Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Resting potential wikipedia , lookup
Threshold potential wikipedia , lookup
Electrophysiology wikipedia , lookup
Cushing reflex wikipedia , lookup
Intracranial pressure wikipedia , lookup
Biofluid dynamics wikipedia , lookup
Common raven physiology wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Hemodynamics wikipedia , lookup
Haemodynamic response wikipedia , lookup
Circulatory system wikipedia , lookup
Homeostasis wikipedia , lookup
Cardiac action potential wikipedia , lookup
Cardiac output wikipedia , lookup
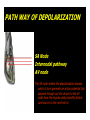
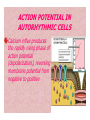
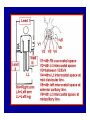
Dr.Eman Al.Hadethy Al-Faluoja.College of medicine/CVS Physiology Cardiovascular System Heart The heart • Is the transport system pumps: the delivery routs are the blood vessels. Using blood as the transport medium, the heart propels oxygen,nutrients,wastes and other substances to and past the body cells. Anatomy View Deep cut away-view Pulmonary and systemic circulation • The heart consist of two • side-by- side pumps. The bl.v are the pipes carry blood through the body. Pulmonary and Systemic Circuit Magnified view of the heart cell •Nucleus •Intercalated disc •Cardiac myofibril Cell junction • Desmosome adjacent cell together when m.cell contract they pull each other. • Gap junction imp. for different reason allow stimulating impulse to move across the heart from cell to cell so the heart beat as entire unit if each cardiac m. cell allow to do something the heart useless as a pump. Intrinsic conduction system • Intrinsic conduction system sets the basic rhythm of the beating heart. It consists of autorhythmic cardiac cells that initiate and distribute impulses (action potentials) through out the heart. Location of autorythmic cell *SA node *internodal pathway *AV node *AV bundle *Bundle branches *Purkinje fibers PATH WAY OF DEPOLARIZATION SA Node Internodal pathway AV node The SA node initiate the depolarization impulse which in turn generate an action potential that speared through out the atrium to the AV node here the impulse delay breafilly before continue on to the ventricle to • • • • To the AV node AV bundle Bundle branches and Purkinje fibers. Action potential which spread from the autorhythmic cells of intrinsic conduction system to the contractile cells, are electrical events. Subsequent contraction of the contractile cells is a mechanical event that causes heart beat Correlation between heart electrical activity and ECG wave tracing *P wave=Atrial depolarization followed by atrial contraction. *QRS wave=V.depolarization followed by V.contraction. *T wave=V.Repolarization followed by V.relaxation. * Atrial repolarization is hidden by QRS complex. SUMMARY • The intrinsic conduction system of the heart initiates depolarization impulses. • Action potentials spread throughout the heart, causing a coordinated heart contraction • An ECG wave tracing records the electrical activity of the heart. CARDIAC ACTION POTENTIAL The coordinated contractions of the heart result from electrical changes that take place in cardiac cells GOALS * To understand the ionic basis of the pacemaker potential and action potential in a cardiac autorhythmic cell * To understand the ionic basis of an action potential in a cardiac contractile (ventricular) cell. * To understand that autorhythmic and contractile cells are electrically coupled by current that flows through gap junctions. AUTORHYTHMIC CELLS In the intrinsic conduction system generate action potentials that spread throughout the heart, triggering contractions in the contractile cells. Action Potential • Action potentials generated by autorhythmic cells create waves of depolarization that spread to contractile cells via gap junctions *If depolarization reaches threshold the contractile cells in turn generate action potentials first depolarizing then repolarizing. *Contractile cells contract after depolarization and relax after repolarization AUTORHYTHMIC CELL Plasma channel • Sodium channel • Fast calcium • Potassium channel Protein Channel *Sodium and fast Ca++ channels allow Na+ and Ca to enter the cell * where as potassium channel allow K+ to leave the cell. Membrane potential *The movement of ions effect the membrane potential the voltage Crosse