Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
DNA vaccination wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Adaptive immune system wikipedia , lookup
Gluten immunochemistry wikipedia , lookup
Innate immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
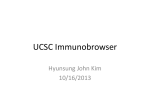
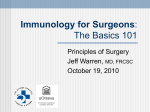
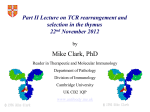
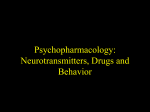
Available online at www.sciencedirect.com Neurotransmitters activate T-cells and elicit crucial functions via neurotransmitter receptors Mia Levite1,2 Neurotransmitters are traditionally viewed as nerve-secreted molecules that trigger or inhibit neuronal functions. Yet, neurotransmitters bind also their neurotransmitter receptors in T-cells and directly activate or suppress T-cell functions. This review focuses only on the activating effects of neurotransmitters on T-cells, primarily naı̈ve/resting cells, and covers dopamine, glutamate, serotonin, and few neuropeptides: GnRH-I, GnRH-II, substance P, somatostatin, CGRP, and neuropeptide Y. T-cells express many neurotransmitter receptors. These are regulated by TCR-activation, cytokines, or the neurotransmitters themselves, and are upregulated/downregulated in some human diseases. The context — whether the T-cells are naı̈ve/resting or antigen/mitogen/cytokine-activated, the T-cell subset (CD4/CD8/Th1/Th2/Teff/Treg), neurotransmitter dose (low/optimal or high/excess), exact neurotransmitter receptors expressed, and the cytokine milieu — is crucial, and can determine either activation or suppression of T-cells by the same neurotransmitter. T-cells also produce many neurotransmitters. In summary, neurotransmitters activate vital T-cell functions in a direct, potent and specific manner, and may serve for communicating between the brain and the immune system to elicit an effective and orchestrated immune function, and for new therapeutic avenues, to improve T-cell eradication of cancer and infectious organisms. Addresses 1 The School of Behavioral Sciences, The Academic College of Tel-AvivYaffo, Israel 2 Department of Neurobiology, the Weizmann Institute of Science, Rehovot 76100, Israel Corresponding author: Levite, Mia ([email protected]) Current Opinion in Pharmacology 2008, 8:460–471 This review comes from a themed issue on Immunomodulation Edited by Mia Levite and John Gordon potently activate vital human T-cell functions needed for the T-cells to perform their specialized tasks, such as cytokine secretion, adhesion to extracellular matrix (ECM), chemotactic migration and homing into specific organs and eradication of infectious organisms and cancer cells ([1,2,3,4,5,6,7], most of the additional studies cited in this review, and others) (Tables 1 and 2, Figures 1–3). In fact, both activating and suppressing effects of neurotransmitters on T-cells were reported, depending on the neurotransmitter itself, as well as on all the parameters discussed below and shown schematically in Figure 4. For maintaining clarity, brevity, and focus in this review, and because of space limitations, the present review will deal with only one type of immune cells: T-cells, and cover only the activation of these cells by certain neurotransmitters. To stay away from misleading generalizations, the review will NOT elaborate on various other effects of either the same or other neurotransmitters on diverse immune cells (such as B cells, dendritic cells, stem cells, neutrophils, macrophages, natural killer monocytes, mast), and will NOT cover the suppressive effects of some neurotransmitters on T-cell function. Tables 1 and 2 cover for example three ‘small’ neurotransmitters: dopamine, glutamate and serotonin, and four peptidergic neurotransmitters (i.e. neuropeptides): GnRH-I, GnRH-II, Substance P, and Somatostatin and show: first, their main function in the brain; second, their known receptors in the body; third, their receptors expressed in T-cells; fourth, some of the T-cell functions these neurotransmitters (or their receptor agonists) activate, when they bind naı̈ve/resting T-cells; and fifth, potential relevance to human disease, i.e. the reported abnormal expression of certain neurotransmitter receptors in T-cells, or the abnormal T-cell response to these neurotransmitter, reported in few human diseases. Available online 23rd June 2008 1471-4892/$ – see front matter # 2008 Elsevier Ltd. All rights reserved. DOI 10.1016/j.coph.2008.05.001 Introduction It is undoubtedly clear now that many neurotransmitters can bind to their neurotransmitter receptors expressed not only in various ‘classical’ target cells within the central or peripheral nervous system, but also in T-cells, and can Current Opinion in Pharmacology 2008, 8:460–471 Neurotransmitters A substance is conventionally viewed as a neurotransmitter, if the following four criteria are met: first, it is synthesized in neurons; second, it is present in the presynaptic terminal and released in amounts sufficient to exert a defined action on the postsynaptic neuron or effector organs; third, when administered exogenously (as a drug) in reasonable concentrations, it precisely mimics the action of the endogenously released transmitter; and fourth, a specific mechanism exists for its removal from its site of action (the synaptic cleft). www.sciencedirect.com Neurotransmitters activate T-cells Levite 461 Table 1 Three examples of neurotransmitters that can directly activate naı̈ve/resting human T-cells: Their main function and receptors in the brain, receptors in T-cells, activating effects on T-cells, and abnormal expression/function of the receptors in T-cells in human diseases Dopamine Dopamine effects in the brain: Regulation of movement and involvement in psychoses Dopamine receptors expressed in the brain: Dopaminergic receptors D1, D2, D3, D4, D5 Dopamine receptors expressed in various T-cells: Primarily D3 and D2, but also D1/5 and D4, depending on the T-cell subpopulation and activation state [7,10,15,16,–21,42] Among the human T-cell functions activated/enhanced by Dopamine: (1) Induction of integrin-mediated adhesion to fibronectin of human T-cells [10]; (2) Production of TNFa mRNA and secretion of TNFa (primarily via D3R) [7]; (3) Production of IL-10 mRNA and secretion of IL-10 (primarily via D2R) [7]; (4) Induction of integrin-mediated adhesion of naı̈ve CD8+ T-cells to fibronectin and ICAM-1 [21]; (5) Induction of chemotactic responses of naı̈ve CD8+ T-cells and their attraction to the peritoneal cavity [21]; (6) Induction of Th2 to Th1 shift in cytokine secretion upon stimulation of activated T-cells by dopaminergic agonist [24]; (7) Suppression of regulatory T-cells (Treg) which subsequently releases Treg inhibition on T effector cells [13,22] Abnormal expression or function of Dopamine receptors in T-cells in human diseases: Schizophrenia [23–25]; Parkinson’s disease [27]; Alzheimer’s disease [17]; Migrane (cited within [17]) and Multiple sclerosis [31] Glutamate Glutamate effects in the brain: The brain’s primary excitatory neurotransmitter, involved in affective, sensory, and motor function, learning, memory, cognition, and synaptic plasticity Glutamate receptors expressed in the brain: Ionotropic glutamate receptors: NMDA, AMPA, and Kainite; Metabotropic glutamate receptors mGluR1, 2, 3, 4, 5, 6, 7 Glutamate receptors expressed in various T-cells: Ionotropic: AMPA GluR3 in normal, leukemia and encephalitogenic anti-MBP T-cells from mice, healthy individuals and MS patients [6,11,33]; AMPA and Kainate [32]; Metabotropic: mGlu1R, mGlu5R [43] Among the human T-cell functions activated/enhanced by Glutamate: (1) Induction of T-cell adhesion to fibronectin and laminin [6]; (2) Induction of chemotactic migration of normal naı̈ve peripheral T-cells towards SDF-1 [6]; (3) Induction of calcium signals and c-jun and c-fos gene expression, via group I metabotropic glutamate receptors [38]; (4) Positive modulation Kv1.3 channel gating, causing currents to activate faster and at significantly more hyperpolarized potentials, hence rendering the T lymphocyte readily responsive to immune stimuli [37]; (5) Enhancement of T lymphocyte proliferation to MBP and MOG and the chemotactic migration of T-cells in MS patients and control individuals. Higher GluR3 expression and higher activating effect of glutamate on T-cells of MS patients during relapses were reported [33]. Abnormal expression or function of Glutamate receptors in T-cells in human diseases: Multiple sclerosis [33]; ALS [36] Serotonin Serotonin effects in the brain: Regulation of emotion, anxiety, agitation, and gastrointestinal function Serotonin receptors expressed in the brain: Serotonergic 5-HT1A, 5-HT1B, 5-HT1D, 5-HT1E, 5-HT1F, 5-HT2A, 5-HT2B, 5-HT2C, 5-HT3, 5-HT4, 5-HT5, 5-HT6, 5-HT7 Serotonin receptors expressed in various T-cells: Serotonergic 5HT1, 5HT1a, 5-HT(1B), 5-HT(2A), 5-HT3, 5-HT3A, 5-HT7 [39,44,45] Among the human T-cell functions activated/enhanced by Serotonin: (1) Induction of Na+ influx [46]; (2) Induction of IL-16 secretion from CD8+ (not CD4+) T-cells [40]; (3) Enhancement of proliferation and IL-2 production in response to Con A [39]; (4) Induction of ERK1/2 phosphorylation in naı̈ve T-cells via 5-HT(7) [45]; (5) Potentiatation of T-cell activation, via elevated [Na(+)](i) and activation of PKC-dependent PLD pathway [47]; (6) Increased proliferation and mRNA for IL-2 and IFN-g in PHAstimulated in lymphocytes from HIV-seropositive subjects [48]; (7) Injection of a serotonin receptor agonist to HIV-seropositive subjects increased: CD4 T-cells, CD4/CD8 ratio, T-cell proliferation to mitogen and expression of IL-2R (Hofmann et al., 1996) Abnormal expression or function of Serotonin receptors in T-cells in human diseases: HIV [48] Neurotransmitters fall into one of three chemical categories: (1) Amino acids: among them Glutamate, Glycine, and g-aminobutyric acid (GABA). (2) Biogenic amines: among them Dopamine, Norepinephrine, Epinephrine and Serotonin. (3) Peptidergic neurotransmitters termed neuropeptides: among them Somatostatin, Substance P, Neuropeptide Y, Opioids, Gonadotropin releasing hormone (GnRH): GnRH-I and GnRH-II, Calcitonin generelated peptide (CGRP), Thyrotropin releasinghormone (TRH), Corticotropin releasing hormone (CRH), Vasoactive intestinal polypeptide (VIP), Neurotensin, Bombasin, Prolactin, Galanin, Motilin, and many others. The peptidergic neurotransmitters are well known to exert physiological effects at www.sciencedirect.com substantial distances from their sites of release, with clear implication for the functional interactions between nerve fibers and immune target cells. Neurotransmitters have a very wide spectrum of activities via which they affect a kaleidoscope of body functions, some shown in Tables 1 and 2. Many neurotransmitters and/or their analogues have medicinal properties, serve as drugs for various diseases, and are subject of extensive pharmacological studies. Where can T-cells ‘meet’ neurotransmitters? T-cells may be exposed to neurotransmitters in the: (a) Brain — since activated T-cells, and to a lesser extent naı̈ve/resting T-cells, regularly transmigrate into the Current Opinion in Pharmacology 2008, 8:460–471 462 Immunomodulation Table 2 Four examples of neuropeptides (peptidergic neurotransmitters) that can directly activate naı̈ve/resting human T-cells: Their primary function and receptors in the brain, receptors in T-cells, and some of their activating effects on T-cells GnRH-I and GnRH-II GnRH-I and GnRH-II effects in the brain: GnRH-I: Stimulates pituitary synthesis of LH and FSH. The chief hormone orchestrating reproductive events; GnRH-II: Multiple, under investigation GnRH receptors expressed in the brain: GnRH-I R; GnRH-II R identified thus far only in non-human primates. The human GnRH-II R gene is disrupted GnRH receptors expressed in various T-cells: GnRH-I R and a postulated GnRH-II R which is different than GnRH-I R (i.e. GnRH-II induced effects are not blocked by GnRH-I R antagonists) [5] Among the T cell functions activated/enhanced by GnRH-I and GnRH-II: (1) Increase in IL-2 receptor-positive cells and in the basal proliferative activity of splenocytes and thymocytes (Batticane et al., 1991); (2) Injection of GnRH-I agonist increases CD8+ T-cell levels and proliferation to a variety of mitogens [49]; (3) Induction by GnRH-I and GnRH-II of de novo T cell gene expression and of cell surface expression of 67-kDa laminin receptor [5]; (4) Induction by GnRH-I and GnRH-II of T-cell adhesion to laminin [5]; (5) Induction by GnRH-I and GnRH-II of T-cell chemotactic migration towards SDF-1 [5], (6) Augmentation of T-cell homing in vivo into the spleen and bone marrow [5], (7) Increase in IFNg production and in response to IFNg; decrease in IL-4 production (Dixit et al., 2003); (8) Increase in vivo of: CD3+CD69+, CD3+CD25+, and CD3+DR+ lymphocyte subpopulations (decrease CD4+ and CD25+ T-cells) (Ho et al., 1995) Substance P Substance P effects in the brain: In CNS: regulation of mood disorders, anxiety, stress, reinforcement, neurogenesis, respiratory rhythm, neurotoxicity, nausea/emesis and pain Substance P receptors expressed in the brain: NK1, NK2, NK3 Substance P receptors expressed in various T-cells: NK1 receptor ([50] & McCormack, 1996) Some of the T cell functions activated/enhanced by Substance P: (1) Stimulation of human T-cell proliferation ([50] and Payan et al., 1984); (2) Stimulation of IL-2 production, via the NK1 receptor; (3) Induction of atypical secretion of IL-2 and IFN-g by Th2 antigen-specific T cell lines and clones [1,3]; (4) Increase of proliferation, IL-2 production and CD4+ CD25+ and CD4+ RT1B MHC class II molecule via the NK1 receptor (Santoni et al., 2002); (5) In vivo: stimulation of efferent lymph flow and the output into efferent lymph of both small recirculating and blast lymphocytes; Increase and prolongation of in vivo CD4 T-cell output from lymph nodes, associated with a depressant effect on the output of CD8 T-cells (and B cells) (Moore et al., 1990); (6) Enhancement of T cell adhesiveness to endothelial cells, via enhancement of LFA-1/ICAM-1 interactions and induction of T-cell chemotaxis (Vishwanath et al., 1996); (7) Increase in T-cell proliferation by an autocrine effect of endogenous substance P produced by T-cells; the effect is mediated by NK1 receptors (Lambrecht et al., 1999); (8) Induction of T-cell chemotaxis, via the NK1 receptor (Hood et al., 2000); (9) Induction of proliferation, CD25 expression and IL-2 production, and rescue of apoptosis (Santoni et al., 2002) Somatostatin Somatostatin effects in the brain: Regulates the endocrine system and affects neurotransmission and prolifeartion by inhibiting the release of numerous secondary hormones Somatostatin receptors expressed in the brain: SSTR1, SSTR2, SSTR3, SSTR4, SSTR5 Somatostatin receptors expressed in various T-cells: Primarily SSTR2 and SSTR3, SSTR1, SSTR4. SSTR5 expression was reported selectively in activated T-cells (Talme et al., 2001; SSTR2, Elliott et al., 1999, Solomou et al., 2002) Some of the T-cell functions activated/enhanced by Somatostatin: (1) Induction of