Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Dirofilaria immitis wikipedia , lookup
Typhoid fever wikipedia , lookup
Tuberculosis wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Herpes simplex virus wikipedia , lookup
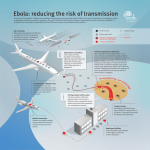
Ebola virus disease wikipedia , lookup
Brucellosis wikipedia , lookup
Orthohantavirus wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Gastroenteritis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Meningococcal disease wikipedia , lookup
Trichinosis wikipedia , lookup
Henipavirus wikipedia , lookup
Chagas disease wikipedia , lookup
Onchocerciasis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
West Nile fever wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neonatal infection wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Hepatitis C wikipedia , lookup
Leptospirosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS CHAPTER 5 Infectious diseases of potential risk for travellers Depending on the travel destination, travellers may be exposed to a number of infectious diseases; exposure depends on the presence of infectious agents in the area to be visited. The risk of becoming infected will vary according to the purpose of the trip and the itinerary within the area, the standards of accommodation, hygiene and sanitation, as well as the behaviour of the traveller. In some instances, disease can be prevented by vaccination, but there are some infectious diseases, including some of the most important and most dangerous, for which no vaccines exist. General precautions can greatly reduce the risk of exposure to infectious agents and should always be taken for visits to any destination where there is a significant risk of exposure. These precautions should be taken regardless of whether any vaccinations or medication have been administered. Modes of transmission and general precautions The modes of transmission for different infectious diseases and the corresponding general precautions are outlined in the following paragraphs. Foodborne and waterborne diseases Foodborne and waterborne diseases are transmitted by consumption of contaminated food and drink. The risk of infection is reduced by taking hygienic precautions with all food, drink and drinking-water consumed when travelling and by avoiding direct contact with polluted recreational waters (see Chapter 3). Examples of diseases acquired by food and water consumption are traveller’s diarrhoea, hepatitis A, typhoid fever and cholera. Vector-borne diseases A number of particularly serious infections are transmitted by insects and other vectors such as mosquitoes and ticks. The risk of infection can be reduced by taking precautions to avoid insect bites and contact with other vectors in places where infection is likely to be present (see Chapter 3). Examples of vector-borne 53 INTERNATIONAL TRAVEL AND HEALTH 2009 diseases are malaria, yellow fever, dengue, Japanese encephalitis, chikungunya and tick-borne encephalitis. Zoonoses (diseases transmitted by animals) Zoonoses include many infections that can be transmitted to humans through animal bites or contact with animals, contaminated body fluids or faeces, or by consumption of foods of animal origin, particularly meat and milk products. The risk of infection can be reduced by avoiding close contact with any animals—including wild, captive and domestic animals—in places where infection is likely to be present. Particular care should be taken to prevent children from approaching or touching animals. Examples of zoonoses are rabies, tularemia, brucellosis, leptospirosis and certain viral haemorrhagic fevers. Sexually transmitted diseases Sexually transmitted diseases are passed from person to person through unsafe sexual practices. The risk of infection can be reduced by avoiding casual and unprotected sexual intercourse, and by use of condoms. Examples of sexually transmitted diseases are hepatitis B, HIV/AIDS and syphilis. Bloodborne diseases Bloodborne diseases are transmitted by direct contact with infected blood or other body fluids. The risk of infection can be reduced by avoiding direct contact with blood and body fluids, by avoiding the use of potentially contaminated needles and syringes for injection or any other medical or cosmetic procedure that penetrates the skin (including acupuncture, piercing and tattooing), and by avoiding transfusion of unsafe blood (see Chapter 8). Examples of bloodborne diseases are hepatitis B and C, HIV/AIDS and malaria. Airborne diseases Airborne transmission occurs when droplet nuclei (evaporated droplets) < 5 micron in size are disseminated in the air. These droplet nuclei can remain suspended in the air for some time. Droplet nuclei are the residuals of droplets and when suspended in the air, they dry and produce particles ranging in size from 1–5 microns. Diseases spread by this mode include open/active pulmonary tuberculosis (TB), measles, chicken pox, pulmonary plague and haemorrhagic fever with pneumonia. 54 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Droplet transmission occurs when there is adequate contact between the mucous membranes of the nose and mouth or conjunctivae of a susceptible person and large particle droplets (> 5 microns). Droplets are usually generated by the infected person during coughing, sneezing, talking or when health care workers undertake procedures such as tracheal suctioning. Diseases transmitted by this route include pneumonias, pertussis, diphtheria, SARS, mumps and meningitis. Diseases transmitted from soil Soil-transmitted diseases include those caused by dormant forms (spores) of infectious agents, which can cause infection by contact with broken skin (minor cuts, scratches, etc). The risk of infection can be reduced by protecting the skin from direct contact with soil in places where soil-transmitted infections are likely to be present. Examples of bacterial diseases transmitted from soil are anthrax and tetanus. Certain intestinal parasitic infections, such as ascariasis and trichuriasis, are transmitted via soil and infection may result from consumption of soil-contaminated vegetables. Fungal infections may be acquired by inhalation of contaminated soil. Specific infectious diseases involving potential health risks for travellers The main infectious diseases to which travellers may be exposed, and precautions for each, are detailed on the following pages. Information on malaria, one of the most important infectious disease threats for travellers, is provided in Chapter 7. The infectious diseases described in this chapter have been selected on the basis of the following criteria: — diseases that have a sufficiently high global or regional prevalence to constitute a significant risk for travellers; — diseases that are severe and life-threatening, even though the risk of exposure may be low for most travellers; — diseases for which the perceived risk may be much greater than the real risk, and which may therefore cause anxiety to travellers; — diseases that involve a public health risk due to transmission of infection to others by the infected traveller. Information about available vaccines and indications for their use by travellers is provided in Chapter 6. Advice concerning the diseases for which vaccination is routinely administered in childhood, i.e. diphtheria, measles, mumps and rubella, pertussis, poliomyelitis and tetanus, and the use of the corresponding vaccines later 55 INTERNATIONAL TRAVEL AND HEALTH 2009 in life and for travel, is also given in Chapter 6. These diseases are not included in this chapter. The most common infectious illness to affect travellers, namely travellers’ diarrhoea, is covered in Chapter 3. Because travellers’ diarrhoea can be caused by many different foodborne and waterborne infectious agents, for which treatment and precautions are essentially the same, the illness is not included with the specific infectious diseases. Some of the diseases included in this chapter, such as brucellosis, HIV/AIDS, leishmaniasis and tuberculosis, have prolonged and variable incubation periods. Clinical manifestations of these diseases may appear long after the return from travel, so that the link with the travel destination where the infection was acquired may not be readily apparent. AVIAN INFLUENZA Cause Highly pathogenic avian influenza A(H5N1) virus, or other non-human influenza subtypes (e.g.H7, H9). Transmission Human infections with highly pathogenic avian influenza A(H5N1) virus occur through bird-to-human, possibly environment-to-human, and very rarely limited, non-sustained human-to-human transmission. Direct contact with infected poultry, or surfaces and objects contaminated by their droppings, is the main route of transmission to humans. Exposure risk is considered highest during slaughter, de-feathering, butchering, and preparation of poultry for cooking. There is no evidence that properly cooked poultry or poultry products can be a source of infection. Nature of disease Patients usually present initially with symptoms of fever and influenza-like illness (malaise, myalgia, cough, sore throat). Diarrhoea and other gastrointestinal symptoms may occur. The disease progresses within days and almost all patients develop clinically apparent pneumonia with radiographic infiltrates of varying patterns. Sputum production is variable and sometimes bloody. Multi-organ failure, sepsis-like syndromes, and uncommonly encephalopathy, occur. The fatality rate among hospitalized patients with confirmed H5N1 infection has been high (about 60%), most commonly as a result of respiratory failure caused by progressive pneumonia and acute respiratory distress syndrome. Geographical distribution Extensive outbreaks in poultry have occurred in parts of Asia, the Middle East, Europe and Africa since 2003, but only sporadic human infections have occurred to date. Continued exposure of humans to avian H5N1 viruses increases the likelihood that the virus will acquire the necessary characteristics for efficient and sustained human-to-human transmission through either gradual genetic mutation or reassortment with a human influenza A virus. Between November 2003 and July 2008, nearly 400 human cases of laboratory-confirmed H5N1 infection were reported to WHO from 15 countries in