the membrane potential is result of the relative the concentration of the ions inside or outside of the plasma membrane * if there are more + ions outside the cell then inside the cell is relatively _ as shown here. Many transport channel are voltage regulated that is open and close in response to specific voltage level across the membrane. GAP JUNCTION * The gap junction adjacent the cell this allow the ions to pass between the cell allowing of rapid effect initiate depolarization in one cell and another and so on. OVERVIW:INTIATION OF ACTION POTENTIALS IN AUTORHYTHMIC CELLS Autorhythmic cells has unique ability to depolarized spontaneously resulting 1.Pacemaker potential once threshold is reach an action potential initiated which become with further 2.Depolarization and reversal of membrane potential 3.Repolrization return the cell to resting membrane potential. the cell spontaneous begin to slow depolarize once again and sequence is repeated. ACTION POTENTIAL AUTORHYTHMIC CELLS 1.Pacemaker potential Autorhythmic cells begin depolarizing due to slow continuous influx of Na+ & reduced efflux of K+. AUTORHYTHMIC CELLS * Due to Na+ influx,the inner membrane gradually become less negative, generating the pacemaker potential. ACTION POTENTIAL IN AUTORHYTHMIC CELLS 2.Depolarization and reversal of membrane potential When membrane potential gets to(-40) mv.It is reached threshold for initiated an action potential, fast calcium channels open and calcium rushes in. ACTION POTENTIAL IN AUTORHYTHMIC CELLS Calcium influx produces the rapidly rising phase of action potential (depolarization), reversing membrane potential from negative to positive ACTION POTENTIAL IN AUTORHYTHMIC CELLS 3.Repolarization Reversal of membrane potential triggers opening of K+ channels, resulting in rapid efflux of K+.(rapidly K+ leave the cell). Potassium efflux produces repolarization bring the membrane potential back down to resting potential Action potential in Autorhythmic cells Although not shown her, ionic pumps actively transport calcium back to the extra- cellular space during repolarization Na+/K+ pumps also pump sodium out and K+ in. Cardiac contractile cell • This cell like • autorythmic cell to generate action potential &pass the impulses down align before the cell contract Cardiac Contractile Cell • Like the autorhythmic cell it • • • • has protein transport channels but slightly different. Gap junction:-link autorhythmic & contractile cell & contractile with each other SR which is storage site of Ca ion &Channel with SR allow the Ca to the cell. Myofilaments are the contractile of the C.m.cell. Action Potential in Contractile cells • • • • • 1- Depolarization 2- Plateau 3- Repolarization Once threshold is reached the action potential start with depolarization during plateau period ions movement balances out & memb.potential return to resting state 1-Depolarization: during depolarization.in autorhythmic cells,+ve ions move through gap junctions to adjacent contractile cells Depolarization • The entry of +ve ions (Na+,Ca+) creates a small voltage change initiating depolarization. Depolarization • Voltage change stimulates opening of voltageregulated fast sodium channels. • Rapid influx of Na results in dep.of memb.potential. 2-Plateau: Depolarization also triggers opening of slow Ca channels,allowing Ca entry from EC space & SR. At the same time K+ efflux begins Slow ca+ influx briefly balances the early K+ efflux,producing a plateau in the action potential tracing intracellular Ca+ initiates cell contraction. REPOLARIZATION • Ca+ channels • close while more K+ channels open, thus rapidly repolarizing the membrane • Rapid K+ efflux results in repolarization. Although not shown here,ionic pumps actively transport Ca+ back to the SR & extracellular space during repolarization. • Na+/K+ pumps • also pump Na+out • &K+ in. Cardiac Cycle (the mechanical events) The cardiac cycle includes all events related to the flow of bl. Through the heart during one complete heart beat. Cardiac Cycle • During the cardiac cycle, • • • • • heart valves open & close in response to differences in bl.p.on their two sides. These figure show Pulmonary semi lunar V. Aortic semilunar V. Lt. AV valve (mitral v) Rt. AV valve (tricuspid). Over View: Phases of the Cardiac Cycle 1.Ventricular filling:- occur during mid-to-late V.diastol 2. Ventricular Emptying (ventricular systole) which include:- Isovolumetric contraction - Ventricular ejection. - Isovolumetric relaxation occur during early diastole. Cardiac Cycle • Inject dye into superior & inferior venae cava to show bl.flow on Rt.side of heart Phases of cardiac cycle • 1st phase:-of cardiac cycle. 