Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Electrocardiography wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Artificial heart valve wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Aortic stenosis wikipedia , lookup
Cardiac surgery wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
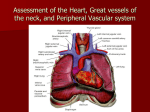
Heart & Neck Vessels CHAPTER 19 - JARVIS Overview Neck Carotid pulse – observe and palpate Observe jugular venous pulse Estimate jugular venous pressure Precordium Inspection and palpation Describe location of apical pulse Note any heave (lift) or thrill Auscultation Identify anatomic areas noting rate and rhythm Listen in systole and diastole for murmurs Repeat with bell Listen at apex and base Cardiovascular System Consists of the Heart and Blood Vessels Position & Surface Landmarks Precordium: area on anterior chest directly overlying the heart and great vessels Mediastinum: area between the lungs in the middle third of the thoracic cage Heart: top is the broader base & bottom is the apex Apical Impulse: 5th intercostal space, 7-9cm from midsternal line Great Vessels: superior & inferior vena cava; pulmonary artery; pulmonary veins; aorta Position & Surface Landmarks Heart Wall, Chambers, & Valves Heart Wall: Pericardium, Myocardium, & Endocardium Chambers: Atria & Ventricles; right & left Valves Atrioventricular Semi lunar Blood Flow Blood flow animation Heart Sounds Conduction P wave: depolarization of aorta PR interval: beginning of P wave to beginning of QRS (atrial depolarization & impulse through AV node) QRS complex: depolarization of ventricles T wave: repolarization of ventricles Conduction You tube Pumping Ability Cardiac Output: normally 4-6 Liters of blood per minute Cardiac Output = Stroke Volume x Rate Preload: venous return that builds during diastole; ventricular muscle is stretched before contraction Afterload: opposing pressure the ventricle must generate to open the aortic valve against the higher aortic pressure; resistance against which ventricle must pump its blood Neck Vessels Carotid Arteries Jugular Veins: Internal and external History: Subjective Data Chest pain Nocturia Dyspnea Past cardiac history Orthopnea Family cardiac history Cough Personal habits (cardiac Fatigue Cyanosis or pallor Edema risk factors) Objective Data Neck Vessels Neck Vessels Inspect Jugular Venous Pulse – assessing central venous pressure Stand on patient’s right side Position patient supine from 30-45 degree angle; Pulsation may be seen the sternal notch At 45 degree angle, jugulars should disappear Inspect carotid pulsations Neck Vessel Exam Neck Vessels Palpate Carotid Artery One at a time Avoid excessive pressure Normal: smooth with 2+ strength Auscultate Carotid Artery Listen for presence of bruit (blowing or swishing sound) Apply bell of the stethoscope at angle of jaw, midcervical area, and base of the neck Person can take breath, exhale, and hold while you listen so no sound is masked Neck Vessels Jugular Venous Pressure Use angle of Louis as arbitrary reference point, and compare it with highest level of venous pulsation Hold a vertical ruler on sternal angle Align a straight edge on ruler like a T-square, and adjust level of horizontal straight edge to level of pulsation Read level of intersection on vertical ruler; normal jugular venous pulsation is 2 cm or less above sternal angle State person’s position, e.g., “internal jugular vein pulsations 3 cm above sternal angle when elevated 30 degrees” Chest Inspect Anterior Chest Pulsations: may or may not see apical impulse at 4th intercostal space at or inside the midclavicular line Palpate the Apical Impulse Ask the person to exhale and hold Use 1 finger pad Note: location (4th or 5th intercostal space), size (1 x 2 cm), amplitude (short, gentle tap), duration (short) May not be palpable in all adults Chest Palpate Across Precordium Use palmar aspects of 4 fingers, or ulnar surface of hand and gently palpate Normally no findings Percussion Used to outline the heart’s border Not done as much because of availability of chest xray and/or echocardiography Chest Auscultation 4 traditional valve “areas” 2nd right interspace – aortic valve area 2nd left interspace – pulmonic valve area Left lower sternal border – tricuspid valve area 5th interspace, left midclavicular line – mitral valve area Auscultate in Z pattern from base of heart, across and down, then over to apex Traditionally Aortic area, pulmonic area, Erb’s point, tricuspid area, mitral area “ APE –To-Man” Chest Chest Rate: 50-90 bpm Rhythm: regular Heart Sounds http://www.wilkes.med.ucla.edu/i nex.htm Identify S1 & S2: lub-dup S1 louder at apex = closure of AV valves, beginning of systole S2 louder at base = closure of semilunar valves Focus on systole, then diastole, then listen for extra heart sounds Listen for murmurs Describe by timing, loudness, pitch, pattern, quality, location, radiation, posture Variation in S1 Factors: Position of AV valve at start of systole, change in valve structure, & pressure in the ventricles 1. Loud S1 2. Faint S1 3. Varying Intensity of S1 4. Split S1 Variations in S2 Accentuated