South-East and central Asia, Europe, Africa and the Middle East. 56 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Risk for travellers H5N1 avian influenza is primarily a disease in birds. The virus does not easily cross the species barrier to infect humans. To date, no traveller has been infected. The risk of infection is increased by prolonged, close and heavy exposure to the virus. Prophylaxis Neuraminidase inhibitors (oseltamivir, zanamivir) are inhibitory for the virus and demonstrate proven efficacy in vitro and in animal studies for prophylaxis and treatment of H5N1 infection. Studies in hospitalized H5N1 patients, although limited, suggest that early oseltamivir treatment with oseltamivir improves survival and given the prolonged virus replication, late intervention with oseltamivir is also justified. Neuraminidase inhibitors are recommended for post-exposure prophylaxis in certain exposed persons. At present WHO does not recommend pre-exposure prophylaxis for travellers but advice may change depending on new findings. Inactivated H5N1 vaccines for human use have been developed and licensed in several countries but are not yet generally available although this situation is expected to change. Some countries are stockpiling these vaccines as a part of pandemic preparedness. Although immunogenic, the effectiveness of these vaccines in preventing the H5N1 infection or reducing disease severity is unknown. Currently, WHO does not have a policy in its use. Precautions Travellers should avoid contact with high-risk environments in affected countries such as live animal markets and poultry farms, any free-ranging or caged poultry, or surfaces that might be contaminated by poultry droppings. Travellers in affected countries should avoid contact with dead migratory birds or wild birds showing signs of disease. Travellers should avoid consumption of undercooked eggs, poultry or poultry products. Hand hygiene with frequent washing or use of alcohol rubs is recommended. If exposure to persons with suspected H5N1 illness or severe, unexplained respiratory illness occurs, travellers should urgently consult health professionals. Travellers should contact their local health providers or national health authorities for supplementary information. ANTHRAX Cause Bacillus anthracis bacteria. Transmission Anthrax is primarily a disease of animals. Cutaneous infection, the most frequent clinical form of anthrax, occurs through contact with products from infected animals (mainly cattle, goats, sheep), such as leather or woollen goods, or through contact with soil containing anthrax spores. Nature of the disease A disease of herbivorous animals that occasionally causes acute infection in humans, usually involving the skin, as a result of contact with contaminated tissues or products from infected animals, or with anthrax spores in soil. Untreated infections may spread to regional lymph nodes and to the bloodstream, and may be fatal. Geographical distribution Sporadic cases occur in animals worldwide; there are occasional outbreaks in central Asia and Africa. Risk for travellers Very low for most travellers. 57 INTERNATIONAL TRAVEL AND HEALTH 2009 Prophylaxis None. (A vaccine is available for people at high risk because of occupational exposure to B. anthracis; it is not commercially available in most countries.) Precautions Avoid direct contact with soil and with products of animal origin, such as souvenirs made from animal skins. BRUCELLOSIS Cause Several species of Brucella bacteria. Transmission Brucellosis is primarily a disease of animals. Infection in people is acquired from cattle (Brucella abortus), dogs (B. canis), pigs (B. suis), or sheep and goats (B. melitensis), usually by direct contact with infected animals or by consumption of unpasteurized (raw) milk or cheese. Nature of the disease A generalized infection with insidious onset, causing continuous or intermittent fever and malaise, which may last for months if not treated adequately. Relapse is not uncommon after treatment. Geographical distribution Worldwide, in animals. It is most common in developing countries, the Mediterranean, Middle East and Central Asia and South America. Risk for travellers Low for most travellers. Those visiting rural and agricultural areas may be at greater risk. There is also a risk in places where unpasteurized milk products are sold near tourist centres. Prophylaxis None. Precautions Avoid consumption of unpasteurized milk and milk products and direct contact with animals, particularly cattle, goats and sheep. CHIKUNGUNYA Cause Chikungunya virus – an Alphavirus (family Togaviridae). Transmission Chikungunya is a viral disease that is spread by mosquitoes. Two important vectors are Aedes aegypti and Aedes albopictus which also transmit dengue virus. These species bite during daylight hours with peak activity in the early morning and late afternoon. Both are found biting outdoors but Ae. aegypti will also readily bite indoors. There is no direct person-to-person transmission. Nature of the disease The name “chikungunya” derives from a Kimakonde word meaning “to become contorted” and describes the stooped appearance of sufferers with joint pain. Chikungunya is an acute febrile illness with sudden onset of fever and joint pains, particularly affecting the hands, wrists, ankles and feet. Most patients recover after a few days but in some cases the joint pains may persist for weeks, months or even longer. Other common signs and symptoms include muscle pain, headache, rash and leukopenia. Occasional cases of gastrointestinal complaints, eye, neurological and heart complications have been reported. Symptoms in infected individuals are often mild and the infection may go unrecognized, or be misdiagnosed in areas where dengue occurs. 58 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Geographical distribution Chikungunya occurs in sub-Saharan Africa, South-East Asia and tropical areas of the Indian subcontinent, as well as islands in the south-western Indian Ocean. Risk for travellers There is a risk for travellers in areas where chikungunya is endemic and in areas affected by ongoing epidemics. Prophylaxis There are no specific anti-viral drugs and no commercial vaccine. Treatment is directed primarily at relieving the symptoms, in particular the joint pain. Precautions Travellers should take precautions to avoid mosquito bites during both day and night (see Chapter 3). CHOLERA Cause Vibrio cholerae bacteria, serogroups O1 and O139. Transmission Infection occurs through ingestion of food or water contaminated directly or indirectly by faeces or vomitus of infected persons. Cholera affects only humans; there is no insect vector or animal reservoir host. Nature of the disease An acute enteric disease varying in severity. Most infections are asymptomatic (i.e. do not cause any illness). In mild cases, diarrhoea occurs without other symptoms. In severe cases, there is sudden onset of profuse watery diarrhoea with nausea and vomiting and rapid development of dehydration. In severe untreated cases, death may occur within a few hours due to dehydration leading to circulatory collapse. Geographical distribution Cholera occurs mainly in poor countries with inadequate sanitation and lack of clean drinking-water and in war-torn countries where the infrastructure may have broken down. Many developing countries are affected, particularly those in Africa and Asia, and to a lesser extent, those in central and South America (see map). Risk for travellers Very low for most travellers, even in countries where cholera epidemics occur. Humanitarian relief workers in disaster areas and refugee camps are at risk. Prophylaxis Cholera vaccines for use by travellers and those in occupational risk groups are available in some countries (see Chapter 6). Precautions As for other diarrhoeal diseases. All precautions should be taken to avoid consumption of potentially contaminated food, drink and drinking-water. Oral rehydration salts should be carried to combat dehydration in case of severe diarrhoea (see Chapter 3). DENGUE Cause The dengue virus – a flavivirus of which there are four serotypes. Transmission Dengue is mostly transmitted by the Aedes aegypti mosquito, which bites during daylight hours. There is no direct person-to-person transmission. Monkeys act as a reservoir host in South-East Asia and West Africa. 59 INTERNATIONAL TRAVEL AND HEALTH 2009 Nature of the disease Dengue occurs in three main clinical forms: ■ Dengue fever is an acute febrile illness with sudden onset of fever, followed by development of generalized symptoms and sometimes a macular skin rash. It is known as “breakbone fever” because of severe muscle, joint and bone pains. Pain behind the eyes (retro-orbital pain) may be present. The fever may be biphasic (i.e. two separate episodes or waves of fever). Most patients recover after a few days. ■ Dengue haemorrhagic fever has an acute onset of fever followed by other symptoms resulting from thrombocytopenia, increased vascular permeability and haemorrhagic manifestations. ■ Dengue shock syndrome supervenes in a small proportion of cases. Severe hypotension develops, requiring urgent medical treatment to correct hypovolaemia. Without appropriate hospital care, 40–50% of cases can be fatal; with timely medical care by experienced physicians and nurses the mortality rate can be decreased to 1% or less. Geographical distribution Dengue is widespread in tropical and subtropical regions of central and South America and South and South-East Asia. Is also occurs in Oceania and Africa (see Map). The risk is lower at altitudes above 1000 metres. Risk for travellers There is a significant risk for travellers in areas where dengue is endemic and in areas affected by epidemics of dengue. Prophylaxis There are no specific vaccines or anti-viral treatments against dengue fever. Use of paracetamol to bring down the fever is indicated. Aspirin, and related non-steroidal anti-inflammatory drugs (NSAIs) such as ibuprofen should be avoided. Precautions Travellers should take precautions to avoid mosquito bites both during the day and evening in areas where dengue occurs. LYMPHATIC FILARIASIS Cause The parasitic disease covered is caused by nematodes of the family Filarioidea. Though this group includes lymphatic filariasis (elephantiasis), onchocerciasis (river blindness), loiaisis (Calabar swelling) or forms of mansonellosis, the term filariasis is usually used to describe lymphatic filariasis caused by W.bancrofti, B.malayi or B.timori. Transmission Lymphatic filariasis is transmitted through the bite of infected mosquitoes, which introduce larval forms of the nematode during a blood meal. Nature of the disease ■ Lymphatic filariasis is a chronic parasitic disease in which adult filaria inhabit the lymphatic vessels, discharging microfilaria into the blood stream. Typical manifestations in symptomatic cases include filarial fever, lymphadenitis and retrograde lymphangitis followed by chronic manifestations such as lymphoedema, hydrocele, chyluria, tropical pulmonary eosinophilic syndrome and in rare instances renal damage. Geographical distribution Lymphatic filariasis occurs throughout sub-Saharan Africa and in much of South-East Asia, in the Pacific islands and in smaller foci in south America. Risk for travellers generally low, unless travel involves extensive exposure to the vectors in endemic areas. 