phenotype. Illustrates with a chromosomal cluster of lipidrelated apolipoprotein genes (AI, CIII, AIV) how the effect of the inherited genotype on risk of coronary artery disease (CAD), or heart attack, a stochastic late-onset final event, is filtered through various levels, from primary gene-product level, risk variable (e.g., triglycerides, or HDL cholesterol levels), to risk (top panel, risk inversely related to HDL cholesterol and directly to high triglyceride levels), to outcome. S OURCE : M ODIFIED FROM A FIGURE PROVIDED COURTESY OF C. F. S ING . wards (Goring,Terwilliger, and Blangero 2001; Ioannidis, Schmid, and Lau 2000; Ioannidis et al. 2001). In the end, loci with alleles of replicably strong effect usually account for only a small fraction of cases, leaving a larger residuum of unexplained familial aggregation.Tens of genes have been associated in this way with diabetes, cardiovascular disease, cancer, retinitis pigmentosa, deafness, and many other diseases. Recent tabulations report about 150 genes associated with obesity in humans and in laboratory animals (Brockmann and Bevova 2002; Perusse et al. 2001; Rankinen et al. 2002).Genetic variation associated with disease compatible with reproduction (e.g., because of late onset), and hence not severely constrained by natural selection, can be generally expected to be comparable to variation in neutrally evolving regions or in genes associated with serious pediatric disease that are under strong natural selection. A major objective of complex disease genetics is to use genotypes to predict risk so that targeted preventive measures can be taken. But many factors intervene between an inherited DNA sequence and the final stochastic event of a late-onset disease. These are shown schematically in Figure 4, relative to a cluster of apolipoprotein genes and heart attacks.The genes must be transcribed and 172 Perspectives in Biology and Medicine Evolution by Phenotype translated, and because of the imprecision of biological processes described earlier, there will be variation in the cellular concentration of their protein products. These gene products are related to an intermediate phenotype, the levels of lipoproteins that package cholesterol, triglycerides, and apolipoproteins for circulation in the blood. Lipoprotein levels constitute a more proximate concentration-related risk factor for cardiovascular disease (inverse with HDL cholesterol, direct with triglycerides), and heart attacks themselves have an additional stochastic component. The levels of these risk factors are affected by external environments and many other genes and internal feedback loops (not shown, and usually unknown). Other biological risk factors, such as endothelial calcification may also be at work. The subtle complexities in such systems have been analyzed extensively by Sing and colleagues (e.g., Perusse et al. 2001; Sing, Haviland, and Reilly 1996). It is no surprise that late-onset effects are difficult to identify or estimate from inherited genotypes. Despite disavowals, tacit genetic determinism is reflected in the naming of genes for diseases such as breast cancer (BRCA), diabetes (NIDDM), and Alzheimer’s disease (presenilin). Here we see the effects of the Lamarckian illusion: we name the gene as if the “function” through which we discover it is its evolutionary reason for being. Usually, that is not even its main function—many genes “for” a particular complex trait are actually ubiquitously expressed. We rivet attention on small susceptibility differences, of little relevance to the evolution of the genes involved.We seem to have little appreciation for our unprecedented good fortune that these diseases occur in large part because we are so healthy that we live far longer than did our evolutionary ancestors. Even the bearers of high-risk alleles at these loci typically thrive healthfully for many decades.Yet, despite pro forma caveats, we still speak of and daily seek out genes “for” these diseases. One view of things is that this theoretical talk about complexity is fine, but that in reality not so horribly many genes are involved. For the sake of discussion, let us grant that the loci affecting risk are not too numerous; that these loci are identified and the relevant variants genotyped; that genotypic risk estimates are accurate; and that a high-risk subset of the population can be identified that might constitute a substantial fraction of all cases (Horrobin 2001a; Pharoah et al. 2002). Even then, because the different