1- Ventricular filling (Midto-Late V.D) when heart chamber relax A- Bl.flow passively into the atria, through open AV valves,& into ventricles, where the pressure is lower. Ventricular filling B- Atria contract, forcing the remaining blood into ventricles. C- During the last 3rd of ventricular diastolic time the atria contract & give an additional 20%-30% of the filling of the ventricle during each cardiac cycle. Function of the atria as pumps • The propagated action potential which is represented by p wave on (ECG) precedes atrial contraction. • Bl.normally flows continually from the great veins into the atria & about 70% of this flows pass directly through the atria into the ventricles even before the atria contract. • Then, trial contraction causes an additional 2030% filling of the ventricles. Central venous pressure (CVP) • The p.in the Rt atrium is called CVP • Measured clinically from the level of the column of • • • • • bl.in the neck veins (jugular v) While subject is reclining at an angle of about 450 where the heart & sternal angle at the same level. Venous pressure can be also measured by inserting a syringe needle connected to a pressure recorder or to a water manometer directly into a vein. CVP can be measured accurately by inserting a catheter through the veins into the Rt.atrium. CVP is decreased during inspiration (negative pressure breathing) & shock. Increased by expiration&heart failure. Jugular venous pressure • During cardiac cycle ,the atrial pressure • • • are transmitted to the great veins, producing 3 characteristic waves in the jugular pulse (also called jvp) & these are: 1. The a wave 2. The c wave 3. The v wave. Jugular venous pressure • The a wave : which is caused by atrial contraction and the atrial pressure increases (about 4-6mmHg in the right atrium and 78mmHg in the left atrium). • The c wave: occurs when the ventricles begin to contract. It is caused to less extent by slight back flow of blood into the atria at the onset of ventricular contraction and mainly by bulging of the AV valves backward toward the atria because of increasing pressure in the ventricles. JVP • The V wave: Occurs toward the end of • ventricular contraction and it results from slow build up of blood in the atria while the AV valves are closed during ventricular contraction. venous pressure falls during inspiration as a result of the increased negative intrathoracic pressure and rises again during expiration. Normal electrocardiogram • As the transmission of the depolarization wave (cardiac impulse) passes through the heart, electrical currents spread into the surrounding tissues and to the surface of the body which can be recorded by E.C.G. • Are merely the recordings of differences in voltage between tow electrodes on the body surface as a function of time. Calibration • A limited amount of information is provided by the • • height of the P,QRS,& T waves, provided the machine is properly calibrated. A standard signal of 1mV should move the stylus vertically 1cm.(2 large squares),& this ‘calibration’ signal should be included with every record. When the machine is properly calibrated, -tall P waves indicated RT atrial hypertrophy. -tall R waves in the Lt ventricular leads indicate Lt.V.H -& tall R waves in the Lt.ventricular leads indicate Lt.V.H.& tall T waves indicate hyperkalaemia. Small complex indicate a pericardial effusion. RECORDING ECG • 1- the patient must lie down & relax. • 2- Connect up the limb leads’making certain that they are applied to the correct limb. • 3- Calibrate the record with the 1ml V signal • 4- Record the six standard leads-3 or 4 complexes are sufficient for each. • 5- Record the six chest leads (V leads). The 12 -lead ECG • E.C.G.interpretation is easy if you remember the directions from which the various leads look at the heart. • Standard ECG uses 9 electrodes which are used to form 12 ‘lead's recording axis. • Six of these recording axis are in the frontal plane,6 in the horizontal plane. The limb leads-frontal