60 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Prophylaxis None. Precautions Avoid exposure to the bites of mosquitoes in endemic areas. GIARDIASIS Cause The protozoan parasite Giardia intestinalis, also known as G. lamblia and G. duodenalis. Transmission Infection usually occurs through ingestion of G. intestinalis cysts in water (including both unfiltered drinking-water and recreational waters) or food contaminated by the faeces of infected humans or animals. Nature of the disease Many infections are asymptomatic. When symptoms occur, they are mainly intestinal, characterized by chronic diarrhoea (watery initially, then loose greasy stools), abdominal cramps, bloating, fatigue and weight loss. Geographical distribution Worldwide. Risk for travellers Significant risk for travellers in contact with recreational waters used by wildlife or with unfiltered water in swimming pools, or contaminated municipal water supplies. Prophylaxis None. Precautions Avoid eating uncooked food (especially raw fruit and vegetables) or ingesting any potentially contaminated (i.e. unfiltered) drinking-water or recreational water. Water can be purified by boiling for at least 5 minutes, alternatively by filtration or chlorination. HAEMOPHILUS MENINGITIS Cause Haemophilus influenzae type b (Hib) bacteria. Transmission Direct contact with infected persons (usually children). Nature of the disease Hib causes meningitis in infants and young children; it may also cause epiglottitis, osteomyelitis, pneumonia, sepsis and septic arthritis. Geographical distribution Worldwide. Hib disease is most common in countries where vaccination against Hib is not practised. It has almost disappeared in countries where routine childhood vaccination is carried out. Risk for travellers A risk for unvaccinated children visiting countries where Hib vaccination is not practised and where infection is therefore likely to be more common. Prophylaxis Vaccination of children (see Chapter 6). Precautions None. HAEMORRHAGIC FEVERS Haemorrhagic fevers are viral infections; important examples are Ebola and Marburg haemorrhagic fevers, Crimean–Congo haemorrhagic fever (CCHF), Rift Valley fever (RVF), Lassa fever, Hantavirus diseases, dengue and yellow fever. Hantavirus diseases, dengue and yellow fever are described separately. 61 INTERNATIONAL TRAVEL AND HEALTH 2009 Cause Viruses belonging to several families. Ebola and Marburg belong to the Filoviridae family; hantaviruses, CCHF and RVF belong to Bunyaviridae family; Lassa fever belongs to Arenaviridae family and dengue and yellow fever belong to the Flaviviridae family. Transmission Viruses that cause haemorrhagic fevers are transmitted by mosquitoes (dengue, yellow fever, RVF), ticks (CCHF), rodents (Hantavirus, Lassa) or bats (Ebola, Marburg). For Ebola or Marburg viruses, humans have been infected from contact with tissues of diseased non-human primates and other mammals, but most human infections have resulted from direct contact with the body fluids or secretions of infected patients. Humans who become infected with CCHF usually become infected from a tick bite, but can also acquire the virus from direct contact with blood or other infected issues from livestock. RVF can be acquired either by mosquito bite or by direct contact with blood or tissues of infected animals (mainly sheep), including consumption of unpasteurized milk. Lassa fever virus is carried by rodents and transmitted by excreta, either as aerosols or by direct contact. Some viral haemorrhagic fevers were amplified in hospitals by nosocomial transmission by unsafe procedures, use of contaminated medical devices (including needles and syringes) and unprotected exposures to contaminated body fluids. Nature of the diseases The haemorrhagic fevers are severe acute viral infections, usually with sudden onset of fever, malaise, headache and myalgia followed by pharyngitis, vomiting, diarrhoea, skin rash and haemorrhagic manifestations. The outcome is fatal in a high proportion of cases (over 50%). Geographical distribution Diseases in this group occur widely in tropical and subtropical regions. Ebola and Marburg haemorrhagic fevers and Lassa fever occur in parts of sub-Saharan Africa. CCHF occurs in the steppe regions of central Asia and in central Europe, as well as in tropical and southern Africa. RVF occurs in Africa and has recently spread to Saudi Arabia. Other viral haemorrhagic fevers occur in central and South America. Risk for travellers Very low for most travellers. However, travellers visiting rural or forest areas may be exposed to infection. Prophylaxis None (except for yellow fever). Precautions Avoid exposure to mosquitoes and ticks and contact with rodents or bats. Avoid unpasteurized milk. HANTAVIRUS DISEASES Hantavirus diseases are viral infections; important examples are haemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS). Cause Hantaviruses, which belong to the family of Bunyaviridae. Transmission Hantaviruses are carried by various species of rodents; specific viruses have particular rodent hosts. Infection occurs through direct contact with the faeces, saliva or urine of infected rodents or by inhalation of the virus in rodent excreta. 62 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Nature of the diseases Acute viral diseases in which the vascular endothelium is damaged, leading to increased vascular permeability, hypotension, haemorrhagic manifestations and shock. Impaired renal function with oliguria is characteristic of HFRS. Respiratory failure caused by acute non-cardiogenic pulmonary oedema occurs in HPS. The outcome is fatal in up to 15% of HFRS cases and up to 50% of HPS cases. Geographical distribution Worldwide, in rodents. Risk for travellers Very low for most travellers. However, travellers may be at risk in any environment where rodents are present in large numbers and contact may occur. Prophylaxis None. Precautions Avoid exposure to rodents and their excreta. Adventure travellers, back-packers, campers and travellers with occupational exposure to rodents in areas endemic for hantaviruses should take precautions to exclude rodents from tents or other accommodation and to protect all food from contamination by rodents. HEPATITIS A Cause Hepatitis A virus, a member of the picornavirus family. Transmission The virus is acquired directly from infected persons by the faecal–oral route or by close contact, or by consumption of contaminated food or drinking-water. There is no insect vector or animal reservoir (although some non-human primates are sometimes infected). Nature of the disease An acute viral hepatitis with abrupt onset of fever, malaise, nausea and abdominal discomfort, followed by the development of jaundice a few days later. Infection in very young children is usually mild or asymptomatic; older children are at risk of symptomatic disease. The disease is more severe in adults, with illness lasting several weeks and recovery taking several months; case-fatality is greater than 2% for those over 40 years of age and 4% for those over 60. Geographical distribution Worldwide, but most common where sanitary conditions are poor and the safety of drinking-water is not well controlled (see Map). Risk for travellers Non-immune travellers to developing countries are at significant risk of infection. The risk is particularly high for travellers exposed to poor conditions of hygiene, sanitation and drinking-water control. Prophylaxis Vaccination (see Chapter 6). Precautions Travellers who are non-immune to hepatitis A (i.e. have never had the disease and have not been vaccinated) should take particular care to avoid potentially contaminated food and water. HEPATITIS B Cause Hepatitis B virus (HBV), belonging to the Hepadnaviridae. 