Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Brain (1996), 119, 1183-1198
Throwing while looking through prisms
I. Focal olivocerebellar lesions impair adaptation
T. A. Martin,1 J. G. Keating,1 H. P. Goodkin,1 A. J. Bastian2 and W. T. Thach1'3'4
department of Anatomy and Neurobiology, 2The Program
in Physical Therapy, ^Department of Neurology and
Neurological Surgery, and 4The Irene Walter Johnson
Institute of Rehabilitation Research, Washington University
School of Medicine, St Louis, USA
Correspondence to: W. T. Thach, MD, Department of
Anatomy and Neurobiology, Washington University School
of Medicine, 660 S. Euclid Avenue, Box 8108, St Louis,
MO 63110, USA
Summary
Normal human subjects and patients with lesions of the
olivocerebellar system threw balls of clay at a visual target
while wearing wedge prism spectacles. Normal subjects
initially threw in the direction of prism-bent gaze, but with
repeated throws adapted to hit the target. Patients with
generalized cerebellar atrophy, inferior olive hypertrophy, or
focal infarcts in the distribution of the posterior inferior
cerebellar artery, in the ipsilateral inferior peduncle, in the
contralateral basalpons or in the ipsilateral middle cerebellar
peduncle had impaired or absent prism adaptation. Patients
with infarcts in the distribution of the posterior inferior
cerebellar artery usually had impaired or absent adaptation
but little or no ataxia. By contrast, patients with damage in
the distribution of the superior cerebellar artery or in
cerebellar thalamus usually had ataxia but preserved
adaptation. These results implicate climbing fibres from
the contralateral inferior olive via the ipsilateral inferior
cerebellar peduncle, mossy fibres from the contralateral
pontocerebellar nuclei via the ipsilateral middle cerebellar
peduncle, and posterior inferior cerebellar artery territory
cortex as being critical for this adaptation. The
dentatothalamic projection and the superior cerebellar artery
territory cortex are not necessary for this adaptation.
Keywords: throwing; cerebellum; prism; motor adaptation
Abbreviations: AC = adaptation coefficient; PC = performance coefficient; PICA = posterior inferior cerebellar artery;
SCA = superior cerebellar artery
Introduction
When attempting to hit a target with a thrown object, humans
usually foveate the target and then throw in the direction of
gaze (Vickers, 1994). The relationship between the directions
of gaze and arm movement is adjustable, as has been
demonstrated using the paradigm of adaptation to wedge
prisms in pointing and throwing movements (Held and Hein,
1958; Harris, 1963; Kohler, 1964; Kane and Thach, 1989).
Wedge prisms bend the light path and, when worn as
spectacles with the bases to one side, require gaze to shift
to the opposite side along the bent light path to fixate the
target. The initial throw in the direction of gaze thus misses
the target to the side by an amount proportionate to the
diopter of the prism. The subject sees the impact as laterally
displaced. With continued throws aimed at the perceived
target the subject gradually increases the angle between the
direction of gaze and the direction of throw so that the object
lands on target. When the prisms are removed, gaze is now
© Oxford University Press 1996
on target, but the widened angle between the direction of
gaze and the direction of throw persists: the object misses
the target to the opposite side by an amount almost equal to
the initial prism-induced error. This error has been called the
'negative after-effect' (e.g. Weiner et ai, 1983). Like the
initial error, the after-effect error gradually diminishes with
repeated throwing as the direction of throwing shifts back to
the direction of gaze.
Prior reports stated that the cerebellum is involved in
adaptation to wedge prisms in an arm pointing task (Baizer
and Glickstein, 1974; Weiner et al., 1983). We have further
studied patients with damage of the cerebellum or its inputs
or outputs during prism adaptation of throwing to localize
the parts of the olivocerebellar system that are necessary for
adaptation of this form of eye-hand coordination. Portions
of this work have been presented previously in brief (Kane and
Thach, 1989; Thach et al., 1991, 1992; Martin et al... 1995).
1184
T. A. Martin et al.
Methods
Subjects
Control subjects were healthy, unpaid, adult volunteers with
no history of neurological injury and were naive to the
purpose of the experiments. We recorded data from 15
subjects (mean age±l SD of 50.0± 16.6 years; range 22-70
years) as controls for the patients in the basic prism adaptation
paradigm.