integrin-mediated adhesion to fibronectin, [4] and to a certain extent also to collagen type IV and laminin, via SSTR2 and SSTR3 (Talme et al., 2001); (2) Induction of typical and atypical secretion of IL-2, IFN-g, IL-4 and IL-10 by Th0, Th1 and Th2 antigen-specific T cell lines and clones [10]; (4) Induction of IL-2 secretion and proliferation [23,89] For other effects of somatostatin on T-cells read: Ferone et al. (2004), Krantic et al. (2000), ten Bokum et al. (2000) CNS across the blood brain barrier, under physiological and pathological conditions. (b) Lymphoid organs — as all primary and secondary lymphoid organs, among them the thymus, spleen, lymph nodes, bone marrow and gut, are massively innervated by nerves which release a variety of neurotransmitters and neuropeptides [8,9]. Furthermore, within these lymphoid organs, there are direct contacts between nerve terminals containing neurotransmitters, and individual immune cells, among them T-cells and B-cells and mast-cells [8,9]. (c) Blood — since both fenestrated and non-fenestrated blood capillaries are intensely innervated by nervesecreting neurotransmitters, thus providing conditions for direct contacts between neurotransmitters and blood-borne T-cells in health and disease. Current Opinion in Pharmacology 2008, 8:460–471 (d) All the other innervated body organs — since all these contain neurotransmitters as well as T-cells that pass through for routine immune surveillance. Collectively, all the above indicate that various neurotransmitters may encounter and affect T-cells in everyday life, in almost every site of the body, and in almost every context of health and disease. T-cells produce endogenous neurotransmitters and can be affected by them in an autocrine/paracrine manner Numerous interesting and solid studies show that T-cells (and other immune cells) can in fact produce and secrete various endogenous neurotransmitters, either spontaneously or after induction by external stimuli. Some of the neurotransmitters produced by T-cells are: Dopamine, www.sciencedirect.com Neurotransmitters activate T-cells Levite 463 Figure 1 Schematic representation showing the various features and functions of normal resting peripheral human T-cells that are activated or modulated by dopamine itself, or by selective dopamine-receptor agonists. Epinephrine, Norepinephrine, Acetylcholine, Serotonin, Somatostatin, VIP, CGRP, GnRH-I, GnRH-II, and others. T-cells may also be affected by some of their endogenously produced and exogenously secreted neurotransmitters in an autocrine and paracrine manner (e.g. [10]), yet only if the concentration of the respective neurotransmitter is appropriate. Finally, I speculate that T-cells may use their own neurotransmitters not only to ‘talk’ to themsleves, but also to ‘talk’ to other cells, mainly to neurons and glia cells, when they enter the brain and ‘need’ to communicate and cooperate with these CNS-resident cells, for example, during viral infection within the CNS. T-cells express specific receptors for various neurotransmitters, and these are dynamically regulated by TCR-activation, cytokines, the neurotransmitters themselves, and other factors Neurotransmitters exert all either excitatory or inhibitory effects on their targets by binding to their cognate receptors expressed in target cells within the nervous system. Each neurotransmitter has a broad family of receptors. The families of neurotransmitter receptors expressed in the nervous system for some of the relevant neurotransmitters and neuropeptides discussed herein, are shown in Tables 1 and 2, respectively. These tables also show the main neurotransmitter receptors expressed www.sciencedirect.com in T-cells, focusing primarily on published evidence for: first, the existence of these receptors at the protein level (not only mRNA, which may or may not be translated) and second, the functional response of these neurotransmitter receptors to the natural neurotransmitter itself (not only to synthetic and somewhat artificial neurotransmitter agonists). Interestingly, the expression of the neurotransmitter receptors in T-cells seems to be very dynamic, and can change dramatically in response to different molecules and processes among them: (a) T-cell receptor (TCR) activation. TCR-activation, that is induced naturally and specifically by viral/ bacterial/parasite/cancer antigens, and can be mimicked artificially by mitogens (e.g. phorbol esters) and anti-CD3 and anti-CD28 antibodies, may dramatically affect the expression of a given neurotransmitter receptor on the T-cell membrane. For example, we recently described a striking example: the glutamate receptor of the AMPA GluR3 subtype (GluR3) is highly expressed in peripheral naı̈ve/resting human T-cells (60–90% GluR3 positive) of all healthy individuals tested, yet eliminated completely from the T-cell surface upon TCR-activation [11] (Figure 2). Going deeper into the mechanism, we revealed that it is granzyme B, the key proteolytic enzyme which is routinely released from TCR-activated T-cells, that cleaves GluR3 from Current Opinion in Pharmacology 2008, 8:460–471 464 Immunomodulation Figure 2 Glutamate receptor of the AMPA subtype 3, GluR3, is highly expressed in resting human T-cells, but not in TCR-activated cells, as the latter release the proteolytic enzyme granzyme B which cleaves GluR3 from their surface [6]. (a–c) Evidences for the presence in T-cells of high levels of GluR3, which is identical in sequence to the brain’s GluR3. (a) GluR3 RT-PCR in normal naı̈ve human peripheral T-cells, human T leukemia line and human T helper clone, and in total brain as positive control [6]. The GluR3 RT-PCR amplification products in T-cells are of the expected molecular weight for each set of primers respectively (E4-E9 632 bp and E3-E6 516 bp) [6]; (b) Double immunofluoresence staining and flow cytometry of naı̈ve normal human T-cells for GluR3 (FITC) and TCR (PE), showing 74% GluR3+ TCR+ double positive cells [6]. (c) GluR3-specific immunostaining staining and confocal microscopy of naı̈ve normal human T-cells (Levite et al., paper in preparation). (d–e) Once T-cells become activated via their T-cell receptor (TCR) by viral/bacterial/parasite/cancer antigens, they characteristically release Granzyme B, a very potent and important proteolytic enzyme. Granzyme B cleaves GluR3 from the T-cell surface, resulting in the complete elimination of this glutamate receptor from the T-cell membrane for some 48 h. After this lag period, GluR3 expression is restored [6]. Cleaved GluR3 portions, containing the immunogenic GluR3B peptide are released to the extracellular milieu. We suggest that this event, if chronic, drives the production of pathogenic GluR3B autoantibodies found in epilepsy patients (see the discussion in [6], the Refs cited therein, and our papers on glutamate receptor autoantibodies and ‘Autoimmune Epilepsy’) [51]. such activated cells, leading to its disappearance from the cell surface for 48 h [11] (Figure 2). (b) Cytokines. Certain cytokines, alike IL-2, can change the expression of neurotransmitter receptors in Tcells. (c) The neurotransmitter itself. Alike in neurons, a neurotransmitter can regulate (usually downregulate) the expression of its own receptors in T-cells. activate many T-cell functions in a powerful and rapid manner. Table 1: for dopamine, glutamate, and serotonin and Table 2: for the neuropeptides GnRH-I, GnRH-II, Substance P and Somatostatin (other relevant and important neuropeptides, including NPY and CGRP [3,4], are unfortunately not covered in this