63 INTERNATIONAL TRAVEL AND HEALTH 2009 Transmission Infection is transmitted from person to person by contact with infected body fluids. Sexual contact is an important mode of transmission, but infection is also transmitted by transfusion of contaminated blood or blood products, or by use of contaminated needles or syringes for injections. There is also a potential risk of transmission through other skin-penetrating procedures including acupuncture, piercing and tattooing. Perinatal transmission may occur from mother to baby. There is no insect vector or animal reservoir. Nature of the disease Many HBV infections are asymptomatic or cause mild symptoms, which are often unrecognized in adults. When clinical hepatitis results from infection, it has a gradual onset, with anorexia, abdominal discomfort, nausea, vomiting, arthralgia and rash, followed by the development of jaundice in some cases. In adults, about 1% of cases are fatal. Chronic HBV infection persists in a proportion of adults, some of whom later develop cirrhosis and/or liver cancer. Geographical distribution Worldwide, but with differing levels of endemicity. In north America, Australia, northern and western Europe and New Zealand, prevalence of chronic HBV infection is relatively low (less than 2% of the general population) (see Map). Risk for travellers Negligible for those vaccinated against hepatitis B. Unvaccinated travellers are at risk if they have unprotected sex or use contaminated needles or syringes for injection, acupuncture, piercing or tattooing. An accident or medical emergency requiring blood transfusion may result in infection if the blood has not been screened for HBV. Travellers engaged in humanitarian relief activities may be exposed to infected blood or other body fluids in health care settings. Prophylaxis Vaccination (see Chapter 6). Precautions Adopt safe sexual practices and avoid the use of any potentially contaminated instruments for injection or other skin-piercing activity. HEPATITIS C Cause Hepatitis C virus (HCV), which is a hepacivirus Transmission The virus is acquired through person-to-person transmission by parenteral routes. Before screening for HCV became available, infection was mainly transmitted by transfusion of contaminated blood or blood products. Nowadays transmission frequently occurs through use of contaminated needles, syringes and other instruments used for injections and other skin-piercing procedures. Sexual transmission of hepatitis C occurs rarely. There is no insect vector or animal reservoir for HCV. Nature of the disease Most HCV infections are asymptomatic. In cases where infection leads to clinical hepatitis, the onset of symptoms is usually gradual, with anorexia, abdominal discomfort, nausea and vomiting, followed by the development of jaundice in some cases (less commonly than in hepatitis B). Most patients will develop a long-lasting chronic infection, which may lead to cirrhosis and/or liver cancer. 64 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Geographical distribution Worldwide, with regional differences in levels of prevalence. Risk for travellers Travellers are at risk if they practise unsafe behaviour involving the use of contaminated needles or syringes for injection, acupuncture, piercing or tattooing. An accident or medical emergency requiring blood transfusion may result in infection if the blood has not been screened for HCV. Travellers engaged in humanitarian relief activities may be exposed to infected blood or other body fluids in health care settings. Prophylaxis None. Precautions Adopt safe sexual practices and avoid the use of any potentially contaminated instruments for injection or other skin-piercing activity. HEPATITIS E Cause Hepatitis E virus, which has not yet been definitively classified (formerly classified as a member of the Caliciviridae). Transmission Hepatitis E is a waterborne disease usually acquired from contaminated drinking-water. Direct faecal–oral transmission from person to person is also possible. There is no insect vector. Hepatitis E virus has a domestic animal reservoirs host, such as pigs. Nature of the disease The clinical features and course of the disease are generally similar to those of hepatitis A. As with hepatitis A, there is no chronic phase. Young adults are most commonly affected. In pregnant women, there is an important difference between hepatitis E and hepatitis A. During the third trimester of pregnancy, hepatitis E takes a much more severe form with a case-fatality rate reaching 20%. Geographical distribution Worldwide. Most cases, both sporadic and epidemic, occur in countries with poor standards of hygiene and sanitation. Risk for travellers Travellers to developing countries may be at risk when exposed to poor conditions of sanitation and drinking-water control. Prophylaxis None. Precautions Travellers should follow the general conditions for avoiding potentially contaminated food and drinking-water (see Chapter 3). HIV/AIDS AND OTHER SEXUALLY TRANSMITTED INFECTIONS The most important sexually transmitted diseases and infectious agents are: HIV/AIDS human immunodeficiency virus hepatitis B hepatitis B virus syphilis Treponema pallidum gonorrhoea Neisseria gonorrhoeae chlamydial infections Chlamydia trachomatis trichomoniasis Trichomonas vaginalis chancroid Haemophilus ducreyi genital herpes herpes simplex virus (human (alpha) herpesvirus 2) genital warts human papillomavirus 65 INTERNATIONAL TRAVEL AND HEALTH 2009 Travel restrictions Some countries have adopted entry and visa restrictions for people with HIV/AIDS. Travellers who are infected with HIV should consult their personal physician for a detailed assessment and advice before travel. WHO has taken the position that there is no public health justification for entry restrictions that discriminate solely on the basis of a person’s HIV status. Transmission Infection occurs during unprotected sexual intercourse (both heterosexual and homosexual – anal, vaginal or oral). Some of these infections, such as HIV infection, hepatitis B and syphilis can also be passed on from an infected mother to her unborn or newborn baby and can be transmitted via blood transfusions. Hepatitis B and HIV infections may also be transmitted through contaminated blood products, syringes and needles used for injection, and potentially by unsterilized instruments used for acupuncture, piercing and tattooing. Nature of the diseases A number of the most common sexually transmitted infections could be included in the following syndromes: genital ulcer, pelvic inflammatory disease, urethral discharge and vaginal discharge. However, many infections are asymptomatic. Sexually transmitted infections may cause acute and chronic illness, infertility, long-term disability and death, with severe medical and psychological consequences for millions of men, women and children. Apart from being serious diseases in their own right, sexually transmitted infections increase the risk of contracting or transmitting HIV infection. Other viral infections, such as herpes simplex virus type 2 causing genital ulcer or human papillomavirus causing cervical cancer are becoming more prevalent. The presence of an untreated disease (ulcerative or non-ulcerative) can increase by a factor of up to 10 the risk of becoming infected with HIV. Individuals with HIV infection are also more likely to transmit the infection to their sexual partner if they have a sexually transmitted infection. Early diagnosis and treatment of all sexually transmitted infections are therefore important. Geographical distribution The regional differences in the prevalence of HIV infection are shown in the map. Sexually transmitted infections have been known since ancient times; they remain a major public health problem, which was compounded by the appearance of HIV/AIDS around 1980. An estimated 340 million episodes of curable sexually transmitted infections (chlamydial infections, gonorrhoea, syphilis, trichomoniasis) occur throughout the world every year. Risk for travellers For some travellers there may be an increased risk of infection. Lack of information about risk and preventive measures and the fact that travel and tourism may enhance the probability of having sex with casual partners increase the risk of contracting sexually transmitted infections. In some countries, a large proportion of sexually transmitted infections now occur as a result of unprotected sexual intercourse during international travel. There is no risk of acquiring any sexually transmitted infection from casual day-to-day contact at home, at work or socially. People run no risk of infection when sharing any means of communal transport (e.g. aircraft, boat, bus, car, train) with infected individuals. There is no evidence that HIV or other sexually transmitted infections can be acquired from insect bites. 66 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Prophylaxis Vaccination against hepatitis B (see Chapter 6). Preventive vaccines against oncogenic types of human papillomavirus are now available in some countries. For post-exposure prophylaxis see Chapter 8. Precautions The risk of acquiring a sexually transmitted infection can be prevented by abstinence from sex with occasional or causal partners during travel or reduced by safer sexual practices such as non penetrative sex and correct and consistent use of male or female condoms. Condoms also reduce the risk of unwanted pregnancy. Latex rubber condoms are relatively inexpensive, are highly reliable and have virtually no side-effects. Studies on serodiscordant couples (only one of whom is HIV-positive) have shown that, with regular sexual intercourse over a period of two years, partners who consistently use condoms have a near-zero risk of HIV infection. A man should always use a condom during sexual intercourse, each time, from start to finish, and a woman should make sure that her partner uses one. A woman can also protect herself from sexually transmitted infections by using a female condom – essentially, a vaginal pouch – which is now commercially available in some countries. It is essential to avoid injecting drugs for non-medical purposes, and particularly to avoid any type of needle-sharing to reduce the risk of acquiring hepatitis B and HIV infections. Blood transfusions should be given only with a good indication to minimize the risk of transmitting infections such as syphilis, HIV and hepatitis B infections. Medical injections, dental care or the use of needles or blades for piercing and tattooing using unsterilized equipment are also a possible source of infection and should be avoided. If an injection is needed, the traveller should try to ensure that single use needles and syringes come from a sterile package Patients under medical care who require frequent injections, e.g. diabetics, should carry sufficient sterile needles and syringes for the duration of their trip and a doctor’s authorization for their use. INFLUENZA Cause Influenza viruses of types A and B are associated with the epidemics and outbreaks typical of influenza “seasons.” Influenza type C is thought to be associated primarily with milder common cold-like illnesses. Type A viruses are further subdivided into subtypes (H1N1 and H3N2). During an influenza season, one of the two influenza A subtypes or influenza B can be predominant, while in other years all three viruses may be found. Influenza viruses undergo rapid genetic evolution which eventually results in changes to the virus’ antigenic characteristics’. Influenza vaccine virus strains are selected each year to make sure that the vaccine is matched as closely as possible to the currently circulating influenza strains. Other subtypes of influenza A viruses occur in animals and all 16 HA and 9 NA subtypes are found in birds (mainly in water fowl); inter-species transmission (1918 pandemic) and viral reassortment (1957, 1968 pandemics) may give rise to new subtypes able to infect and easily transmissible between humans and cause the next pandemic. 