genotypes affect risk in different ways, intervention would typically have to be generic rather than genetic (e.g., on cholesterol or blood pressure levels or early detection, much as we do now, rather than on individually specific genetic pathways). And this would have to be done taking into account the effect of diverse environmental factors that temper or exacerbate genetic risk. Preventive intervention in the form of a low-cholesterol diet, for example, might lower some people’s cholesterol, while others’ levels don’t budge. Common diseases do somewhat conceptually change the nature of ascertainment, however, because we tend to confuse two meanings of the word genetics. spring 2003 • volume 46, number 2 173 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n We have been discussing the classic meaning—that is, genes as the units of inheritance, and thus the effect of genotypic variation on phenotypic variation. This usually means we study the patterns of correlation of phenotypes and genotypes among relatives. From this point of view, only those people who inherit specific alleles are particularly vulnerable to a disorder.These alleles are studied by ascertainment on the tail of the genetic effects distribution. The second sense of genetics refers to genes as units of function, that is, the mechanistic role of genes in developmental and physiologic pathways. From this point of view, everyone may be vulnerable to chronic disease, for example, by exposure to levels of substrates for those pathways that overwhelm homeostatic mechanisms that everyone shares. In this case, a knowledge of the pathway may indicate points at which effective intervention may be relevant for the general population and hence for public health. For such traits, ascertainment is uncorrelated with genotype. We cannot tell a priori whether a trait is common for the inherited or functional genetic reason. A disease may be common in a population because some environmental factor affects a particular genetic pathway that is shared by everyone. Many chronic diseases have risen greatly in prevalence because of relatively recent exposures to aspects of modern life like sloth, dietary excess, and chemical carcinogens (e.g.,Trowell and Burkitt 1981). In such cases, essentially everyone is susceptible if exposed. Alternatively, a disease could be common because an underlying genetic variant is, if not shared by everyone, at least common in the human species. (Here, too, the disease could have risen in prevalence because such variants interact with changed environments.) How often common variants are responsible for common complex disease has been the subject of heated debate.The evidence to date—and there is a lot of it—clearly suggests that common variants with major effects on risk are the exception, not the rule, but the “common variant for common disease” notion has itself become common, and major funding and policy decisions have been made in service to it. However, the evidence shows that most often a disease is common because many different, individually rare genetic variants are involved. Under “Normal” Conditions: Gene or Environment? It is important to consider the role of environments in this context. In terms of public health benefits, it seems hard to avoid the inference that while rare allelic variants can overwhelm other factors, environmental factors play a major—probably the major—role in risk for common diseases. A few examples can make the point. A lot is being said these days about genetic influences on Alzheimer’s disease. But anti-inflammatory agents like ibuprofen and cholesterol-lowering agents like statins have been reported to have huge effects on the risk of Alzheimer’s disease—reducing risk by up to around 80 percent (in t’Veld et al. 2001; Jick et al. 2000;Wolozin et al. 2000). Possible mechanisms have been suggested (Simons 174 Perspectives in Biology and Medicine Evolution by Phenotype et al. 2001); this is tentative (e.g., Koudinov, Berezov, and Koudinova 2002), but if such results hold up they dwarf the effects commonly attributed to apolipoprotein (APOE) genotypes.A few alleles in the BRCA1 and BRCA2 genes have dramatic effects on breast cancer risk.These are about as determinative as genetic risk for complex disease can get. However, recent work has shown that even for these dramatic, clear-cut, and severe mutations, lifetime risk varies greatly, depending on the decade when the person was born (Welsch and King 2001); also, among women with the BRCA1 mutation, risk