planes axes • The most common set of connections is with electrodes connected to both arms & the left leg give 3 limb leads (AVL,AVR,AVF). • Alternate connections(Einthoven’s triangle) produces the 3 limb leads(1,11,111). • The 6 limb leads give electrical views of the heart in the frontal plane. • The six ‘standard 'leads can be through of as looking at the heart in a vertical plane (that is,from the sides or the feet). Thus Standard leads • Leads 1, AVL,V5,V6 look at the Lt.lateral surface of the heart. • Leads 111 & AVF at the inferior surface • Lead AVR looks at the atria. The septal leads, V1 and V2 septal wall of the left ventricle The anterior leads, V3 and V4 anterior wall of the left ventricle Standard Leads • Lead I- horizontal axis + electrode on Lt.arm negative on Rt. • Lead II- axis at 600,+ electrode on Lt.leg, negative on Rt.arm • Lead III-axis at 1200, + electrode on Lt leg, negative on Lt.arm. Chest leads- horizontal plane axes • The V lead (chest leads) is attached to the • chest wall by means of a suction electrode, & recordings are made from 6 position overlying the 4th & 5th rib spaces. The 6 V leads (V1,V2,V3,V4,V5,V6) look at the heart in a horizontal plane from the front & the Lt side. Thus: • Leads V1 & V2 look at the Rt.ventricle • Leads V3 & V4 look at the septum between the ventricles (the anterior wall of the Lt ventricle) • Leads V5 & V6 at the lateral walls of the Lt.V The Shape of the QRS complex in leads I,II,III • The E.C.G. machine is arranged so that when depolarization wave spreads towards a lead the needle moves upwards & when it spreads a way from the lead the needle moves downwards. • The deflection of the QRS complex thus shows the direction in which the wave of depolarization is spreading. NORMAL ECG • The normal E.C.G is composed of a P wave, • a QRS complex and • a T wave. • The QRS complex is often three separated waves the Q wave, the R wave and the S wave. ECG • The P wave is caused by electrical currents generated as the atria depolarize prior to contraction. • QRS complex is caused by current generated when the ventricles depolarize prior to contraction. • The T wave is caused by currents generated as the ventricle recover (repolarize) from the state of depolarization. ECG • The atria repolarize a approximately 0.15 to 0.20 sec after the depolarization wave which is just at the moment that the QRS wave is being recorded in the E.C.G. • The PR interval is the period between the beginning of the atrial depolarization and the beginning of the ventricular depolarization .It is a measure of atrio-ventricular conduction time. ECG • The QT interval is the time from the beginning of the ventricular depolarization to the end of repolarization (about o.41 sec at 50 beats/min in normal male subjects). • The R-R interval is the time between tow successive complexes and is usually used to measure the cardiac cycle length. • The regular heart rat can be measured using R-R interval according to the following equation:- Heart rate= 60/R-R interval (in sec) Type of ECG wave &interval Duration (sec) P wave duration 0.08 QRS duration 0.05-0.10 T wave duration 0.15-o.25 PR interval 0.12-0.20 Q-T interval Heart rate-dependent It is imp to be remembered The normal electrical axis lies between -30º and+ 120º . Right axis deviation is present when the mean electrical axis lies between+ 120º and +180º. as occurs in right ventricular hypertrophy &Rt bundle branch block • Left axis deviation is present when the mean electrical axis lies between -30º and -90ºas occurs in obesity, Left ventricular hypertrophy and left bundle branch block . Systematic approach to read E.C.G 1. Rate 2. Rhythm 3. Axis deviation 4. Presence of ventricular hypertrophy 5. P wave 6. P-R interval 7. Q wave 8. QRS complex 9. S-T segment 10. T wave Heart rate How to calculate heart rate: When the rhythm is regular When the rhythm is irregular Rhythm If the interval between all R waves is equal then it is regular rhythm If the interval between all R waves is unequal then it is irregular rhythm (arrhythmia). There is a normal arrhythmia called sinus arrhythmia which occurs with respiration When the rhythm is regular Heart Rate = 1500 / No. of small squares between two consecutive waves or Heart Rate = 300 / No. of large squares between two consecutive waves NOTE: The above formulas