67 INTERNATIONAL TRAVEL AND HEALTH 2009 Transmission Respiratory transmission occurs mainly by droplets disseminated by unprotected coughs and sneezes. Short-distance airborne transmission of influenza viruses may occur, particularly in crowded enclosed spaces. Hand contamination and direct inoculation of virus is another possible source of transmission. Nature of the disease An acute respiratory infection of varying severity, ranging from asymptomatic infection to fatal disease. Typical influenza symptoms include fever with abrupt onset, chills, sore throat, non-productive cough and, often accompanied by headache, coryza, myalgia and prostration. Complications of Influenza viral infection include: primary influenza viral pneumonitis, bacterial pneumonia, otitis media and exacerbation of underlying chronic conditions. Illness tends to be most severe in the elderly and in infants and young children, and in immunocompromised hosts. Death resulting from seasonal influenza occurs mainly in the elderly and in individuals with preexisting chronic diseases. Geographical distribution Worldwide. In temperate regions, influenza is a seasonal disease occurring typically in winter months: it affects the northern hemisphere from November to April and the southern hemisphere from April to September. In tropical areas there is no clear seasonal pattern, and influenza circulation is year around typically with several peaks during rainy seasons. Risk for travellers Travellers, like local residents, are at risk in any country during the influenza season. In addition, groups of travellers that include persons from areas affected by seasonal influenza (e.g. cruise ships) may experience out-ofseason outbreaks. Travellers visiting countries in the opposite hemisphere during the influenza season are at special risk, particular if they do not have some degree of immunity through recent infection or regular vaccination. The elderly, people with pre-existing chronic diseases and young children are most susceptible to complications. Prophylaxis Vaccination before the start of the influenza season. However, vaccine for visitors to the opposite hemisphere may not be obtainable before arrival at the travel destination (see Chapter 6). For travellers in the highest risk groups for severe influenza who have not been or cannot be vaccinated, the prophylactic use of antiviral drugs such as zanamivir or oseltamivir is indicated in countries where they are available. Amantadine and rimantadine may also be considered when the circulating strains are known to be susceptible. However, the latter drugs are not active against influenza B, and high frequencies of resistance in H3N2 and less often H1N1 viruses make then unreliable for prevention currently. Precautions 68 Whenever possible, avoid crowded enclosed spaces and close contact with people suffering from acute respiratory infections. Hand-washing after direct contact with ill persons or their environment may reduce the risk of illness. Ill persons should be encouraged to practise cough etiquette (maintain distance, cover coughs and sneezes with disposable tissues or clothing, wash hands). CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS JAPANESE ENCEPHALITIS Cause Japanese encephalitis (JE) virus, which is a flavivirus. Transmission The virus is transmitted by various mosquitoes of the genus Culex. It infects pigs and various wild birds as well as humans. Mosquitoes become infective after feeding on viraemic pigs or birds. Nature of the disease Most infections are asymptomatic. In symptomatic cases, severity varies; mild infections are characterized by febrile headache or aseptic meningitis or encephalitis. Severe cases have a rapid onset and progression with headache, high fever and meningeal signs. Permanent neurological sequelae are common among survivors. Approximately 30% of severe clinical cases have a fatal outcome. Geographical distribution JE occurs in a number of countries in Asia (see Map) and occasionally in northern Queensland, Australia. Risk for travellers Low for most travellers. Visitors to rural and agricultural areas in endemic countries may be at risk, particularly during epidemics of JE. Prophylaxis Vaccination, if justified by likelihood of exposure (see Chapter 6). Precautions Avoid mosquito bites (see Chapter 3). LEGIONELLOSIS Cause Various species of Legionella bacteria, frequently Legionella pneumophila, serogroup I. Transmission Infection results from inhalation of contaminated water sprays or mists. The bacteria live in water and colonize hot-water systems at temperatures of 20–50 °C (optimal 35–46 °C). They contaminate air-conditioning cooling towers, hot-water systems, humidifiers, whirlpool spas and other watercontaining devices. There is no direct person-to-person transmission. Nature of the disease Legionellosis occurs in two distinct clinical forms: ■ Legionnaires’ disease is an acute bacterial pneumonia with rapid onset of anorexia, malaise, myalgia, headache and rapidly rising fever, progressing to pneumonia, which may lead to respiratory failure and death. ■ Pontiac fever is an influenza-like illness with spontaneous recovery after 2–5 days. Susceptibility to legionellosis increases with age, especially among smokers and people with pre-existing chronic lung disease or other immunocompromising conditions. Geographical distribution Worldwide. Risk for travellers Generally low. Outbreaks occasionally occur through dissemination of infection by contaminated water or air-conditioning systems in hotels and other facilities used by visitors. Prophylaxis None. Prevention of infection depends on regular cleaning and disinfection of possible sources. Precautions None. 69 INTERNATIONAL TRAVEL AND HEALTH 2009 LEISHMANIASIS (INCLUDING ESPUNDIA OR ORIENTAL SORE, AND KALA-AZAR) Cause Several species of the protozoan parasite Leishmania. Transmission Infection is transmitted by the bite of female phlebotomine sandflies. Dogs, rodents and other mammals are reservoir hosts for leishmaniasis. Sandflies acquire the parasites by biting infected humans or animals. Transmission from person to person by injected blood or contaminated syringes and needles is also possible. Nature of the disease Leishmaniasis occurs in two main forms: ■ Cutaneous and mucosal leishmaniasis (espundia) causes skin sores and chronic ulcers of the mucosae. Cutaneous leishmaniasis is generally selflimited but in a proportion of cases can be a chronic, progressive, disabling and mutilating disease. ■ Visceral leishmaniasis (kala-azar) affects the bone marrow, liver, spleen, lymph nodes and other internal organs. It is usually fatal if untreated. Geographical distribution Many countries in tropical and subtropical regions, including Africa, parts of central and South America, Asia, southern Europe and the eastern Mediterranean. Over 90% of all cases of visceral leishmaniasis occur in Bangladesh, Brazil, India, Nepal and Sudan. More than 90% of all cases of cutaneous leishmaniasis occur in Afghanistan, Algeria, Brazil, the Islamic Republic of Iran, Saudi Arabia and the Syrian Arab Republic. Risk for travellers Visitors to rural and forested areas in endemic countries are at risk. Prophylaxis None. Precautions Avoid sandfly bites, particularly after sunset, by using repellents and insecticide-impregnated bednets. The bite leaves a non-swollen red ring, which can alert the traveller to its origin. LEPTOSPIROSIS (INCLUDING WEIL DISEASE) Cause Various spirochaetes of the genus Leptospira. Transmission Infection occurs through contact between the skin (particularly skin abrasions) or mucous membranes and water, wet soil or vegetation contaminated by the urine of infected animals, notably rats. Occasionally infection may result from direct contact with urine or tissues of infected animals, or from consumption of food contaminated by the urine of infected rats. Nature of the disease Leptospiral infections take many different clinical forms, usually with sudden onset of fever, headache, myalgia, chills, conjunctival suffusion and skin rash. The disease may progress to meningitis, haemolytic anaemia, jaundice, haemorrhagic manifestations and other complications, including hepatorenal failure. Geographical distribution Worldwide. Most common in tropical countries. Risk for travellers Low for most travellers. There is an occupational risk for farmers engaged in paddy rice and sugar cane production. Visitors to rural areas and in contact 70 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS with water in canals, lakes and rivers may be exposed to infection. There is increased risk after recent floods. The risk may be greater for those who practise canoeing, kayaking or other activities in water. Outbreaks associated with eco-sports activities have occurred. Prophylaxis Doxycycline may be used for prophylaxis if exposure is likely. Vaccine against local strains is available for workers where the disease is an occupational hazard, but it is not commercially available in most countries. Precautions Avoid swimming or wading in potentially contaminated waters including canals, ponds, rivers, streams and swamps. Avoid all direct or indirect contact with rodents. LISTERIOSIS Cause The bacterium Listeria monocytogenes. Transmission Listeriosis affects a variety of animals. Foodborne infection in humans occurs through the consumption of contaminated foods, particularly unpasteurized milk, soft cheeses, vegetables and prepared meat products such as pâté. Listeriosis multiplies readily in refrigerated foods that have been contaminated, unlike most foodborne pathogens. Transmission can also occur from mother to fetus or from mother to child during birth. Nature of the disease Listeriosis causes meningoencephalitis and/or septicaemia in adults and newborn infants. In pregnant women, it causes fever and abortion. Newborn infants, pregnant women, the elderly and immunocompromised individuals are particularly susceptible to listeriosis. In others, the disease may be limited to a mild acute febrile episode. In pregnant women, transmission of infection to the fetus may lead to stillbirth, septicaemia at birth or neonatal meningitis. Geographical distribution Worldwide, with sporadic incidence. Risk for travellers Generally low. Risk is increased by consumption of unpasteurized milk and milk products and prepared meat products. Prophylaxis None. Precautions Avoid consumption of unpasteurized milk and milk products. Pregnant women and immunocompromised individuals should take stringent precautions to avoid infection by listeriosis and other foodborne pathogens (see Chapter 3). LYME BORRELIOSIS (LYME DISEASE) Cause The spirochaete Borrelia burgdorferi, of which there are several different serotypes. Transmission Infection occurs through the bite of infected ticks, both adults and nymphs, of the genus Ixodes. Most human infections result from bites by nymphs. Many species of mammals can be infected, and deer act as an important reservoir. 