is higher in women who were exposed to oral contraceptives for more than five years, or who used them prior to 1975 or when under age 30 (Narod et al., 2002). Clearly, environmental factors have a significant effect on risk. Further, it has been suggested that the method of case ascertainment itself in these studies has led to overestimates of genetic risk, because ascertaining on multiply affected families will include all the sources of increased risk, most of which are probably unknown or unsuspected.This again raises epistemological issues concerning our understanding of the genetics of disease (Begg 2002). A pandemic of adult (type 2) diabetes and related diseases is in progress in Amerindians and populations with Amerindian admixture (Weiss 1999). These conditions have a particular natural history in Amerindian-related populations that suggests a common genetic background. Numerous gene-mapping studies have identified genes that may contribute to this risk (e.g., Arya et al. 2002a, 2002b; Duggirala et al. 2000, 2001; Ehm et al. 2000; Hanis et al. 1996; Hanson et al. 1995; Horikawa et al. 2000), and the evidence suggests that unidentified genetic factors contribute even more.Yet, 60 years ago these problems were rare in the same populations. Clearly, the most important cause is change in environment or lifestyle—probably involving diet or physical activity—interacting with predisposing genotypes that may comprise an unusual instance of high-frequency genotypes conferring major susceptibility on complex disease. These examples point to a substantial amount of non-genetic inheritance in humans. Children of mothers who had gestational diabetes have a higher risk of disease, at younger ages, than children whose mothers were disease-free during pregnancy, which suggests that something in the uterine environment may affect a person’s risk decades later. But dietary habits are also inherited, leading to secular trends in risk and decreasing age of onset. Those who prefer a gene’s eye view of the world must consider the use of genetic information.The above examples show that phenogenetic relationships can be sensitive to rapid environmental changes. Biotechnology must be able not just to genotype individuals but to estimate future risk, so that interventions can be designed.Yet, risk can only be estimated from past experience, while future environments are impossible to predict—except that they will change unpredictably. Will they evoke susceptibility in genotypes that today appear to be safe? For whom can we confidently recommend difficult preventive measures (like “prophylactic” bilateral mastectomy)? spring 2003 • volume 46, number 2 175 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Conclusion In the 150 years since Huxley bemoaned his failure to see the simplicity of evolutionary explanations, the twin discoveries of evolution and genetics have transformed the life sciences and our understanding of life itself. As so often happens when a science is transformed by sweeping new ideas or technology, strong signals are rapidly identified and a picture falls into place. This describes our success with Mendelian traits—but that success has lured us to extrapolate the behavior of strong effects to that of all effects, and another general experience in science is that extrapolation does not work with equal efficacy across the entire scale-space of relevant phenomena. A number of authors have considered the problem of causal genetic inference for complex biomedical traits (e. g., Beaudet 1999; Emahazion et al. 2001; Holtzman 2001; Holtzman and Marteau 2000; Horrobin 2001b; Millikan 2002; Scriver 2002; Sing, Haviland, and Reilly 1996; Strohman 1997, 2000a, 2000b, 2002; Terwilliger and Goring 2000; Wolf 1995, 1997). Proponents of current approaches sometimes offer measured views, but often only in passing, and overall, the momentum behind strongly Mendelian thinking is difficult to deny or to overcome. The Modern Synthesis was a theory that united to divide.A conceptual union of all biology was made by defining causation as essentially genetic, with the environment and phenotypes something temporary that genes had to slog through to get to the next generation. This gave universal scope to molecular genetic reductionism and provided a systematic research program that suited the traditions of the physical sciences. But that in turn led the conceptual union to be re-divided, all the way down to single nucleotides.That’s where we are now, and how or when a