review because of space limitation) present examples of neurotransmitters that by themselves activate T-cell function. Herein, only two of these neurotransmitters will be further discussed: dopamine and glutamate. Many neurotransmitters can trigger T cell function Dopamine The data accumulated thus far show that various neurotransmitters bind to their receptors in T-cells and can Dopamine (Table 1) is one of the principal neurotransmitters in the central nervous system involved in several Current Opinion in Pharmacology 2008, 8:460–471 www.sciencedirect.com Neurotransmitters activate T-cells Levite 465 Figure 3 Schematic representation showing the various features and functions of normal resting peripheral human T-cells that are activated or modulated either by glutamate itself, or by selective glutamate/AMPA receptor agonists. key functions such as behavior, control of movement, endocrine regulation, and cardiovascular function. The secondary lymphoid tissues are highly innervated by sympathetic nerve fibers that store dopamine at high contents, and lymphocytes also produce dopamine [12,13,14]. Dopamine signals via five different seventransmembrane G-protein-coupled receptors termed D1– D5 dopamine receptors, some of which (particularly of the D2 subclass) represent the primary therapeutic target in a number of neuropathological disorders, including schizophrenia, Parkinson’s disease, and are expressed in Huntington Chorea. Dopamine triggers T-cell function via its dopamine receptors Dopamine-receptors D2, D3, D4 and D5 are expressed in T-cells ([7,10,15,16,21], see also Table 1). Furthermore, these dopaminergic receptors are genuinely functional, because various T-cell functions are affected upon binding of dopamine or dopaminergic agonists to T-cells. The T-cell features and functions activated by dopamine or by highly selective dopamine D2 and D3 receptor agonsists appear in Table 1 and are shown schematically in Figure 1. For example, we reveled that dopamine on its own can activate human normal naı̈ve peripheral T-cells and trigger their adhesion to fibronectin [10], a major glycoprotein of the extracellular matrix (ECM), via activation of 4b1 a5b1 integrin moieties. Such T-cell adhesion is critical for trafficking and extravasation of T-cells across blood vessels and tissue barriers [10]. Using seven dopaminergic agonists and antagonists highly selective for the different dopamine subtypes, www.sciencedirect.com we further found that the dopamine-induced T-cell adhesion was mediated via the D3R and D2R [10]. Testing dopamine in a broad concentration range of 10 16 to 10 4 M, we found that 10 nM was within the optimal range for activating T-cells [10]. In a subsequent confirming study, Watanabe et al. [21] found that the D3R was the predominant subtype of dopamine-receptors in the secondary lymphoid tissues and selectively expressed by naı̈ve CD8+ T-cells from both humans and mice. Dopamine selectively induced the chemotactic migration of naı̈ve CD8+ T-cells, and was highly synergistic with CCL19, CCL21, and CXCL12. Dopamine also selectively induced adhesion of naı̈ve CD8+ T-cells to fibronectin and ICAM-1 by the activation of integrins. Intraperitoneal injection of mice with dopamine selectively attracted naı̈ve CD8+ T-cells into the peritoneal cavity. Treatment of mice with a D3 antagonist reduced homing of naı̈ve CD8+ T-cells into lymph nodes [21]. Dopamine can also induce T-cell cytokine secretion. Indeed, we found that dopamine on its own induced a significant increase in TNFa and IL-10 secretion by naı̈ve resting normal-human T-cells, and induced 5fold elevation of the corresponding TNFa and IL-10 mRNA levels (without affecting IFNg and IL-4) [7]. Interestingly, dopamine-induced TNFa upregulation was evident 24 hours after dopamine stimulation, and was mediated primarily by D3R, while IL-10 upregulation was evident after 72 hours, and was mediated primCurrent Opinion in Pharmacology 2008, 8:460–471 466 Immunomodulation Figure 4 It’s a matter of context: The context determines the final effect of a given neurotransmitter on a given T-cell function. The schemes in A-D show the most important factors that determine whether a specific neurotransmitter would activate or suppress a given T-cell function: (a) The activation state of the T-cells: this has a major impact on the specific neurotransmitter receptors expressed on the cell surface of T-cells, and on the response of these Tcells to the neurotransmitter. Naı̈ve/resting resting T-cells are often activated by a given neurotransmitter, while TCR-activated or cytokine-activated Tcells are often suppressed by the very same neurotransmitter. (b) The specific neurotransmitter receptors expressed on the T cells. Each neurotransmitter has a broad family of cognate receptors, which all bind the native neurotransmitter, but respond somewhat differently, due to their different characteristics. (c) The neurotransmitter dose: many neurotransmitters affect T-cell function at an optimal low range of 10 10 to 10 8 M. Higher concentration may be nonproductive, suppressive or even toxic [6,33,37,39]. (d) The T-cell subtype: Different T-cells subpopulation can respond differently to the same neurotransmitter. CD4+ react differently than CD8+ T-cells [40], and so do Th1 and Th2 T-cells [14,41], and Teff and Treg cells [13]. (e) Other neurotransmitters released concomitantly from the same nerve endings or others. T-cells exposed to one neurotransmitter or neuropeptide would respond differently than T-cells exposed simultaneously to more than one neurotransmitter or neuropeptide released from the same neuron. Examples of neuroactive peptides coexisting with other neurotransmitters in the same neurons are: (1) Dopamine and Cholecystokinin or Neurotensin; (2) Serotonin and Substance P or TRH or Enkephalin; (3) Norepinephrine (noradrenaline) with Galanin, Enkephalin, or Neuropeptide Y; (4) Epinephrine (adrenaline) with Neuropeptide Y or Neurotensin; (5) GABA with Somatostatin or Cholecystokinin or Neuropeptide Y; (6) Acetylcholine with VIP or Substance P. In addition to the above, some neurons make several different neuropeptides. For instance, Vasopressin coexists with dynorphin and galanin or with CRF. Oxytocin co-exists with enkephalin, dynorphin and cholecystokinin. (f) The cytokine milieu. The specific cytokines present around the T-cells once a neurotransmitter is released in their vicinity, can markedly affect the final effect of this neurotransmitter on these cells. arily by D2R. This study showed that dopamine has an unique ability to trigger a selective secretion of either TNFa only (via D3R), or IL-10 only (via D2R) or both (via D1/D5R) [7]. This dopamine-induced effect sharply contrasts with ‘classical’ TCR-activation, that leads to a robust yet nonselective secretion of all the T-cell cytokines. As such, dopamine-induced T-cell cytokine secretion may have important implications in fighting pathologies that are either mediated or can be cured by IL-10 or TNFa. Dopamine can probably also activate T-cell function indirectly, by suppressing T-regulatory cells (Treg), as suggested recently [13,22]. Here, the endogenous catecholamines act by autocrine/paracrine loop, via dopaminergic receptors and pathways, to downregulate Treg function [13]. The effect is mediated primarily by D1 receptors [13]. Current Opinion in Pharmacology 2008, 8:460–471 Taken together, all the above mentioned effects, and those described in Table 1 and Figure 1, show that dopamine by itself can bind to naı̈ve/resting peripheral T-cells, and