71 INTERNATIONAL TRAVEL AND HEALTH 2009 Nature of the disease The disease usually has its onset in summer. Early skin lesions have an expanding ring form, often with a central clear zone. Fever, chills, myalgia and headache are common. Meningeal involvement may follow. Central nervous system and other complications may occur weeks or months after the onset of illness. Arthritis may develop up to 2 years after onset. Geographical distribution There are endemic foci of Lyme borreliosis in forested areas of Asia, northwestern, central and eastern Europe, and the USA. Risk for travellers Generally low. Visitors to rural areas in endemic regions, particularly campers and hikers, are at risk. Prophylaxis None. Precautions Avoid tick-infested areas and exposure to ticks (see Chapter 3). If a bite occurs, remove the tick as soon as possible. MALARIA See Chapter 7 and Map. MENINGOCOCCAL DISEASE Cause The bacterium Neisseria meningitidis, of which 12 serogroups are known. Most cases of meningococcal disease are caused by serogroups A, B and C; less commonly, infection is caused by serogroups Y (emerging in the United States) and W-135 (particularly in Burkina Faso). Some small-scale outbreaks caused by serogroup X have been reported in Niger and Uganda. Epidemics in Africa are usually caused by N. meningitidis type A. Transmission Transmission occurs by direct person-to-person contact, and through respiratory droplets from the nose and pharynx of infected persons, patients or asymptomatic carriers. Humans are the only reservoir. Nature of the disease Most infections do not cause clinical disease. Many infected people become asymptomatic carriers of the bacteria and serve as a reservoir and source of infection for others. In general, susceptibility to meningococcal disease decreases with age, although there is a small increase in risk in adolescents and young adults. Meningococcal meningitis has a sudden onset of intense headache, fever, nausea, vomiting, photophobia and stiff neck, plus various neurological signs. The disease is fatal in 5–10% of cases even with prompt antimicrobial treatment in good health care facilities; among individuals who survive, up to 20% have permanent neurological sequelae. Meningococcal septicaemia, in which there is rapid dissemination of bacteria in the bloodstream, is a less common form of meningococcal disease, characterized by circulatory collapse, haemorrhagic skin rash and high fatality rate. Geographical distribution Sporadic cases are found worldwide. In temperate zones, most cases occur in the winter months. Localized outbreaks occur in enclosed crowded spaces (e.g. dormitories, military barracks). In sub-Saharan Africa, in a zone stretching across the continent from Senegal to Ethiopia (the African “meningitis belt”), large outbreaks and epidemics take place during the dry season (November–June). Recent reports of endemic occurrence of group Y meningococcal disease in the United States, and outbreaks cau- 72 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS sed by serogroup W-135 strains in Saudi Arabia and sub-Saharan Africa, particularly Burkina Faso, suggest that these serogroups may be gaining in importance. Risk for travellers Generally low. However, the risk is considerable if travellers are in crowded conditions or take part in large population movements such as pilgrimages in the Sahel meningitis belt. Localized outbreaks occasionally occur among travellers (usually young adults) in camps or dormitories. See also Chapter 6 for specific risks for travellers. Prophylaxis Vaccination is available for N. meningitidis types A, C, Y and W135 (see Chapter 6). Protection by vaccines is group-specific, and appropriate vaccines need to be administered to protect against the most prevalent serogroup at the destination country of the traveller. Precautions Avoid overcrowding in confined spaces. Following close contact with a person suffering from meningococcal disease, medical advice should be sought regarding chemoprophylaxis. ONCHOCERCIASIS Cause Onchocerca volvulus (a nematode) Transmission Onchocercias (river blindness) is transmitted through the bite of infected blackflies. Nature of the disease Onchocerciasis is a chronic parasitic disease occurring mainly in subSaharan western Africa in which adult worms are found in fibrous nodules under the skin. They discharge microfilaria, which migrate through the skin causing dermatitis, and reach the eye causing damage that results in blindness. Geographical distribution Onchocerciasis occurs mainly in western and central Africa, also in central and South America. Risk for travellers Generally low, unless travel involves extensive exposure to the vectors in endemic areas. Prophylaxis None. Precautions Avoid exposure to the bites of blackflies in endemic areas. PLAGUE Cause The plague bacillus, Yersinia pestis. Transmission Plague is a zoonotic disease affecting rodents and transmitted by fleas from rodents to other animals and to humans. Direct person-to-person transmission does not occur except in the case of pneumonic plague, when respiratory droplets may transfer the infection from the patient to others in close contact. 73 INTERNATIONAL TRAVEL AND HEALTH 2009 Nature of the disease Plague occurs in three main clinical forms: ■ Bubonic plague is the form that usually results from the bite of infected fleas. Lymphadenitis develops in the drainage lymph nodes, with the regional lymph nodes most commonly affected. Swelling, pain and suppuration of the lymph nodes produces the characteristic plague buboes. ■ Septicaemic plague may develop from bubonic plague or occur in the absence of lymphadenitis. Dissemination of the infection in the bloodstream results in meningitis, endotoxic shock and disseminated intravascular coagulation. ■ Pneumonic plague may result from secondary infection of the lungs following dissemination of plague bacilli from other body sites. It produces severe pneumonia. Direct infection of others may result from transfer of infection by respiratory droplets, causing primary pulmonary plague in the recipients. Without prompt and effective treatment, 50–60% of cases of bubonic plague are fatal, while untreated septicaemic and pneumonic plague are invariably fatal. Geographical distribution There are natural foci of plague infection in rodents in many parts of the world. Wild rodent plague is present in central, eastern and southern Africa, South America, the western part of North America and in large areas of Asia. In some areas, contact between wild and domestic rats is common, resulting in sporadic cases of human plague and occasional outbreaks. Risk for travellers Generally low. However, travellers in rural areas of plague-endemic regions may be at risk, particularly if camping or hunting or if contact with rodents takes place. Prophylaxis A vaccine effective against bubonic plague is available exclusively for persons with a high occupational exposure to plague; it is not commercially available in most countries. Precautions Avoid any contact with live or dead rodents. RABIES Cause The rabies virus, a rhabdovirus of the genus Lyssavirus. Transmission Rabies is a zoonotic disease affecting a wide range of domestic and wild mammals, including bats. Infection of humans usually occurs through the bite of an infected animal as the virus is present in the saliva. Any other contact with a rabies-susceptible species such as a penetrating scratch with bleeding and licking of broken skin and mucosa in an area where rabies is present should be treated with caution. In developing countries, transmission is usually through dog bites. Person-to-person transmission has not been laboratory-confirmed. Nature of the disease An acute viral encephalomyelitis, which is almost invariably fatal. The initial signs include a sense of apprehension, headache, fever, malaise and sensory changes around the site of the animal bite. Excitability, hallucinations and aerophobia are common, followed in some cases by fear of water 74 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS (hydrophobia) due to spasms of the swallowing muscles, progressing to delirium, convulsions and death a few days after onset. A less common form, paralytic rabies, is characterized by loss of sensation, weakness, pain and paralysis. Geographical distribution Rabies is present in mammals in many countries worldwide (see Map). Most of the estimated 55 000 rabies deaths per year in Africa and Asia alone occur in developing countries and follow a dog bite. More information is available on www.who.int/rabies/rabnet/en. Risk for travellers In rabies-endemic areas, travellers may be at risk if there is exposure to a rabies-susceptible animal species (domestic, particularly dogs and cats, or wild, including bats). Travellers with extensive outdoor exposure and certain occupational activities are at higher risk even if the duration of the trip is short. Spelunkers (cavers) should not handle bats. Children are considered at higher risk because they may play with animals and often do not report bites or scratches. Prophylaxis Vaccination for travellers with a foreseeable significant risk of exposure to rabies or travelling to a hyperendemic area where modern rabies vaccine may not be available (see Chapter 6). Precautions Avoid contact with wild animals and stray