renewed, refreshed, or more effective holism will build organisms back up to a more perfect union is unclear (Laubichler 2000).The job will require perceptive re-thinking. In the meantime, we have misremembered the Central Dogma. It is about the mechanistic relationship of genes to polypeptides, not phenotypes, and it works best when the latter two are closely related and predominate over other aspects of causation.We got here via Mendel, who deliberately chose well-behaved traits to work with. He was clever enough to avoid complex traits—and even then he was a bit lucky (Weiss 2002). If phenotypes can’t always be accurately predicted from genotypes, the converse presents even greater challenges, because successful gene mapping requires the ability to predict underlying genotype (G) from observed phenotype (P) (Weiss and Terwilliger 2000).The causal arrow (G→P) does not imply the inferential one (G←P). Weak G←P relationships explain much of the problem encountered in complex disease mapping.This is a biological fact, not a technological limitation. The same is true with regard to natural selection: if scientists cannot screen effectively on genotypes via ascertainment of phenotypes, neither 176 Perspectives in Biology and Medicine Evolution by Phenotype can selection.We can’t expect selection to have refined genetic causation for our convenience. This may go against the faith, but it is at least worth taking seriously as we endlessly launch ever more costly attempts at the Sisyphean mountain of complexity. One justification proffered for current approaches is we are merely attempting to assess the reaction norms of disease-related genes across the array of lifestyle environments. But even this modest objective is somewhat illusory. In essence we are only studying responses to the particular limited range of the last few decades of exposures, to rapidly and unpredictably changing environmental variants usually not identified or measured in genetic studies.We routinely treat genotypes and environments as separate, replicable entities whose effects can be regressed on each other (Marx 2002; Strohman 2002; Willett 2002). The true relationships are probably more subtle and seamless—not least because we modify our environments and transmit them culturally, such as by jogging or eating less fat, based on knowledge that we think will alter disease risk itself (e.g., by exercise or diet; Lewontin 2000; Moore 2001; Oyama 2000). The points we raise are not new, and a common reaction is that “everybody knows” them. But if they are not integrated into practice—and policy—how well does everybody really know what “everybody knows”? There will always be seductive exceptions, but an evolutionary perspective helps us see why genetic variation may not adequately explain the subtle variation in complex traits that is the target of so much of our research. That this is not really understood (or honestly presented) is shown by the widespread promises of genetically personalized medicine (your risk on a chip). These considerations have societal implications. From a public health point of view, genetic approaches to complex disease should be pursued where they are most appropriate or could have the most impact on the population that pays for them. The caveats we have raised do not promise solutions, but they do lead to a few suggestions: 1. It is potentially easier and less costly to alter environment than genotype, especially on a population scale, a point made more than once in these pages (e.g.,Weiss and Schull 2002).The residuum of recalcitrant cases that really are genetic in the usual Mendelian sense are appropriate targets for gene-based research investment. 2. A common justification for “hypothesis free” genome scanning is to find pathways involved in complex traits, on the grounds that known candidate genes have not fared well.Yet candidate genes got that status for good reasons, and what mapping studies do is generate more of them. There are now more direct, tissue-specific, expression-based ways to find pathways lurking within the genome.We no longer need to rely on the caprices of phenotypic variation in families. spring 2003 • volume 46, number 2 177 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n 3. There may be some traits whose basic biology remains so mysterious that current approaches are the best available way to open the door. Devastating early-onset psychiatric diseases may be examples. But we can expect complexity to continue to bedevil our efforts. 