induce T-cell adhesion, chemotactic migration, attraction and homing into specific organs, cytokine secretion, and additional T-cell functions. All these suggest that dopamine is very important not only for its well-known ‘classsical’ effects (see Table 1), but also for delivering signals from the brain to T-cells, needed for effective, proper, regulated, and orchestrated immune responses. Having said that, and focused herein only on the activating effects on dopamine on T-cell function, it should nevertheless be mentioned that dopamine can also suppress some T-cell functions and features, primarily proliferation and cytotoxicity, mainly when it interacts with activated T-cells (rather than with naı̈ve/resting T-cells). www.sciencedirect.com Neurotransmitters activate T-cells Levite 467 Relevance of the dopamine-receptors in T-cell to human diseases Abnormal expression of dopamine-receptors in lymphocytes/T-cells, or abnormal response of dopaminergic receptors in lymphocytes/T-cells, was reported in Schizophrenia [23–25], Parkinson’s disease, [26,27], Alzheimer’s disease [17], Migraine [28], HIV [29,30], and Multiple Sclerosis [31]. Unfortunately, some of these studies studied only the presence of abnormal receptor mRNA levels rather than the functional receptor itself. Thus, further studies are needed before the pathological and pharmacological significance of these potentially exciting findings can be fully evaluated. Glutamate Glutamate (Table 1) is the brain’s primary excitatory neurotransmitter, involved in affective, sensory, and motor function, as well as in learning, memory, cognition, and synaptic plasticity. Glutamate signals though two broad families of glutamate receptors, consisting of the ionotropic (ion channels) glutamate-receptor, and the G-protein-coupled metabotropic glutamate-receptors. The ionotropic glutamate-receptors are subdivided into AMPA, Kainate, and NMDA glutamate-receptors, and in each, there is yet some further subdivision to individual receptors having different numbers. The metabotropic glutamate receptors are also subdivided into mGluR1 to mGluR7. Glutamate triggers T-cell function via its glutamate-receptors Human T-cells express several types of glutamate-receptors, and glutamate has various effects on T cell function [32,6,11,33,34–38]. Table 1 and Figure 3 list and cite some of the glutamate-induced T-cell functions and features. In a recent study we described for the first time, that normal human T-cells, human T-leukemia line, and the mouse anti-myelin basic protein (MBP) 87–99 T-cells (which induce experimental autoimmune encephalomyelitis (EAE), the animal model for multiple sclerosis (MS)), express very high levels of glutamate receptor GluR3 [6]. The multiple methodologies used for showing GluR3 expression in T-cells (Figure 2a–c) include: GluR3-specific RT-PCR and sequencing, establishing identity between the T-cell GluR3 and the authentic brain GluR3, Western blot, and GluR3 cell-surface expression, as revealed by immunofluorescence-staining, flow-cytometry, and confocal microscopy [6]. Furthermore, glutamate in the absence of any additional molecule, induced integrin-dependent adhesion to laminin and fibronectin, and chemotactic migration toward the chemokine SDF-1 [6] (Figure 2d,e). The effects of glutamate were mimicked by AMPA (glutamate/AMPA receptor-agonist) and blocked by CNQX and NBQX (glutamate/AMPA receptor-antagonists). www.sciencedirect.com Testing glutamate in a very broad concentration range, we found that glutamate-induced T-cell activation was evident in an optimal conc. of 10 nM, which is exactly the concentrations of glutamate within the brain extracellular fluid. Taken together, the high expression of GluR3 in T-cells, and the ability of glutamate to activate T-cell functions in its physiological concentration within the brain, could be of importance in many physiological and pathological situations, among them: first, T-cell transmigration into the CNS across laminin-containing capillary endothelial cells that form the blood–brainbarrier and second, T-cell mediated autoimmune diseases, especially MS [6]. Surprisingly, in a subsequent study [11], we further found that the glutamate receptor GluR3 is completely eliminated from the cell surface of the TCR-activated cells, and that this is because of proteolytic cleavage of GluR3 by granzyme B released by the TCR-activated cells. This is shown schematically in Figure 2. In parallel to losing intact GluR3, TCR-activated cells also lose glutamate-induced adhesion to laminin [6]. Thus, glutamate, via GluR3, may activate only resting, but not TCR-activated cells [6]. Gallart et al. have recently shown that human dendritic cells undergoing maturation and in contact with T-cells, release significant amounts of glutamate, and that after productive antigen presentation, the metabotropic glutamate-receptor 1 is expressed in T-cells and mediates an enhanced T-cell proliferation, and secretion of Th1 and proinflammatory cytokines [34]. The stimulation of group I metabotropic glutamatereceptors also evokes calcium signals and c-jun and c-fos gene expression in human T-cells, thus activating multiple downstream signaling regulating important T-cell functions [38]. Glutamate, at concentrations within its normal plasma levels, and via metabotropic glutamate receptors also positively modulates the channel gating of Kv1.3 [37], a key voltage-gated potassium ion channel in T-cells [2], causing a faster current activation at significantly more hyperpolarized potentials, hence rendering the T-cells readily responsive to immune stimuli [37]. These and other glutamate-induced T-cell activating effects are mentioned in Table 1 and Figure 3. Relevance of glutamate-receptors in T-cell to human diseases Multiple sclerosis Sarchielli et al. [33] showed recently that T-cells of control subjects and MS patients express both the mRNA and the GluR3 receptor protein, in line with Current Opinion in Pharmacology 2008, 8:460–471 468 Immunomodulation GluR3 expression shown previously in murine antiMBP 87–99 T-cell line [37]. Excitingly, an upregulation of the GluR3 expression during relapse, and in patients with neuroradiological evidence of disease activity, was revealed [33]. Furthermore, glutamate and AMPA, at concentrations of 10 nM to 10 mM enhanced T-cell proliferation to MBP and MOG, and the chemotactic migration of T-cells of both controls and MS patients. In the latter group, significantly higher proliferation values in response to glutamate were found in patients assessed during relapse and in those with gadolinium (Gd)+ enhancing lesions on MRI. Together, MS patients during relapses with evidence of disease activity on MRI, had higher GluR3 expression in their T-cells and glutamate affected these cells to a greater extent [33]. These interesting findings are in perfect agreement with the original suggestions raised when GluR3 was first detected in encephalitogenic anti-MBP T-cells [6], and support the idea that glutamate-induced activation of MSassociated T-cells may indeed play a vital role in this disease. This topic surely calls for further investigation. Autoimmune epilepsy We recently suggested that the cleavage of glutamate receptor GluR3 from the T-cell surface by granzyme B, upon TCR-activation, and the release of immunogenic GluR3B peptide to the extracellular milieu (especially if occurring in a continuous manner, for example in a chronic infection), could be the first step leading to the production of neuropathogenic GluR3B autoantibodies, found in some epilepsy