Our 27 patients with neurological deficits had an average
age of 55.2± 16.8 years (range 21-82 years) and were seen
in the hospital and out-patient departments of neurological
and neurorehabilitation services or by referral from local
hospitals. All subjects were informed of the procedure, which
had been approved by the Human Studies Committee of
Washington University School of Medicine, and they gave
informed consent prior to the experiments in accord with the
declaration of Helsinki.
Patients with clinical diagnoses of cerebellar disorders
were selected and divided into three main groups (see Table
2 below): (i) damage of cerebellar cortex and/or nuclei
(n = 12), (ii) cerebellar input pathways (mossy or climbing
fibre) (n = 10); (iii) cerebellar output pathways at the level
of the thalamus (n = 3). Patients with signs of corticospinal
or somaesthetic pathway involvement were excluded. In
addition, we studied two subjects with palatal myoclonus
without inferior olive hypertrophy or additional neurological
deficits. Lesion locations were determined in 25 out of 27
patients by a radiologist using MRI or CT scans (see Table 2).
The task: prism adaptation of throwing
Two kinds of prisms were used in the experiments involving
patients with neurological deficits. Subjects viewed the target
either monocularly through a Risley prism set to 30 diopters
(-17°) with the other eye patched or binocularly (see Fig.
1A) through 30 diopter, Fresnel 3M Press-on plastic lenses
(3M Health Care, Specialties Division, St Paul, Minn., USA).
There was no apparent difference between subjects adapting
with monocular Risley versus binocular Fresnel lenses, and
we have therefore combined these data.
Subjects threw clay balls at a target (a 8X8 cm2 square
drawn on a large sheet of parcel paper) centred at shoulder
level 2 m in front of them. Subjects stood, except when
postural instability required sitting. The subject's head was
unrestrained, and no directions were given about trunk,
shoulder, or head/neck posture. A baseline throwing
performance was obtained by having the subjects throw balls
at the target before they donned prisms. The position at
which the balls made an impact around or on the target was
marked immediately after each throw (Fig. IB, black circles).
After donning prisms, the subjects were instructed to throw
with the same arm 'where you see the target,' and the results
were marked as described above (Fig.IB, empty circles).
After removing the prisms the subjects threw again with
the same arm (Fig. IB, shaded circles). Subjects had an
unobstructed view of the target during the entire session, but
were instructed not to look down at their hands as they were
handed the balls or during the throws. The locations of the
impacts were then plotted sequentially by trial number
(abscissa) versus horizontal displacement (in centimetres)
from a vertical line passing through the target centre (ordinate)
with impacts to the left of the target plotted as negative
values and those to the right as positive values (Fig. 1C).
The adaptive process was modelled by fitting an exponential
decay curve to the data (Fig. 1C).
Dissociation of performance and adaptation
The subject's capacity for motor adjustment was distinguished
from the precision of motor performance in the following
manner. During the pre-prism control period, the scatter of
the impacts around the mean baseline reflected how
consistently and well the subject could throw. In all cases,
the horizontal errors (distance from each impact location to
a vertical line passing through the target) of the subject's last
eight throws before donning prisms served as the baseline
performance. The standard deviation of these errors (in
centimetres) was called the performance coefficient (PC).
A mathematical model of each subject's adaptation data
was used to estimate the rate of adaptation. During normal
adaptation, the impact locations were plotted against the trial
number and were fitted with an exponential decay function.
The rate of change of slope of the exponential decay curve
was taken as a measure of the rate of adaptation (Keating
and Thach, 1990). This rate constant was called the adaptation
coefficient (AC). It is the number of throws taken to get to
a point (1-e"1) or ~63.2% of the way through the adaptation.
All curve fits were generated using CoStat software
(CoHort Software; Berkeley, Calif., USA) and Fourier
(periodic) curve fitting and were fit to the regression equation:
y = a-b
X z-"c
where a is the final value that the exponential decay function
approaches, b is the magnitude of the adaptation required
from the first throw to the value a, c (the decay constant)
represents the rate at which adaptation takes place (AC) and
t is the trial number. This method gave objective, independent
and quantitative measures of adaptation and performance. A
large PC value relative to control indicated impaired performance values, while a large AC value indicated impaired
adaptation.