4. Perhaps it is time to demonstrate with some accountability that genetic knowledge can actually deliver the health miracles that we have been promised. Proof of principle could be achieved by intense, programmatic investment in a model complex trait for which we already have many candidate genes. If genetic approaches actually work there, it will be clearly justified to fund them for other traits. Should we start with, say, the 150 obesity genes? 5. We are swimming in an epistemological maelstrom yet seem unwilling to acknowledge the depths of the problem. Both our genetic approaches and the questions we ask of them may be inapt.The situation is compounded by an essentially identical history of attempting to decompose the same traits in terms of environmental risk factors. Current “complexity” schools of thought may be faddish (Lewontin 2000), but they have a point, and they have amply shown that even relatively simple causation can be inferentially problematic (Wolfram 2002).We lack adequate theory for observational units that are each unique rather than replicable (Molenaar, Huizenga, and Nesselroade, in press), or for when unmeasured phenomena have as much causal impact as those we know about, like unspecified secular trends in exposure and diagnostic criteria. Rather than continuing to tinker with existing approaches, a mobilized effort to understand these epistemological rather than technical problems in the underlying notions of causation and inference themselves would be warranted. Change will probably have to come from the young. We know that even this paper is largely reductionist in phrasing. We have written of disease alleles, of environment, genes, and interactions, in rather loose ways as separable, replicable causal elements. It is not easy to escape from a paradigm. At least, we have tried to state a tempering perspective in regard to complex traits based on simple and rather obvious aspects of evolution, in order to show why current frustrations are explicable and even to be expected. These are difficult problems to solve by any means, so impatience may be unfair. Certainly much knowledge comes from looking into the basic science underlying human traits. But the cost is high, especially if we have good reason to believe we are looking in the wrong place. In regard to the two meanings of genetics: because of evolution, genetics is involved in everything; but because of evolution by phenotype, not everything is genetic. 178 Perspectives in Biology and Medicine Evolution by Phenotype References Arya, R., et al. 2002a. Factors of insulin resistance syndrome: Related phenotypes are linked to genetic locations on chromosomes 6 and 7 in nondiabetic Mexican-Americans. Diabetes 51:841–47. Arya, R., et al. 2002b. Linkage of high-density lipoprotein-cholesterol concentrations to a locus on chromosome 9p in Mexican Americans. Nat. Genet. 30:102–5. Beaudet, A. L. 1999. 1998 ASHG Presidential address. Making genomic medicine a reality. Am. J. Hum. Genet. 64:1–13. Begg, C. B. 2002. On the use of familial aggregation in population-based case probands for calculating penetrance. JNCI 94(16):1221–26. Brockmann, G. A., and M. R. Bevova. 2002. Using mouse models to dissect the genetics of obesity. Trends Genet. 18:367–76. Clark, A. G. 1998. Mutation-selection balance with multiple alleles. Genetica 102:41–47. Darwin, C. 1859. On the origin of species by means of natural selection. London: John Murray. Rpt. Cambridge: Harvard Univ. Press, 1964. Duggirala, R., et al. 2000. A major susceptibility locus influencing plasma triglyceride concentrations is located on chromosome 15q in Mexican Americans. Am. J. Hum. Genet. 66:1237–45. Duggirala, R., et al. 2001. A major locus for fasting insulin concentrations and insulin resistance on chromosome 6q with strong pleiotropic effects on obesity-related phenotypes in nondiabetic Mexican Americans. Am. J. Hum. Genet. 68:1149–64. Ehm, M. G., et al. 2000. Genomewide search for type 2 diabetes susceptibility genes in four American populations. Am. J. Hum. Genet. 66:1871–81. Emahazion,T., et al. 2001. SNP association studies in Alzheimer’s disease highlight problems for complex disease analysis. Trends Genet. 17:407–13. Finch, C. E., and T. B. L. Kirkwood. 2000. Chance, development, and aging. New York: Oxford Univ. Press. Fortin, A., M. M. Stevenson, and P. Gros. 2002. Complex genetic control of susceptibility to malaria in mice. Genes Immunity 3:177–86. Goring, H. H., J. D.Terwilliger, and J. Blangero. 