patients (see the Discussion in [6], the relevant Refs cited therein, and our papers on ‘Autoimmune Epilepsy’) [51]. It is a matter of context: crucial factors can determine whether a given neurotransmitter would activate or rather suppress a given T-cell function An important take-home message from the study on the effects of neurotransmitters on T-cells, should be that a given neurotransmitter is rarely exclusively stimulatory or inhibitory, when it comes to its effects on T-cells. I would argue that the findings thus far show that often the very same neurotransmitter can be both activating and suppressing! It all depends on the absolutely crucial factors that determine the functional outcome, shown schematically in Figure 4a–f. These include: (a) The activation state of the T-cells. Naı̈ve/resting T-cells are often activated by a given neurotransmitter, while TCR-activated or cytokine-activated T-cells are often suppressed by the very same neurotransmitter. (b) The subtype of neurotransmitter receptors expressed on the target T-cells. Each neurotransmitter has a broad family of receptors, which all bind the parent neurotransmitter, but respond somewhat differently, because of some different characteristics and signaling pathways. Naı̈ve/resting T-cells often express a different composition of neurotransmitter receptors than activated T-cells [6,33,37,39]. (c) The neurotransmitter dose. Many neurotransmitters affect T-cell function at an optimal low dose range of 10 10 to 10 8 M. Higher concentration may be either nonproductive, suppressive or even toxic [6,33,37,39]. (d) The T-cell subpopulation being stimulated. CD4+ and CD8+ T-cells may respond differently to neurotransmitters [40], and so do Th1 and Th2 cells [14,41] and regulatory and effector T-cells [13]. Are the interactions of T-cells with neurotransmitters beneficial or detrimental, first for the cells themselves and second for the overall health of the body? Indeed, different T-cell subpopulations often express different receptor subtypes for the same natural neurotransmitter. I would provocatively argue that the answer to these questions is NOT dictated by the neurotransmitter itself (which has ‘fixed’/conserved identity), but rather by the target T-cells and the context, see Figure 4. Thus, if the T-cells are normal and healthy, their activation by a given neurotransmitter will most probably be beneficial both for the T-cells themselves and for the entire body, as it will improve the beneficial performance of these ‘good’ T-cells. By contrast, if the T-cells are detrimental, alike cancer T-cells, that is, T-leukemia and T-lymphoma, or autoimmune T-cells, alike in MS and other T-cell-mediated autoimmune diseases, their activation by a neurotransmitter will still be beneficial for these detrimental T-cells, but this time bad for the entire body, since it would aggravate the T-cell-mediated pathogenicity. (e) The cytokine, chemokine, and growth factors milieu. These may change dramatically the effect of a given neurotransmitter on a given T-cell population, as shown by published and yet unpublished data. (f) Other neurotransmitters released concomitantly. Nerve endings often contain both a conventional neurotransmitter (such as glutamate, GABA, or dopamine) and one or more neuropeptides, as shown schematically in Figure 4e. There are many such couples of neuroactive peptides coexisting with other neurotransmitters, and specific examples are listed in the legend for Figure 4e. The neuropeptides are generally packaged in large dense-core vesicles, and the coexisting neurotransmitters in small synaptic vesicles. The location within the neuron and the Current Opinion in Pharmacology 2008, 8:460–471 www.sciencedirect.com Neurotransmitters activate T-cells Levite 469 release of the large and small vesicles are different. Clearly, one may envision different contexts and different outcomes: first, T-cells exposed only to one neurotransmitter or one neuropeptide; second, T-cells exposed simultaneously to a given neurotransmitter and a given neuropeptide, or to one after the other. Each of the above parameters can dictate whether a specific neurotransmitter will activate, suppress or rather not affect at all a given T-cell function. Variations in the above parameters that define the context, are most probably the basis for some of the contradictory results reported in the literature, for example where the term ‘inhibitory neuropeptide’ was assigned to a given neuropeptide that, at physiological concentrations, can in fact activate T-cell function in a direct and profound mode. natural neurotransmitters activate T-cells and improve their function in vitro and in vivo, also opens up novel and safe ways by which the pharmacological world could take advantage of it to fight some human diseases, primarily cancer and infectious diseases. Indeed, an especially attractive therapeutic avenue is to activate T-cells by natural neurotransmitters ex vivo, for improved adoptive T-cells immunotherapy of cancer. We are currently moving forward to test this exciting therapeutic option. Acknowledgements I thank Yonatan Ganor for his contribution to the preparation of the tables. References and recommended reading Papers of particular interest, published within the period of review, have been highlighted as: of special interest of outstanding interest Summary and concluding remarks The large body of evidence outlined in this review indicates that some of the ‘classical’ neurotransmitters, alike dopamine, glutamate and serotonin, and numerous neuropeptides among them Substance P, GnRH-I and II, Neuropeptide Y, CGRP and Somatostatin have the ability to bind to their cognate receptors in T-cells and activate pivotal T-cells functions. Among the T-cell functions and features that are triggered/elevated by neurotransmitters (see Tables 1 and 2 and Figures 1 and 3) are: T-cell adhesion, chemotactic migration, homing into solid organs, cytokine secretion, proliferation, cytotoxicity, ion currents, the levels of intracellular Ca2+, the level of surface expressed receptors, de novo gene expression, mRNA levels of various proteins, signal transduction, and others. The expression of the neurotransmitter receptors in T-cells is by no means constant: it can be changed dramatically by TCR-activation, cytokines, the neurotransmitter itself, other co-released neurotransmitters and additional factors. T-cells also produce and secrete some neurotransmitters and may be affected by them in return, by an autocrine/paracrine mode. Abnormal levels of neurotransmitter receptors in T-cells have been observed in a few human diseases. If these interesting findings would be reproduced and extended in future studies, it could mean that perturbed interactions between neurotransmitters and T-cells, for example due to too high or low level of neurotransmitter receptors in T-cells, or due to mal function of the brain because of chronic stress or injury, play an active role in the pathogenesis of the respective diseases, or in the T-cell’s effort to fight the disease. In conclusion, neurotransmitters may be as important for the immune system as for the nervous system, and as such deserve every effort to learn more how they affect T-cells, where and when. In addition, the direct, rapid, potent, specific, and receptor-mediated manner by which certain www.sciencedirect.com 1. Levite M: Nerve-driven immunity. The direct effects of neurotransmitters on T-cell function. Ann N Y Acad Sci 2000, 917:307-321. This is the first review summarizing and discussing a completely novel concept: neurotransmitters can activate T-cells in a direct and powerful manner and trigger key T-cell functions. Neurotransmitters do so by stimulating their cognate functional receptors expressed in T-cells. 