Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
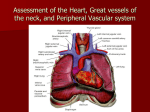
LEARNING GUIDE FOR CARDIAC EXAMINATION Steps / Tasks GET READY Stand to the right of the patient’s bed. Prepare your stethoscope with bell (cone) and diaphragm. Explain the procedure to the patient. Be sure that your hands are warm if not, rub your hands. Put the patient in supine position, if he is orthopnic put him in semisitting position. 6- Ensure good lighting. 7- Expose chest well. 12345- INSPECTION OF THE PRECORDIUM 1234- Look tangentially, from the foot end of the patient, for precordial bulge. Look for dilated veins on the chest wall or any thoracic cage abnormalities. Look tangentially, from the side of the patient for apical pulsation. Look tangentially, from the side of the patient for other pulsations in suprasternal, aortic and pulmonary areas, parasternal, and epigasrium. 5- Comment on: o Precordial bulge or any thoracic cage abnormalities o Site of apex beat o Other pulsations PALPATION OF THE PRECORDIUM 1- Localize the apex beat by inspection. 2- Palpate apex by palmer surface of the hand. 3- Localize the apex (the lowermost outermost powerful pulsation) with the tip of your index finger. 4- Put the patient in the left lateral position to assess the character of the apex. 5- Palpate the left parasternal area using the palmer aspect of your right hand for thrills. 6- Then using the palmer aspect at the base of metacarpals confirm presence of parasternal heave. 7- Put the tips of your fingers in the second left intercostal space to elicit palpable second sound (diastolic shock). 8- Place the palm of your right hand on the epigastrium and slide your fingers under the rib cage to palpate epigastric pulsation. Aortic pulsation thrust forward against the palmer surface of your fingers. The pulsation of enlarged liver thrust downwards against your finger tips. 9- Comment on: A-Apex: 1- Site 2-Character: 3-Thrill 4-Palpable gallop B-Palpable diastolic shock C-Parasternal thrill or heave D-Epigasteric pulsation PERCUSSION OF THE PRECORDIUM 1- Place your left hand on the right side of the chest wall with pleximeter parallel to the right border of the heart, palm downwards with fingers slightly separated. 2- Struck the center of the second phalanx of the middle finger sharply with the tip of the pad of the right middle finger with the movement coming from the wrist joint. 3- Start from resonant to dull in the right third, fourth and fifth intercostal spaces to define the right cardiac border. 4- Start from resonant to dull in the left third, fourth and fifth intercostal spaces to define the left cardiac border. 5- Start from resonant to dull in the second right intercostal spaces to define the dullness in the aortic area. 6- Start from resonant to dull in the second left intercostal spaces to define the dullness in the pulmonary area. 7- Percuss directly over the lower half of the sternum using the tip of the index finger to define dullness of right ventricular hypertrophy. 8- Percuss outside the apex. 9- Comment on the size of the heart and the great vessels. AUSCULTATION OF THE PRECORDIUM 1- Auscultate the base of the heart starting from the first aortic area (second right itercostal space). 2- Move stethoscope to the pulmonary area (second left itercostal space). 3- Move stethoscope to the second aortic area (third left itercostal space). 4- Move stethoscope down left sternal border. 5- Move stethoscope to tricuspid area (lower left sternal border). 6- Move stethoscope to mitral area (fifth left itercostal space). 7- Move stethoscope to axilla. 8- Listen first with the diaphragm for high pitched sounds (first and second heart sounds, mitral regurge, aortic regurge and rub). Time with the carotid pulse. 9- Then listen by the cone (bell) for low pitched sounds (third and forth heart sounds and mitral stenosis). Time with the carotid pulse. 10- Ask the patients to roll onto his left side. 11- Find the apical impulse. 12- Auscultate the apex with the bell. 13- Ask the patient to sit up, lean forward, exhale completely and hold breath in expiration. Listen to aortic areas down the left sternal border to the apex. 14- While the patient is sitting evaluate the splitting of the second sound in the pulmonary area (second left itercostal space). 15- Comment on: A- First and second heart sounds B- Added sounds (third and forth heart sounds, opening snap of mitral stenosis). C- Presence of murmur. If present comment on: 1-site 2-radiation 3-pitch 4-intensty 5-relation to respiration, position and exercise