2001. Large upward bias in estimation of locus-specific effects from genomewide scans. Am. J. Hum. Genet. 69:1357–69. Gould, S. J., and E. A. Lloyd. 1999. Individuality and adaptation across levels of selection: How shall we name and generalize the unit of Darwinism? Proc. Natl. Acad. Sci. USA 96:11904–9. Guldberg, P., et al. 1996. Phenylalanine hydroxylase gene mutations in the United States: Report from the Maternal PKU Collaborative Study. Am. J. Hum. Genet. 59:84–94. Hanis, C. L., et al. 1996. A genome-wide search for human non-insulin-dependent (type 2) diabetes genes reveals a major susceptibility locus on chromosome 2. Nat. Genet. 13:161–66. Hanson, R., et al. 1995. Segregation analysis of non-insulin-dependent diabetes mellitus in Pima Indians: Evidence for a major-gene effect. Am. J. Hum. Genet. 57:160–70. Harpending, H. C., et al. 1998. Genetic traces of ancient demography. Proc. Natl. Acad. Sci. USA 95:1961–67. Hartl, D. L., and R. B. Campbell. 1982.Allele multiplicity in simple Mendelian disorders. Am. J. Hum. Genet. 34:866–73. spring 2003 • volume 46, number 2 179 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Hartl, D. L., and A. G. Clark. 1997. Principles of population genetics. Sunderland, MA: Sinauer. Holtzman, N. A. 2001. Putting the search for genes in perspective. Int. J. Health Serv. 31: 445–61. Holtzman, N.A., and T. M. Marteau. 2000.Will genetics revolutionize medicine? N. Engl. J. Med. 343:141–44. Horikawa,Y., et al. 2000. Genetic variation in the gene encoding calpain-10 is associated with type 2 diabetes mellitus. Nat. Genet. 26:163–75. Horrobin, D. F. 2001a. Realism in drug discovery: Could Cassandra be right? Nat. Biotechnol. 19:1099–1100. Horrobin, D. F. 2001b. Something rotten at the core of science? Trends Pharmacol. Sci. 22: 51–52. Human Gene Mutation Database (HGMD). 2002. <http://www.uwcm.ac.uk/uwcm/ mg/hgmd0.html>. in t’ Veld, B. A., et al. 2001. Nonsteroidal antiinflammatory drugs and the risk of Alzheimer’s disease. N. Engl. J. Med. 345:1515–21. Ioannidis, J. P., C. H. Schmid, and J. Lau. 2000. Meta-analysis in hematology and oncology. Hematol. Oncol. Clin. North Am. 14:973–91. Ioannidis, J. P., et al. 2001. Replication validity of genetic association studies. Nat. Genet. 29:306–9. Jick, H., et al. 2000. Statins and the risk of dementia. Lancet 356:1627–31. Jorde, L. B., M. Bamshad, and A. R. Rogers. 1998. Using mitochondrial and nuclear DNA markers to reconstruct human evolution. Bioessays 20:126–36. Jorde, L. B.,W. S.Watkins, and M. J. Bamshad. 2001. Population genomics: A bridge from evolutionary history to genetic medicine. Hum. Mol. Genet. 10:2199–207. Jorde, L. B., et al. 2000. The distribution of human genetic diversity: A comparison of mitochondrial, autosomal, and Y-chromosome data. Am. J. Hum. Genet. 66:979–88. Kayaalp, E., et al. 1997. Human phenylalanine hydroxylase mutations and hyperphenylalaninemia phenotypes: A metanalysis of genotype-phenotype correlations. Am. J. Hum. Genet. 61:1309–17. Koudinov, A. R., T. T. Berezov, and N.V. Koudinova. 2002. Cholesterol and Alzheimer’s disease: Is there a link? Neurology 58:1135. Laubichler, M. D. 2000.The organism is dead: Long live the organism! Persp. Sci. 8:186– 315. Lewontin, R. C. 2000. The triple helix. Cambridge: Harvard Univ. Press. Mackay,T. F. 2001a.The genetic architecture of quantitative traits. Annu. Rev. Genet. 35: 303–39. Mackay,T. F. 2001b. Quantitative trait loci in Drosophila. Nat. Rev. Genet. 2:11–20. Marx, J. 2002. Unraveling the causes of diabetes. Science 296:686–89. Mayr, E. 1982. The growth of biological thought: Diversity, evolution, and inheritance. Cambridge: Belknap Press. Mayr, E. 1991. One long argument: Charles Darwin and the genesis of modern evolutionary thought. Cambridge: Harvard Univ. Press. Mayr, E. 1997.The objects of selection. Proc. Natl. Acad. Sci. USA 94:2091–94. Millikan, 2002. The changing face of epidemiology in the genomics era. Epidemiology 13(4):472–80. 180 Perspectives in Biology and Medicine Evolution by Phenotype Molenaar, P. C. M., H. M. Huizenga, and J. R. Nesselroade. In press. The relationship between the structure of inter-individual and intra-individual variablity:A theoretical and empirical vindication of developmental systems theory. In Understanding human development, ed. U. M. Staudinger and U. E. R. Lindenberger. Dordrecht: Kluwer Academic. Moore, D. 2001. The dependent gene. New York: Freeman. Narod, S.A., et al. 2002. Oral contraceptives and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. J. Natl. Cancer Inst. 94(23):1773–79. Online Mendelian Inheritance in Man (OMIM). 