are correct when the paper speed is running at the standard rate of 25 mm/s. All ECG machine run at a standard rate and use paper with standard size sequres.Each large square (5mm) represents 0.2 seconds and one small square represents 0.04 seconds. So there are 5 large squares per second and 300 per minute. Thus the ECG event such as QRS complex occurring once per large squares is occurring at a rate of 300 per minute. ECG graph paper A typical electrocardiograph runs at a paper speed of 25 mm/s, although faster paper speeds are occasionally used. Each small block of ECG paper is 1 mm². At a paper speed of 25 mm/s, one small block of ECG paper translates into 0.04 s (or 40 ms). Five small blocks make up 1 large block, which translates into 0.20 s (or 200 ms). Hence, there are 5 large blocks per second. A diagnostic quality 12 lead ECG is calibrated at 10 mm/mV, so 1 mm translates into 0.1 mV. When the rhythm is irregular Heart rate=number of R-R interval in 30 large squars × 10 Rate If the rate is < 60 beat / min (sinus bradycardia) (or < 50 beats/min during sleep). If the rate is >100 beat / min (sinus tachycardia) Sinus arrhythmia Heart Rate increases during inspiration And Heart Rate decreases during expiration The above is normal and is called sinus arrhythmia "sinus” from (SA node) and arrhythmia (irregular rhythm)". Axis deviation The normal range for the cardiac axis is between - 30° and 90°. An axis lying beyond - 30° is termed left axis deviation, whereas an axis > 90° is termed right axis deviation. Cardiac out put (C.O) • Is the volume of blood pumped by each ventricle per minute. • This stroke volume (SV) is the volume of blood pumped by each ventricle /beat. • Therefore:• C.O = Stroke volume χ Heart rate = 70 χ 70=4900 ml/min. STROKE VOLUME • By the time diastole ends each ventricle has filled by • • • • bl. This amount of bl.is the EDV. The amount of bl.ejecte during systole is stroke volume at the end of systole the volume of bl.remaining in each ventricle is ESV. For example:each ventricle normally contain a bout 120ml of bl. By the end of diastole. By end of systole about 50mll of bl. This mean about 70ml/beat is pump out by each ventrical during systole. • The key factor • regulating s.v is the amount of stretching that occur to ventricular cardiac m.prior to the v.contraction. The more cardiac stretching the more forcefully to contract these contraction increase s.v Reynolds increased • Decreased bl.viscosity(ex.decrease Hct,anemia) • Increased bl.velocity (ex.narrawing of avessel). Measuring of Bl.pressure • Methods of measuring blood pressure: • Blood pressure can be recorded direct by using mercury manometer with electronic pressure transducers or indirect by mercury sphygmomanometer (palpatory and auscultatory methods) [refere to the practical Manual]. •Palpatory method: Feel the radial pulse of the subject by placing the three middle fingers on the radial artery against the radius bone with mild pressure of the distal finger, you can feel the radial pulse by index finger. Raise the pressure in the cuff to 200 mm Hg. Start to lower the pressure slowly while you are feeling the radial pulse. Once you feel the pulsation of the radial artery, record the reading on the manometer. This reading gives you the systolic pressure. Repeat this procedure many times and record your result. •Auscultatory method: From your surface anatomy knowledge of the antecubital fossa, put the diaphragm of the stethoscope at the position of the brachial artery just below the lower edge of the cuff (not underneath the cuff !). Raise the pressure to 200 mm Hg, then lower the pressure slowly and steadily Phase measure Bl.pressure The following phases of the character of the sound (Korotkow or Korotkoff sounds) will be heard by the stethoscope: Phase 1: If the pressure is above systolic no sound can be heard. When the systolic pressure is reached a clear loud sound is heard with each heart beat. Phase 2: When you lower the pressure more the sound becomes softer. Phase 3: As the pressure is lowered, the sound becomes louder and banging in character. Phase 4: The sound will disapper completely (sometimes this taken as the diastolic pressure). The exact cause of Korotkoff sounds is still debated but they are believed to be caused mainly by blood jetting through the partly occluded