domestic animals, particularly dogs and cats, in rabies-endemic areas. If bitten by an animal that is potentially infected with rabies, or after other suspect contact as defined above, immediately clean the wound thoroughly with disinfectant or with soap or detergent and water. Medical assistance should be sought immediately and post-exposure prophylaxsis initiated if indicated (see Chapter 6). The vaccination status of the animal involved should not be a criterion for withholding post-exposure prophylaxis unless the vaccination has been thoroughly documented and vaccine of known potency has been used. In the case of domestic animals, the suspect animal should be kept under observation for a period of 10 days. After 10 days, if the animal under observation is healthy, post-exposure prophylaxis may be stopped. SARS (SEVERE ACUTE RESPIRATORY SYNDROME) Cause SARS coronavirus (SARS-CoV) – virus identified in 2003. SARS-CoV is thought to be an animal virus from an as–yet -uncertain animal reservoir, perhaps bats, that spread to other animals (civet cats) ,and first infected humans in the Guangdong province of southern China in 2002. Transmission An epidemic of SARS affected 26 countries and resulted in over 8000 cases in 2003. Since then, a small number of cases have occurred as a result of laboratory accidents or, possibly, through animal-to-human transmission (Guangdong, China). Transmission of SARS-CoV is primarily from person-to-person. It appears to have occurred mainly during the second week of illness, which corresponds to the peak of virus excretion in respiratory secretions and stool, and when cases with severe disease start to deteriorate clinically. Most cases of human-to-human transmission occurred in the healthcare setting, in the absence of adequate infection control precautions. The implementation of 75 INTERNATIONAL TRAVEL AND HEALTH 2009 appropriate infection control practices brought the global outbreak to an end. Nature of the disease Symptoms are flu-like and include fever, malaise, muscle aches and pains (myalgia), headache, diarrhoea, and shivering (rigors). No individual symptom or cluster of symptoms has proved to be specific for a diagnosis of SARS. Although fever is the most frequently reported symptom, it is sometimes absent on initial measurement, especially in elderly and immunosuppressed patients. Cough (initially dry), shortness of breath, and diarrhoea present in the first and/or second week of illness. Severe cases often evolve rapidly, progressing to respiratory distress and requiring intensive care. Geographical distribution The distribution is based on the 2002–2003 epidemic. The disease appeared in November 2002 in the Guangdong province of southern China. This area is considered as a potential zone of re-emergence of SARS-CoV. Other countries/areas in which chains of human-to-human transmission occurred after early importation of cases were Hong Kong Special Administrative Region of China and Taiwan (Province of China), Toronto in Canada, Singapore, and Hanoi in Viet Nam. Risk for travellers Currently, no areas of the world are reporting transmission of SARS. Since the end of the global epidemic in July 2003, SARS has reappeared four times – three times from laboratory accidents (Singapore; Taiwan, Province of China), and once in southern China where the source of infection remains undetermined although there is circumstantial evidence of animal-to-human transmission. Should SARS re-emerge in epidemic form, WHO will provide guidance on the risk of travel to affected areas. Travellers should stay informed about current travel recommendations. However, even during the height of the 2003 epidemic, the overall risk of SARS-CoV transmission to travellers was low. Prophylaxis None. Experimental vaccines are under development. Precautions Follow any travel recommendations and health advice issued by WHO. SCHISTOSOMIASIS (BILHARZIASIS) Cause Several species of parasitic blood flukes (trematodes), of which the most important are Schistosoma mansoni, S. japonicum, S.mekongi and S. haematobium. Transmission Infection occurs in fresh water containing larval forms (cercariae) of schistosomes, which develop in snails. The free-swimming larvae penetrate the skin of individuals swimming or wading in water. Snails become infected as a result of excretion of eggs in human urine or faeces. Nature of the disease Chronic conditions in which adult flukes live for many years in the veins (mesenteric or vesical) of the host where they produce eggs, which cause damage to the organs in which they are deposited. The symptoms depend on the main target organs affected by the different species, with S. mansoni, 76 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS S. mekongi and S. japonicum causing hepatic and intestinal signs and S. haematobium causing urinary dysfunction. The larvae of some schistosomes of birds and other animals may penetrate human skin and cause a self-limiting dermatitis, “swimmers itch”. These larvae are unable to develop in humans. Geographical distribution S. mansoni occurs in many countries of sub-Saharan Africa, in the Arabian peninsula, and in Brazil, Suriname and Venezuela. S. japonicum is found in China, in parts of Indonesia, and in the Philippines. S. haematobium is present in sub-Saharan Africa and in eastern Mediter-ranean areas. S. mekongi is found along the Mekong River in northern Cambodia and in the south of the Lao People’s Democratic Republic (see Map). Risk for travellers In endemic areas, travellers are at risk while swimming or wading in fresh water. Prophylaxis None. Precautions Avoid direct contact (swimming or wading) with potentially contaminated fresh water in endemic areas. In case of accidental exposure, dry the skin vigorously to reduce penetration by cercariae. Avoid drinking, washing, or washing clothing in water that may contain cercariae. Water can be treated to remove or inactivate cercariae by paper filtering or use of iodine or chlorine. TICK-BORNE ENCEPHALITIS (SPRING–SUMMER ENCEPHALITIS) Cause The tick-borne encephalitis (TBE) virus is a flavivirus. Three subtypes of the causative agent are known. The most common subtypes are the European subtype, the Far Eastern subtype (Spring Summer encephalitis) and the Siberian subtype. Other closely related viruses cause similar diseases. Transmission Infection is transmitted by the bite of infected ticks or by ingestion of unpasteurized milk. There is no direct person-to-person transmission. Some related viruses, also tick-borne, infect animals such as birds, deer (louping-ill), rodents and sheep. Nature of the disease Infection may induce an influenza-like illness, with a second phase of fever occurring in 10% of cases. Encephalitis develops during the second phase and may result in paralysis, permanent sequelae or death. Severity of illness increases with age. The Far Eastern subtype causes more severe symptoms and sequelae than the European subtype. Geographical distribution The European subtype is present in large parts of central and eastern Europe, particularly Austria, southern Germany or northern Switzerland, the Baltic states (Estonia, Latvia, Lithuania), the Czech Republic, Hungary and Poland; the Far Eastern subtype is found from north eastern Europe to China and Japan, and the Siberian subtype from northern Europe to Siberia. The disease is seasonal; most cases occur during April to November. The risk is highest in forested areas up to an altitude of about 1400 m. Risk for travellers In endemic areas during the summer months, travellers are at risk when hiking or camping in rural or forested areas. 77 INTERNATIONAL TRAVEL AND HEALTH 2008 Prophylaxis A vaccine against TBE is available (see Chapter 6). Precautions Avoid bites by ticks by wearing long trousers and closed footwear when hiking or camping in endemic areas. If a bite occurs, the tick should be removed as soon as possible. TRYPANOSOMIASIS 1. African trypanosomiasis (sleeping sickness) Cause Protozoan parasites Trypanosoma brucei gambiense and T. b. rhodesiense. Transmission Infection occurs through the bite of infected tsetse flies. Humans are the main reservoir host for T. b. gambiense. Domestic cattle and wild animals, including antelopes, are the main animal reservoir of T. b. rhodesiense. Nature of the disease T. b. gambiense causes a chronic illness with onset of symptoms after a prolonged incubation period of weeks or months. T. b. rhodesiense causes a more acute illness, with onset a few days or weeks after the infected bite; often, there is a striking inoculation chancre. Initial clinical signs include severe headache, insomnia, enlarged lymph nodes, anaemia and rash. In the late stage of the disease, there is progressive loss of weight and involvement of the central nervous system. Without treatment, the disease is invariably fatal. Geographical distribution T. b. gambiense is present in foci in the tropical countries of western and central Africa. T. b. rhodesiense occurs in eastern Africa, extending south as far as Botswana. Risk for travellers Travellers are at risk in endemic regions if they visit rural areas for hunting, fishing, safari trips, sailing or other activities in endemic areas. Prophylaxis None. Precautions Travellers should be aware of the risk in endemic areas and as far as possible avoid any contact with tsetse flies. However, bites are difficult to avoid because tsetse flies can bite through clothing. Travellers should be warned that tsetse flies bite during the day and are not repelled by available insectrepellent products. The bite is painful, which helps to identify its origin, and travellers should seek medical attention promptly if symptoms develop subsequently. 2. American trypanosomiasis (Chagas disease) Cause Protozoan parasite Trypanosoma cruzi. Transmission Infection is transmitted by blood-sucking triatomine bugs (“kissing bugs”). Oral transmission by ingestion of unprocessed freshly squeezed sugar cane in areas where the vector is present has also been reported. During feeding, infected bugs excrete trypanosomes, which can then contaminate the conjunctiva, mucous membranes, abrasions and skin wounds including the bite wound. Transmission also occurs by blood transfusion when blood has been obtained from an infected donor. Congenital infection is possible, due to parasites crossing the placenta during pregnancy. T. cruzi infects many species of wild and domestic animals as well as humans. 