2002. <http://www3.ncbi.nlm.nih. gov/omim>. Oyama, S., ed. 2000. The ontogeny of information: Developmental systems and evolution. Durham: Duke Univ. Press. Perusse, L., et al. 2001.The human obesity gene map:The 2000 update. Obes. Res. 9:135– 69. Pharoah, P. D., et al. 2002. Polygenic susceptibility to breast cancer and implications for prevention. Nat. Genet. 31:33–36. Phenylalanine Hydroxylase Data Base (PAHdb). 2002. <http://data.mch.mcgill.ca/ pahdb_new/>. Rankinen,T., et al. 2002.The human obesity gene map: The 2001 update. Obes Res. 10: 196–243. Reeve, H. K., and P. W. Sherman. 1993. Adaptation and the goals of evolutionary research. Q. Rev. Biol. 68:1–32. Schlichting, C., and M. Pigliucci. 1998. Phenotypic evolution: A reaction norm perspective. Sunderland, MA: Sinauer. Scriver, C. R. 2002. Does hereditary metabolic disease modulate senescence and aging? J. Inherit. Metab. Dis. 25(3):235–51. Scriver, C. R., and P. J.Waters. 1999. Monogenic traits are not simple: Lessons from phenylketonuria. Trends Genet. 15:267–72. Scriver, C. R., et al. 1996.The phenylalanine hydroxylase locus: A marker for the history of phenylketonuria and human genetic diversity. PAH Mutation Analysis Consortium. Ciba Found Symp 197:73–90; discussion 90–96. Scriver, C. R., et al., eds. 2001. The metabolic and molecular basis of inherited disease. New York: McGraw-Hill. Simons, M., et al. 2001. Cholesterol and Alzheimer’s disease: Is there a link? Neurology 57: 1089–93. Sing, C. F., M. B. Haviland, and S. L. Reilly. 1996. Genetic architecture of common multifactorial diseases. Ciba Found Symp 197:211–32. Strohman, R. 1997. The coming Kuhnian revolution in biology. Nat. Biotechnol. 15:194– 200. Strohman, R. 2000a.We need a metaphor to explain life’s mystery. Nature 408:767–68. Strohman, R. 2000b. Organization becomes cause in the matter. Nat. Biotechnol. 18:575–76. Strohman, R. 2002. Maneuvering in the complex path from genotype to phenotype. Science 296:701–3. Terwilliger, J. D., and H. H. Goring. 2000. Gene mapping in the 20th and 21st centuries: Statistical methods, data analysis, and experimental design. Hum. Biol. 72:63–132. Thornhill, R. 1990. The study of adaptation. In Interpretation and explanation in the study of behavior, ed. M. Bekoff and D. Jamieson, 31–62. Boulder:Westview Press. spring 2003 • volume 46, number 2 181 K e n n e t h M . W e i s s a n d A n n e V. B u c h a n a n Trowell, H. C., and D. P. Burkitt. 1981. Western diseases, their emergence and prevention. Cambridge: Harvard Univ. Press. Vogel, F., and A. G. Motulsky. 1997. Human genetics: Problems and approaches. Berlin: Springer. von Haeseler,A.,A. Sajantila, and S. Paabo. 1996.The genetical archaeology of the human genome. Nat. Genet. 14:135–40. Weatherall, D. J. 2001. Phenotype-genotype relationships in monogenic disease: Lessons from the thalassaemias. Nat. Rev. Genet. 2:245–55. Weiss, K. M. 1999. Genetic variation and human disease. Cambridge: Cambridge Univ. Press. Weiss, K. M. 2002. Goings on in Mendel’s garden. Evol. Anthropol. 40–44. Weiss, K. M., and S. M. Fullerton. 2000. Phenogenetic drift and the evolution of genotype-phenotype relationships. Theor. Popul. Biol. 57:187–95. Weiss, K. M., and W. J. Schull. 2002. Perspectives fulfilled: The work and thought of J.V. Neel (1915–2000). Perspect. Biol. Med. 45:46–64. Weiss, K. M., and J. D. Terwilliger. 2000. How many diseases does it take to map a gene with SNPs? Nat. Genet. 26:151–57. Welsch, P. L., and M. C. King. 2001. BRCA1 and BRCA2 and the genetics of breast and ovarian cancer. Hum. Mol. Genet. 10:705–13. Wickner, S., M. R. Maurizi, and S. Gottesman. 1999. Posttranslational quality control: Folding, refolding, and degrading proteins. Science 286:1888–93. Willett, W. C. 2002. Balancing life-style and genomics research for disease prevention. Science 296:695–98. Wolf, U. 1995.The genetic contribution to the phenotype. Hum. Genet. 95:127–48. Wolf, U. 1997. Identical mutations and phenotypic variation. Hum. Genet. 100:305–21. Wolfram, S. 2002. A new kind of science. Champaign, IL:Wolfram Media. Wolozin, B., et al. 2000. Decreased prevalence of Alzheimer disease associated with 3hydroxy-3-methyglutaryl coenzyme A reductase inhibitors. Arch. Neurol. 57:1439–43. Wright, S. 1968–1978. Evolution and the genetics of populations. 4 vols. Chicago: Univ. of Chicago Press. Yasui, A., and S. J. McCready. 1998. Alternative repair pathways for UV-induced DNA damage. Bioessays 20:291–97. 182 Perspectives in Biology and Medicine