2. Levite M: Nervous immunity: neurotransmitters, extracellular K+ and T-cell function. Trends Immunol 2001, 22:2-5. 3. Levite M: Neuropeptides, by direct interaction with T cells, induce cytokine secretion and break the commitment to a distinct T helper phenotype. Proc Natl Acad Sci U S A 1998, 95:12544-12549. This study reveals a very surprising and unique phenomenon: neuropeptides can on their own trigger cytokine secretion by Th1 and Th2 cells, and even induce a ‘forbidden’ atypical cytokine secretion by already committed Th1 and Th2 cells e.g. IFNg and IL-2 secretion by Th2 clones, and IL-4 secretion by Th1 clones. This unique property of neuropeptides may have wide implications to diseases that are mediated by Th1 cytokines and that can be arrested by a shift to Th2 cytokines, or visa versa. 4. Levite M, Cahalon L, Hershkoviz R, Steinman L, Lider O: Neuropeptides, via specific receptors, regulate T cell adhesion to fibronectin. J Immunol 1998, 160:993-1000. A study showing that key neuropeptides: somatostatin, Neuropeptide Y, and CGRP can directly activate T-cells and induce their adhesion to glycoproteins of the extra cellular matrix. Substance P and some of its fragments have a completely opposite inhibitory effect on T-cell adhesion. The study also shows the neuropeptide receptors mediating the effects of these neuropeptides on T-cells. 5. Chen A, Ganor Y, Rahimipour S, Ben-Aroya N, Koch Y, Levite M: The neuropeptides GnRH-II and GnRH-I are produced by human T cells and trigger laminin receptor gene expression, adhesion, chemotaxis and homing to specific organs. Nat Med 2002, 8:1421-1426. This study shows that the neuropeptides GnRH-II and GnRH-I can each on its own trigger several human T-cell functions, among them de novo gene expression of a key laminin receptor, adhesion to laminin, chemtactic migation, and homing in vivo into selected organs. The study also shows that T-cells produce the neuropeptides GnRH-I and GnRH-II. 6. Ganor Y, Besser M, Ben-Zakay N, Unger T, Levite M: Human T cells express a functional ionotropic glutamate receptor GluR3, and glutamate by itself triggers integrin-mediated adhesion to laminin and fibronectin and chemotactic migration. J Immunol 2003, 170:4362-4372. This is the first evidence for high glutamate receptor GluR3 cell surface expression in normal and EAE-inducing anti-MBP T-cells, and that glutamate or AMPA agonists, at a low 10 nM concentration, can activate T-cells and induce their adhesion and migration. The relevance of glutamate-induced T-cell activation to multiple sclerosis (and other T-cellmediated diseases) is suggested and discussed. Current Opinion in Pharmacology 2008, 8:460–471 470 Immunomodulation 7. Besser MJ, Ganor Y, Levite M: Dopamine by itself activates either D2, D3 or D1/D5 dopaminergic receptors in normal human T-cells and triggers the selective secretion of either IL10, TNFalpha or both. J Neuroimmunol 2005, 169:161-171. This study shows that dopamine on its own triggers secretion of IL-10 and TNFalpha by normal human T-cells, and that it does so by activating different dopaminergic receptors expressed in these cells. This exclusive dopamine-induced secretion of either the anti-inflammatory IL-10, or the pro-inflammatory TNFalpha, differs markedly from the classical TCRinduced non-selective cytokine secretion and as such may have wide implications. 8. Fink T, Weihe E: Multiple neuropeptides in nerves supplying mammalian lymph nodes: messenger candidates for sensory and autonomic neuroimmunomodulation? Neurosci Lett 1988, 90:39-44. 9. Weihe E, Nohr D, Michel S, Muller S, Zentel HJ, Fink T, Krekel J: Molecular anatomy of the neuro-immune connection. Int J Neurosci 1991, 59:1-23. A very exiting, important and comprehensive study, showing the presence, distribution, and coexistence of various peptides, neuroendocrine markers and enzymes of the catecholamine pathway in nerves supplying many lymphoid tissues in a variety of mammalian species. The possible importance to various diseases is discussed. 10. Levite M, Chowers Y, Ganor Y, Besser M, Hershkovits R, Cahalon L: Dopamine interacts directly with its D3 and D2 receptors on normal human T cells, and activates beta1 integrin function. Eur J Immunol 2001, 31:3504-3512. The study shows that dopamine by itself activates naı̈ve/resting human peripheral T-cells, by stimulating dopaminergic D2 and D3 receptors expressed in these cells. The study also reveals the dose range in which dopamine can activate resting/naı̈ve T-cells. 11. Ganor Y, Teichberg VI, Levite M: TCR activation eliminates glutamate receptor GluR3 from the cell surface of normal human T cells, via an autocrine/paracrine granzyme B-mediated proteolytic cleavage. J Immunol 2007, 178:683-692. The study shows a completely novel observation and mechanism for the regulation of glutamate receptors in T-cells: glutamate receptor GluR3 is highly expressed in naı̈ve/resting T-cells, yet cleaved from the cell surface by autocrine/paracrine granzyme B after TCR-activation. 12. Bergquist J, Tarkowski A, Ekman R, Ewing A: Discovery of endogenous catecholamines in lymphocytes and evidence for catecholamine regulation of lymphocyte function via an autocrine loop. Proc Natl Acad Sci U S A 1994, 91:12912-12916. 13. Cosentino M, Fietta AM, Ferrari M, Rasini E, Bombelli R, Carcano E, Saporiti F, Meloni F, Marino F, Lecchini S: Human CD4+CD25+ regulatory T cells selectively express tyrosine hydroxylase and contain endogenous catecholamines subserving an autocrine/paracrine inhibitory functional loop. Blood 2007, 109:632-642. This is an important and elegant study, showing that regulatory T-cells (Tregs) contain substantial amounts of dopamine, norepinephrine, and epinephrine, and that catecholamine release leads to an autocrine/paracrine inhibitory effect of Treg function. The effect is mediated by selective dopamine D1-like receptors in Tregs. 18. Ricci A, Bronzetti E, Felici L, Greco S, Amenta F: Labeling of dopamine D3 and D4 receptor subtypes in human peripheral blood lymphocytes with [3H]7-OH-DPAT: a combined radioligand binding assay and immunochemical study. J Neuroimmunol 1998, 92:191-195. 19. Ricci A, Bronzetti E, Mignini F, Tayebati SK, Zaccheo D, Amenta F: Dopamine D1-like receptor subtypes in human peripheral blood lymphocytes. J Neuroimmunol 1999, 96:234-240. 20. Basu S, Dasgupta PS: Dopamine, a neurotransmitter, influences the immune system. J Neuroimmunol 2000, 102:113-124. 21. Watanabe Y, Nakayama T, Nagakubo D, Hieshima K, Jin Z, Katou F, Hashimoto K, Yoshie O: Dopamine selectively induces migration and homing of naive CD8+ T cells via dopamine receptor D3. J Immunol 2006, 176:848-856. 22. Kipnis J, Cardon M, Avidan H, Lewitus GM, Mordechay S, Rolls A, Shani Y, Schwartz M: Dopamine, through the extracellular signal-regulated kinase pathway, downregulates CD4+CD25+ regulatory T-cell activity: implications for neurodegeneration. J Neurosci 2004, 24:6133-6143. 23. Boneberg EM, von Seydlitz E, Propster K, Watzl H, Rockstroh B, Illges H: D3 dopamine receptor mRNA is elevated in T cells of schizophrenic patients whereas D4 dopamine receptor mRNA is reduced in CD4+ -T cells. J Neuroimmunol 2006, 173:180-187. 24. Ilani T, Ben-Shachar D, Strous RD, Mazor M, Sheinkman A, Kotler M, Fuchs S: A peripheral marker for schizophrenia: Increased levels of D3 dopamine receptor mRNA in blood lymphocytes. Proc Natl Acad Sci U S A 2001, 98:625-628. 