vessel. The jet causes turbulence in the open vessel beyond the cuff, and this sets up the vibrations heard throug the stethoscope Regulation of arterial blood pressure • There are tow main mechanisms for regulation • of BP and these are: [A] Rapidly acting mechanism (short – term regulation • [B] Slow acting mechanism (long-term regulation) Rapidly acting mechanism which are rapid to begin acting, they begin to act within seconds and become fully active within a minute or so, and lose their capability for pressure control after few hours or a few days (adaptating mechanisms). • Rapidly acting mechanism • These mechanisms include: • (1) Nervous pressure control mechanisms which include: • [I] The baroreceptors feedback mechanism, • [II] The central nervous system ischemic mechanism, [III] The chemoreceptor • mechanism. • • (2) Other pressure control mechanisms which • • • begin to react within minutes and become fully active within 30 minutes to several hours and include: [I] The hormonal mechanism which include norepinephrine epinephrine,vasopressin,and renin-angiotensin vasoconstrictor mechanisms. [II] Stress relaxation mechanism, [III] Capillary fluid shift. B] Slow acting mechanism (long-term regulation) , which are slow to begin acting and • control the arterial BP over a period of days,weeks, months, and years.Their effectuveness becomes steadily greater with time (non adapting mechanisms), and able to bring the pressure all the way back to normal.These mechanisms include the renal-body fliud –pressure control mechanisms. [A] Rapidly acting mechanism (Shortterm regulation): • The barorecepttors feedback mechanism: This reflex is mediated by baroreceptors located in the carotid sinus at the bifurcation of the common carotid arteries, and their afferent nerve fibers pass to the glossopharyngeal nerves, and baroreceptors which are located along the arch of the aorta, and their afferent nerve fibers pass through the vagi. Increase in Bl.pressure • A rise in pressure stretches the baroreceptors and causes them to transmit signals into the nucleus of tractus solitarius which is the sensory termination of both the vagal and glossopharyngeal nerves at central nervous system. • From this nucleus an inhibitory signals pass to vasoconstrictor area of the VMC and an excitotry signals pass to the vagal (parasympathetic) center. • The feedback signals are then sent back through autonomic nervous circulation cause vasodilatation (decrease peripheral resistance), a decrease in heart and contractility.All will reduce arterial blood pressure downward toward the normal level. • Sudden decrease in bl.pressure when a person sits or stand after having • been lying down. Immediately upon standing, the arterial pressure in the head and upper part of the body obviously tends to fall, the falling pressure at the baroreceptors elicits • an immediate reflex,resulting in strong sympathetic discharge throughout the body, and this minimizes the decrease in the head and upper body. • sudden decrease in bl.pressure Strong pressure to the neck over the • bhfurcations of the carotid arteries in human being can excite the baroreceptors of the carotid sinus,causing the arterial pressure to fall as much as 20 mm Hg in normal person and even a more marked reduction in BP and even stop the heart completely in older atherosclerotic patients which lead to fainting (carotid sinus syncope). The chemoreceptor mechanism Whenever the arterial pressure falls below critical level, the chemoreceptors become stimulated because of diminished blood flow to the aortic and carotid bodies and therefore diminished availability of O2 and excess CO2 and H+ ions are not removed by the slow flow of blood. The signals from the chemoreceptors are transmitted to VMC to excite it, and this elevate the BP back toward normal level whenever it falls too low.Chemoreceptors mechanism start to operat when the blood pressure falls below 80 mm Hg. • Short-Term Regulation of Rising Blood Pressure When rising Pressure • • Rising blood pressure • • Stretching of arterial walls • • Stimulation of baroreceptors in carotid sinus, aortic arch, and other large • arteries of the neck and thorax • • Increased impulses to the brain • • ٍ So the effect of baroreceptors Increased impulses to brain from • baroreceptors • Increased parasympathetic activity and • decreased sympathetic activity • Reduction of heart rate and increase in • arterial diameter • Lower blood pressure • Page 5. Increased Parasympathetic • Activity Increased Parasympathetic Activity • Effect of Increased Parasympathetic and • Decreased Sympathetic Activity on Heart • and Blood Pressure: • • Increased activity of vagus • (parasympathetic) nerve • • Decreased activity of sympathetic cardiac • nerves • • Reduction of heart rate • • Lower cardiac output • • Lower blood pressure • Decreased Sympathetic Activity Effect of Decreased Sympathetic Activity • on Arteries and Blood Pressure: • Decreased activity of vasomotor fibers • (sympathetic nerve fibers) • Relaxation of vascular smooth muscle • • Increased arterial diameter • • Lower blood pressure • Regulation of Rising Blood Pressure Short-term regulation of Rising Blood Pressure • Rising blood pressure • • Stretching of baroreceptors • • Increased impulses to the brain • • Increased parasympathetic activity • • Decreased sympathetic activity • • Slowing of heart rate • Diameter • Increased arterial pressure • • Reduction of blood pressure • • Short-term Regulation of Falling Blood Pressure Falling blood pressure • • Baroreceptors inhibited • • Decreased impulses to the brain • • Decreased parasympathetic activity, increased sympathetic activity • • Three effects: • 1. Heart: increased heart rate and increased contractility • 2. Vessels: increased vasoconstriction • 3. Adrenal gland: release of epinephrine and norepinephrine which • enhance heart rate, contractility, and vasoconstriction • • Increased blood pressure • Sympathetic Activity on Heart and Blood Pressure Increased activity of sympathetic cardiac • nerves • Decreased activity of vagus • (parasympathetic) nerve • Increased heart rate and contractility • • Higher cardiac output • • Increased blood pressure • Vasomotor Fibers Effect of Increased Sympathetic Activity • on Arteries and Blood Pressure: • Increased activity of vasomotor fibers • (sympathetic nerve fibers) • Constriction of vascular smooth muscle • • Decreased arterial diameter • • Increased blood pressure • Sympathetic Activity on Adrenal Gland and Blood Pressure • Increased sympathetic impulses to • adrenal glands • • Release of epinephrine and • norepinephrine to bloodstream • • Hormones increase heart rate, • contractility and vasoconstriction. • Effect is slower-acting and more • prolonged than nervous system control. • Increased blood pressure • • Regulation of Falling Blood Pressur Regulation of Falling Blood Pressure • • Falling blood pressure • • Baroreceptors inhibited • • Decreased impulses to the brain • • Decreased parasympathetic activity • • Increased sympathetic activity • • Increased heart rate and contractility • • Increased vasoconstriction • • Release of epinephrine and • norepinephrine from adrenal gland • • Increased blood pressure • Hormonal mechanisms: Hormonal mechanisms: Hormonal • regulation of the circulation means regulation of tissue blood flow by substances in the body fluids, such as by hormones, ions, or so forth. Among the most important of the humoral factors that affect circulatory function are the following: Vasocontrictor agents: Nor epinephrine has vasoconstrictor effects in almost all vascular beds of the body, and epinephrine has similar effects except it has a mild vasodilator effects in both skeletal, cardiac muscle and liver. Long-Term Regulation of Low BP • Long-term regulation of blood pressure is primarily • accomplished by altering blood volume. • The loss of blood through hemorrhage, accident, or • donating a pint of blood will lower blood pressure and trigger processes to restore blood volume and • therefore blood pressure back to normal. • Long-term regulatory processes promote the • conservation of body fluids via renal mechanisms and stimulate intake of water to normalize blood volume and blood pressures. • Loss of Blood When there is a loss of blood, blood • pressure and blood volume decrease. So Juxtaglomerular Cells in the kidney • monitor alterations in the blood pressure. If blood pressure falls too low, these specialized cells release the • enzyme renin into the bloodstream. Renin-Angiotensin Mechanism: Step 1 The renin/angiotensin mechanism consists • of a series of steps aimed at increasing blood volume and blood pressure. • Step 