S2 Diminished S2 Split S2 Normal: occurs during inspiration Fixed Split: unaffected by respiration Paradoxical Split: occurs during expiration Wide Split: wide on inspiration and still present with expiration Extra Systolic Sounds Ejection Click: sound of the SL valves opening; best heard with diaphragm; aortic at 2nd right interspace and apex; pulmonic at 2nd left interspace Aortic Prosthetic Valve Sounds: early systolic sound Midsystolic Click: associated with mitral valve prolapse; sound is short and high pitched; best heard with the diaphragm at the apex; Extra Diastolic Sounds Early Diastole Opening Snap: opening of AV valves Mitral Prosthetic Valve Sound: opening click just after S2 Mid-diastole Third Heart Sound: S3 – ventricular filling sound, low pitched, like “distant thunder”; heard at the apex or left lower sternal border with the bell Physiologic: frequently heard in children and young adults; disappears when sitting up Pathologic: Ventricular Gallop – indicates decreased compliance of the ventricles (heart failure) Discuss how you differentiate an S3 from a Split S2 Extra Diastolic Sounds Late Diastole Fourth Heart Sound: S4 – ventricular filling sound, soft and low pitched; heard at the apex with person in left lateral position with the bell Physiologic: found in adults older than 40 Pathologic: Atrial Gallop – decreased compliance of the ventricles (CAD, cardiomyopathy, systemic HTN) Summation Sound: S3 & S4 present Extra Cardiac Sounds Pericardial Friction Rub: inflammation of the pericardium; high pitched and scratchy best heard with the diaphragm Murmurs Identified by Where they are heard on the chest Where they occur in the cardiac cycle- Systolic/Diastolic Loudness- graded I-VI Pitch- low to high Variation in loudness- Crescendo/Decrescendo, pan Systolic Murmurs Aortic Stenosis: loud, harsh, midsystolic; loudest at 2nd right interspace Pulmonic Stenosis: medium, coarse, systolic; loudest at 2nd left interspace Mitral Regurgitation: pansystolic, loud, blowing; loudest at apex Triscupid Regurgitation: pansystolic, soft, blowing; loudest at left lower sternal boarder Diastolic Murmurs Mitral Stenosis: low-pitched, diastolic; best heard at the apex with person in left lateral position Tricuspid Stenosis: rumbling, diastolic; best heart at left lower sternal boarder, louder on inspiration Aortic Regurgitation: soft, high-pitched, blowing, diastolic; best heard at 3rd left interspace at the base Pulmonic Regurgitation: same as aortic regurgitation Developmental Considerations Infants Subjective Mother’s health during pregnancy Any cyanosis Growth Activity Objective Fetal shunts close between 10-15 hours but may take up to 48 hours (may have murmurs until shunts close) Apical impulse: palpate at the 4th intercostal space, lateral to the midclavicular line Heart rate: 120-140 bpm Sinus arrhythmia with respirations S2 higher pitched and sharper than S1 Children: Subjective Growth Activity Unexplained joint pain or fevers (strep throat, rheumatic fever) Frequent headaches or nosebleeds Frequent respiratory infections Family History Children: Objective Signs of heart disease: poor weight gain, developmental delay, persistent tachycardia, tachypnea, dyspnea on exertion, cyanosis, clubbing Apical impulse may be visible 4th intercostal space left of the midclavicular line until age 4; 4th intercostal space at midclavicular line age 4-6; 5th intercostal space right of midclavicular line at age 7; Heart rate slows down Sinus arrhythmia common; Physiologic S3 is common Venous hum is common Heart murmurs may occur and are functional Pregnant Woman: Subjective Blood pressure Usual blood pressure before pregnancy Blood pressure during pregnancy Treatments Associated symptoms Fainting or Dizziness Pregnant Woman: Objective Resting pulse rate increase of 10-15 bpm Blood pressure 2nd trimester, 3rd trimester Apical impulse higher and lateral than normal Increased blood volume causes: Exaggerated splitting of S1, increased loudness of S1 Loud S3 Heart murmurs Aging Adult: Subjective Heart or lung disease Treatment Symptoms Medications for any illness Environment Aging Adult: Objective Gradual rise in systolic blood pressure is common Orthostatic hypotension AP chest diameter increases Carotid artery stenosis S4 may occur with no known cardiac disease S3 indicates heart failure Systolic murmurs are common ABNORMAL FINDINGS Heart Failure Decreased cardiac output due to the heart pump failing Dilated pupils Gray, pale, or cyanotic skin; cool skin Anxiety or confusion Decreased O2 saturation Dyspnea Orthopnea Jugular vein distention Crackles/Wheezes in the lungs Cough Weak pulse Decreased blood pressure S3 gallop/ tachycardia Nausea and vomiting Ascites Edema Fatigue Enlarged spleen and liver Decreased urine output Congenital Heart Defects Atrial Septal Defect (ASD): abnormal opening in the atrial septum, results in left-to-right shunting Ventricular Septal Defect (VSD): abnormal opening in the septum between ventricles Tetralogy of Fallot: shunts venous blood into the aorta, blood is not being oxygenated; severe cyanosis Coarctation of the Aorta: severe narrowing of the aorta