25. Kwak YT, Koo MS, Choi CH, Sunwoo I: Change of dopamine receptor mRNA expression in lymphocyte of schizophrenic patients. BMC Med Genet 2001, 2:3. 26. Barbanti P, Fabbrini G, Ricci A, Cerbo R, Bronzetti E, Caronti B, Calderaro C, Felici L, Stocchi F, Meco G et al.: Increased expression of dopamine receptors on lymphocytes in Parkinson’s disease. Mov Disord 1999, 14:764-771. 27. Nagai Y, Ueno S, Saeki Y, Soga F, Hirano M, Yanagihara T: Decrease of the D3 dopamine receptor mRNA expression in lymphocytes from patients with Parkinson’s disease. Neurology 1996, 46:791-795. 28. Barbanti P, Fabbrini G, Ricci A, Pascali MP, Bronzetti E, Amenta F, Lenzi GL, Cerbo R: Migraine patients show an increased density of dopamine D3 and D4 receptors on lymphocytes. Cephalalgia 2000, 20:15-19. 29. Rohr O, Sawaya BE, Lecestre D, Aunis D, Schaeffer E: Dopamine stimulates expression of the human immunodeficiency virus type 1 via NF-kappaB in cells of the immune system. Nucleic Acids Res 1999, 27:3291-3299. 30. Scheller C, Sopper S, Jassoy C, ter Meulen V, Riederer P, Koutsilieri E: Dopamine activates HIV in chronically infected T lymphoblasts. J Neural Transm 2000, 107:1483-1489. 14. Josefsson E, Bergquist J, Ekman R, Tarkowski A: Catecholamines are synthesized by mouse lymphocytes and regulate function of these cells by induction of apoptosis. Immunology 1996, 88:140-146. 31. Giorelli M, Livrea P, Trojano M: Dopamine fails to regulate activation of peripheral blood lymphocytes from multiple sclerosis patients: effects of IFN-beta. J Interferon Cytokine Res 2005, 25:395-406. 15. McKenna F, McLaughlin PJ, Lewis BJ, Sibbring GC, Cummerson JA, Bowen-Jones D, Moots RJ: Dopamine receptor expression on human T- and B-lymphocytes, monocytes, neutrophils, eosinophils and NK cells: a flow cytometric study. J Neuroimmunol 2002, 132:34-40. This is an important study showing the expression of different dopamine receptors in human T-cells, B-cells, monocytes, neutrophils, eosinophils, and NK cells. 32. Lombardi G, Dianzani C, Miglio G, Canonico PL, Fantozzi R: Characterization of ionotropic glutamate receptors in human lymphocytes. Br J Pharmacol 2001, 133:936-944. This is a study showing the human lymphocytes express ionotropic glutamate receptors, functionally operating as modulators of cell activation. 16. Santambrogio L, Lipartiti M, Bruni A, Dal Toso R: Dopamine receptors on human T- and B-lymphocytes. J Neuroimmunol 1993, 45:113-119. 17. Barbanti P, Fabbrini G, Ricci A, Bruno G, Cerbo R, Bronzetti E, Amenta F, Luigi Lenzi G: Reduced density of dopamine D2-like receptors on peripheral blood lymphocytes in Alzheimer’s disease. Mech Ageing Dev 2000, 120:65-75. Current Opinion in Pharmacology 2008, 8:460–471 33. Sarchielli P, Di Filippo M, Candeliere A, Chiasserini D, Mattioni A, Tenaglia S, Bonucci M, Calabresi P: Expression of ionotropic glutamate receptor GLUR3 and effects of glutamate on MBPand MOG-specific lymphocyte activation and chemotactic migration in multiple sclerosis patients. J Neuroimmunol 2007, 188:146-158. A study showing the expression of glutamate receptors AMPA GluR3 in Tcells of healthy individuals and in patients with multiple sclerosis. The study also shows higher GluR3 expression and higher activating effect of glutamate on T cells of MS patients during relapses and with evidence of www.sciencedirect.com Neurotransmitters activate T-cells Levite 471 disease activity on MRI. These observation support the notion that glutamate-activation of autoaggressive T-cells can contribute to the pathology of MS. 34. Pacheco R, Oliva H, Martinez-Navio JM, Climent N, Ciruela F, Gatell JM, Gallart T, Mallol J, Lluis C, Franco R: Glutamate released by dendritic cells as a novel modulator of T cell activation. J Immunol 2006, 177:6695-6704. 35. Pacheco R, Gallart T, Lluis C, Franco R: Role of glutamate on T-cell mediated immunity. J Neuroimmunol 2007, 185:9-19. 36. Poulopoulou C, Davaki P, Koliaraki V, Kolovou D, Markakis I, Vassilopoulos D: Reduced expression of metabotropic glutamate receptor 2mRNA in T cells of ALS patients. Ann Neurol 2005, 58:946-949. 43. Pacheco R, Ciruela F, Casado V, Mallol J, Gallart T, Lluis C, Franco R: Group I metabotropic glutamate receptors mediate a dual role of glutamate in T cell activation. J Biol Chem 2004, 279:33352-33358. 44. Yin J, Albert RH, Tretiakova AP, Jameson BA: 5-HT(1B) receptors play a prominent role in the proliferation of T-lymphocytes. J Neuroimmunol 2006, 181:68-81. 45. Leon-Ponte M, Ahern GP, O’Connell PJ: Serotonin provides an accessory signal to enhance T-cell activation by signaling through the 5-HT7 receptor. Blood 2007, 109:3139-3146. An important study reporting that naı̈ve T cells predominantly express the serotonin receptor 5-HTR, that 5-HTR expression is substantially enhanced on T-cell activation (which leads to the expression of the 5HT(1B) and 5-HT(2A) receptors), and that exogenous 5-HT induces rapid phosphorylation of ERK1/2 and IkappaBalpha in naı̈ve T cells. 37. Poulopoulou C, Markakis I, Davaki P, Nikolaou C, Poulopoulos A, Raptis E, Vassilopoulos D: Modulation of voltage-gated potassium channels in human T lymphocytes by extracellular glutamate. Mol Pharmacol 2005, 67:856-867. 46. Khan NA, Poisson JP: 5-HT3 receptor-channels coupled with Na+ influx in human T cells: role in T cell activation. J Neuroimmunol 1999, 99:53-60. 38. Miglio G, Varsaldi F, Dianzani C, Fantozzi R, Lombardi G: Stimulation of group I metabotropic glutamate receptors evokes calcium signals and c-jun and c-fos gene expression in human T cells. Biochem Pharmacol 2005, 70:189-199. 47. Khan NA, Hichami A: Ionotrophic 5-hydroxytryptamine type 3 receptor activates the protein kinase C-dependent phospholipase D pathway in human T-cells. Biochem J 1999, 344:199-204. 39. Young MR, Kut JL, Coogan MP, Wright MA, Young ME, Matthews J: Stimulation of splenic T-lymphocyte function by endogenous serotonin and by low-dose exogenous serotonin. Immunology 1993, 80:395-400. 48. Eugen-Olsen J, Afzelius P, Andresen L, Iversen J, Kronborg G, Aabech P, Nielsen JO, Hofmann B: Serotonin modulates immune function in T cells from HIV-seropositive subjects. Clin Immunol Immunopathol 1997, 84:115-121. 40. Laberge S, Cruikshank WW, Beer DJ, Center DM: Secretion of IL16 (lymphocyte chemoattractant factor) from serotoninstimulated CD8+ T cells in vitro. J Immunol 1996, 156:310-315. 49. Mann DR, Ansari AA, Akinbami MA, Wallen K, Gould KG, McClure HM: Neonatal treatment with luteinizing hormonereleasing hormone analogs alters peripheral lymphocyte subsets and cellular and humorally mediated immune responses in juvenile and adult male monkeys. J Clin Endocrinol Metab 1994, 78:292-298. 41. Sanders VM, Baker RA, Ramer-Quinn DS, Kasprowicz DJ, Fuchs BA, Street NE: Differential expression of the beta2adrenergic receptor by Th1 and Th2 clones: implications for cytokine production and B cell help. J Immunol 1997, 158:42004210. 42. Barbanti P, Bronzetti E, Ricci A, Cerbo R, Fabbrini G, Buzzi MG, Amenta F, Lenzi GL: Increased density of dopamine D5 receptor in peripheral blood lymphocytes of migraineurs: a marker for migraine? Neurosci Lett 1996, 207:73-76. www.sciencedirect.com 50. Payan DG, Brewster DR, Goetzl EJ: Specific stimulation of human T lymphocytes by substance P. J Immunol 1983, 131:1613-1615. 51. Levite M, Ganor Y: Autoantibodies to glutamate receptors can damage the brain in epilepsy, systemic lupus erythematosus and encephalitis. Expert Rev Neurother 2008, 8:1141-1160. Current Opinion in Pharmacology 2008, 8:460–471