1: Step 1: Catalyzing Formation of • Angiotensin I: As renin travels through the bloodstream, it binds to an inactive plasma protein, • angiotensinogen, activating it into angiotensin I. Step 2: Step 2: Conversion of Angiotensin I • to Angiotensin II: As angiotensin I passes through the lung capillaries, an enzyme in the lungs • converts angiotensin I to angiotensin II. Step 2: Step 3: Angiotensin II in the Bloodstream Step 3: Angiotensin II Stimulates • Aldosterone Release: Angiotensin II continues through the Blood stream until it reaches the • adrenal gland. Release of Aldosterone Step 3: Angiotensin II Stimulates Aldosterone Release: Here it stimulates the cells of the adrenal cortex to release the hormone aldosterone • Release of Aldosterone Angiotensin II as a Vasoconstrictor • • A secondary effect is that angiotensin II • is a vasoconstrictor and therefore raises blood pressure in the body's arterioles. • Aldosterone Mechanism . Aldosterone Mechanism • • Long-Term Regulation: Aldosterone • Mechanism: The target organ for aldosterone is the kidney. Here aldosterone promotes increased • reabsorption of sodium from the kidney tubules. • Long-Term Regulation: Aldosterone Mechanism: Distal Convoluted Tubule • • Each distal convoluted tubule winds • through the kidney and eventually empties its contents into a urine-collecting duct. • • The peritubular capillaries absorb solutes • and water from the tubule cells as these reclaimed from the filtratesubstances Distal Convoluted Tubule Long-Term Regulation: Aldosterone Mechanism Sodium Reabsorption • • Aldosterone stimulates the cells of the • distal convoluted tubule to increase the active transport of sodium ions out of the tubule into the • interstitial fluid, accelerating sodium reabsorption. Long-Term Regulation: Aldosterone Mechanism Long-Term Regulation: Aldosterone Mechanism Water Reabsorption • • As sodium moves into the bloodstream, • water follows. The reabsorbed water increases the blood volume and therefore the blood pressure. • Long-Term Regulation: Aldosterone Mechanism Increase in Osmolarity Increase in Osmolarity • • Dehydration due to sweating, diarrhea, or excessive • urine flow will cause an increase in osmolarity of the blood and a decrease in blood volume and blood • pressure. Long-Term Effect of Osmolarity on BP • • As increased osmolarity is detected there is both a • short and long-term effect. For the long-term effect, the hypothalamus sends a signal to the posterior • pituitary to release antidiuretic hormone Antidiuretic Hormone Antidiuretic Hormone • • ADH increases water reabsorption in the kidney. • ADH in Distal Convoluted Tubule • • ADH promotes the reabsorption of water from the • kidney by stimulating an increase in the number of water channels in the distal convoluted tubules and • collecting tubules (ducts). • These channels aid in the movement of water back • into the capillaries, decreasing the osmolarity of the blood volume and therefore blood pressure. Short-Term Effect of Osmolarity on BP • A short-term effect of increased • osmolarity is the excitation of the thirst center in the hypothalamus. The thirst center stimulates • the individual to drink more water and thus rehydrate the blood and extracellular fluid, • restoring blood volume and therefore blood pressure. Summary In the short-term, rising blood pressure • stimulates increased parasympathetic activity, which leads to reduced heart rate, vasodilation and lower • blood pressure. • Falling blood pressure stimulates increased • sympathetic activity, which leads to increased heart rate, contractility, vasoconstriction, and blood • pressure. • Summary • Long-term blood pressure regulation involves • renal regulation of blood volume via the reninangiotensin mechanism and aldosterone mechanism. • • Increased blood osmolarity stimulates release of antidiuretic hormone (ADH), which promotes reabsorption of water, and excites the thirst • center, resulting in increased blood volume and blood •






















































































































































































































![Cardio Review 4 Quince [CAPT],Joan,Juliet](http://s1.studyres.com/store/data/008476689_1-582bb2f244943679cde904e2d5670e20-150x150.png)