78 CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Nature of the disease In adults, T. cruzi causes a chronic illness with progressive myocardial damage leading to cardiac arrhythmias and cardiac dilatation, and gastrointestinal involvement leading to mega-oesophagus and megacolon. T. cruzi causes acute illness in children, which is followed by chronic manifestations later in life. Geographical distribution American trypanosomiasis occurs in Mexico and in central and South America (as far south as central Argentina and Chile). The vector is found mainly in rural areas where it lives in the walls of poorly-constructed housing. Risk for travellers In endemic areas, travellers are at risk when trekking, camping or using poor-quality housing. Precautions Avoid exposure to blood-sucking bugs. Residual insecticides can be used to treat housing. Exposure can be reduced by the use of bednets in houses and camps. TUBERCULOSIS Cause Mycobacterium tuberculosis, the tubercle bacillus. Infection is usually by direct airborne transmission from person to person. Nature of the disease Exposure to M. tuberculosis may lead to infection, but most infections do not lead to disease. The risk of developing disease following infection is generally 5–10% during the lifetime, but may be increased by various factors, notably immunosuppression (e.g. advanced HIV infection). Multidrug resistance refers to strains of M. tuberculosis that are resistant to at least isoniazid and rifampicin (MDR-TB). The resistant strains do not differ from other strains in infectiousness, likelihood of causing disease, or general clinical effects; however, if they do cause disease, treatment is more difficult and the risk of death will be higher. Extensively drug-resistant TB (XDR-TB) is TB that is resistant to at least isoniazid and rifampin, to any fluoroquinolone and to at least one of the injectable second-line anti-TB drugs capreomycin, kanamycin and amikacin. Geographical distribution Worldwide. The risk of infection differs between countries, as shown on the map of estimated TB incidence. Risk for travellers Low for most travellers. Long-term travellers (over 3 months) to a country with a higher incidence of tuberculosis than their own may have a risk of infection comparable to that for local residents. As well as the duration of the visit, living conditions are important in determining the risk of infection: high-risk settings include health facilities, shelters for the homeless, and prisons. Prophylaxis BCG vaccine is of limited use for travellers but may be advised for infants and young children in some situations (see Chapter 6). Precautions Travellers should avoid close contact with known tuberculosis patients. For travellers from low-incidence countries who may be exposed to infection in relatively high-incidence countries (e.g. health professionals, humanitarian relief workers, missionaries), a baseline tuberculin skin test is advisable in order to compare with retesting after return. If the skin reaction to tuber- 79 INTERNATIONAL TRAVEL AND HEALTH 2008 culin suggests recent infection, the traveller should receive, or be referred for, treatment for latent infection. Patients under treatment for tuberculosis should not travel until the treating physician has documented, by laboratory examination of sputum, that the patient is not infectious and therefore of no risk to others. The importance of completing the prescribed course of treatment should be stressed. TYPHOID FEVER Cause Salmonella typhi, the typhoid bacillus, which infects only humans. Similar paratyphoid and enteric fevers are caused by other species of Salmonella, which infect domestic animals as well as humans. Transmission Infection is transmitted by consumption of contaminated food or water. Occasionally direct faecal–oral transmission may occur. Shellfish taken from sewage-polluted beds are an important source of infection. Infection occurs through eating fruit and vegetables fertilized by night soil and eaten raw, and milk and milk products that have been contaminated by those in contact with them. Flies may transfer infection to foods, resulting in contamination that may be sufficient to cause human infection. Pollution of water sources may produce epidemics of typhoid fever, when large numbers of people use the same source of drinking-water. Nature of the disease A systemic disease of varying severity. Severe cases are characterized by gradual onset of fever, headache, malaise, anorexia and insomnia. Constipation is more common than diarrhoea in adults and older children. Without treatment, the disease progresses with sustained fever, bradycardia, hepatosplenomegaly, abdominal symptoms and, in some cases, pneumonia. In white-skinned patients, pink spots (papules), which fade on pressure, appear on the skin of the trunk in up to 50% of cases. In the third week, untreated cases develop additional gastrointestinal and other complications, which may prove fatal. Around 2–5% of those who contract typhoid fever become chronic carriers, as bacteria persist in the biliary tract after symptoms have resolved. Geographical distribution Worldwide. The disease occurs most commonly in association with poor standards of hygiene in food preparation and handling and where sanitary disposal of sewage is lacking. Risk for travellers Generally low risk for travellers, except in parts of northern and western Africa, in southern Asia, parts of Indonesia and in Peru. Elsewhere, travellers are usually at risk only when exposed to low standards of hygiene with respect to food handling, control of drinking-water quality, and sewage disposal. Prophylaxis Vaccination (see Chapter 6). Precautions Observe all precautions against exposure to foodborne and waterborne infections (see Chapter 3). TYPHUS FEVER (EPIDEMIC LOUSE-BORNE TYPHUS) Cause 80 Rickettsia prowazekii. CHAPTER 5. INFECTIOUS DISEASES OF POTENTIAL RISK FOR TRAVELLERS Transmission The disease is transmitted by the human body louse, which becomes infected by feeding on the blood of patients with acute typhus fever. Infected lice excrete rickettsia onto the skin while feeding on a second host, who becomes infected by rubbing louse faecal matter or crushed lice into the bite wound. There is no animal reservoir. Nature of the disease The onset is variable but often sudden, with headache, chills, high fever, prostration, coughing and severe muscular pain. After 5–6 days, a macular skin eruption (dark spots) develops first on the upper trunk and spreads to the rest of the body but usually not to the face, palms of the hands or soles of the feet. The case-fatality rate is up to 40% in the absence of specific treatment. Louse-borne typhus fever is the only rickettsial disease that can cause explosive epidemics. Geographical distribution Typhus fever occurs in colder (i.e. mountainous) regions of central and eastern Africa, central and South America, and Asia. In recent years, most outbreaks have taken place in Burundi, Ethiopia and Rwanda. Typhus fever occurs in conditions of overcrowding and poor hygiene, such as prisons and refugee camps. Risk for travellers Very low for most travellers. Humanitarian relief workers may be exposed in refugee camps and other settings characterized by crowding and poor hygiene. Prophylaxis None. Precautions Cleanliness is important in preventing infestation by body lice. Insecticidal powders are available for body-louse control and treatment of clothing for those at high risk of exposure. YELLOW FEVER Cause The yellow fever virus, an arbovirus of the Flavivirus genus. Transmission Yellow fever in urban and some rural areas is transmitted by the bite of infective Aedes aegypti mosquitoes and by other mosquitoes in the forests of South America. The mosquitoes bite during daylight hours. Transmission can occur at altitudes up to 2300 metres. Yellow fever virus infects humans and monkeys. In jungle and forest areas, monkeys are the main reservoir of infection, with transmission from monkey to monkey carried out by mosquitoes. The infective mosquitoes may bite humans who enter the forest area, usually causing sporadic cases or small outbreaks. In urban areas, monkeys are not usually involved and infection is transmitted among humans by mosquitoes. Introduction of infection into densely populated urban areas can lead to large epidemics of yellow fever. In Africa, an intermediate pattern of transmission is common in humid savannah regions. Mosquitoes infect both monkeys and humans, causing localized outbreaks. Nature of the disease Although most of the infections are asymptomatic and not detected, some infections lead to an acute illness characterized by two phases. Initially, there 81 INTERNATIONAL TRAVEL AND HEALTH 2009 is fever, muscular pain, headache, chills, anorexia, nausea and/or vomiting, often with bradycardia. About 15% of patients progress to a second phase after a few days, with resurgence of fever, development of jaundice, abdominal pain, vomiting and haemorrhagic manifestations; half of these patients die 10–14 days after onset of illness. Geographical distribution The yellow fever virus is endemic in some tropical areas of Africa and central and South America (see map). The number of epidemics has increased since the early 1980s. Other countries are considered to be at risk of introduction of yellow fever due to the presence of the vector and suitable primate hosts (including Asia, where yellow fever has never been reported). Risk for travellers Travellers are at risk in all areas where yellow fever is endemic. The risk is greatest for visitors who enter forest and jungle areas. Prophylaxis Vaccination (see Chapter 6). In some countries, yellow fever vaccination is mandatory for visitors (see Country list). Precautions Avoid mosquito bites during the day and evening (se evening (see Chapter 3). Further reading Disease outbreak news: http://www.who.int/csr/don/en Heymann D, ed. Control of communicable diseases manual, 18th ed. Washington, DC, American Public Health Association, 2005. Weekly epidemiological record: http://www.who.int/wer/ WHO information on infectious diseases: http://www.who.int/csr/disease/en 82