Criteria for normal and abnormal performance
and adaptation
The PC and AC values for controls and patients and the
presence or absence of a significant after-effect were used
as criteria to differentiate between normal and abnormal
performance and adaptation. As an objective criterion for
normal performance, we arbitrarily selected a cut-off PC
value equal to the mean of the controls' PC values plus two
standard deviations. Any patient whose PC value was larger
Eye-hand coordination and the cerebellum
1185
100
PC = 3.2
AC = 5.0
AC = 8.9
o
UJ
50
2
UJ
FIRST THROW
AFTER PRISMS
FIRST THROW
WITH PRISMS
o
0.
CO
Q
o
o -50
N
DC
O
I
-100
BEFORE
PRISMS
TIME
— -3.9 + -39.0*e (x/5 0)
-25cm
AFTER
—
5.4 + 29.0*e ( - x/89)
L
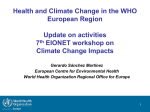
Fig. 1 Prism adaptation test, control subject. (A) Eye-hand positions after adaptation to base-right prisms. The light path is bent to the
subject's right, giving a fuller view of the right side of her face. Her gaze is shifted left along the bent light path to foveate the target in
front of her. Her hand position is ready for a throw at the target in front of her. (B) Normal results of the throwing test of prism
adaptation for a control subject (control subject no. 8, Table 1). Target centre is at the origin of the graph. Impact locations are shown
before donning the prisms (black circles), while wearing 30 diopter base right prisms (empty circles), and after removing the prisms
(shaded circles). First throws during and after prism exposure are marked. The ordinate has been expanded to show the data more
clearly. (C) Horizontal locations of the above impacts displayed sequentially by trial number. Deviations to the left are negative values;
deviations to the right, positive. With the prisms (eyes now looking to the left), the first impact is displaced 60 cm left of centre.
Thereafter, impact points move towards the target (0). After removal of the prisms, the first impact is 50 cm right of centre. Thereafter,
impact points again move towards the target. Data during and after prism use have been fit with exponential curves. The decay constant
is a measure of the rate of adaptation (adaptation coefficient = AC). The standard deviation of the last eight baseline throws is a
measure of performance (performance coefficient = PC).
than this value was determined to have shown impaired
performance.
One objective criterion for adaptation was the presence of
a significant after-effect. Control and patient data for the
adaptation paradigm were analysed with a Mann-Whitney U
test (special tables for small n; Darlington, 1975). The last
eight throws before donning the prisms were used as a
measure of baseline performance. A negative after-effect was
the criterion that adaptation had occurred (Helmholtz, 1867;
Wiener el ai, 1983; Kane and Thach, 1989). To detect a
negative after-effect, we compared the first three throws after
removing the prisms with the pre-prism baseline throwing.
The signed post-prism horizontal deviation was used in all
calculations of the statistic, and the null hypothesis of no
negative after-effect was tested at the P = 0.05 level for a
shift in throwing direction. All adaptive shifts that were
statistically significant were in the predicted direction of the
negative after-effect and are hereafter called 'significant
after-effect.'
For controls and patients with a significant after-effect, the
rates of adaptation were measured and compared. We used
the value equivalent to the mean plus two standard deviations
of the control subjects' AC values during prism adaptation
as a cut-off value. Any patient whose AC value during prism
adaptation was larger than this value was determined to have
shown a slowed adaptation.
Results
Prism adaptation of the gaze-throw angle
Data from control subject no. 8 {see Table 1 below) are
shown in Fig. 1(B and C). During baseline throws, the object
1186
T. A. Martin et al.
Table 1 Prism performance
and adaptation results for control subjects
Control
Sex
Age
(years)
Baseline
(cm±SD)
During (cm)
Adapted (cm)
After (cm)
AC (throws)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
M
M
M
F
M
M
F
F
F
M
F
M
M
M
F
70
43
38
63
70
45
43
57
70
53
60
22
24
63
29
1.3+3.9
2.3±4.6
-0.8±4.4
-1.1±6.1
0.5±3.6
-1.2+3.4
3.1 ±7.2
2.8±3.2
3.4±6.9
1.8+10.3
-1.0+8.7
3.1 it 12.6
8.4±10.9
-1.1+5.4
0.3±11.6
-47.3
-50.2
-47.0
-70.8
-38.5
-42.0
-19.3
-39.5
-30.3
-40.5
-23.3
-65.7
-42.3
-49.7
-51.7
-3.5
-10.7
1.3
-1.8
-2.8
0.7
5.7
-6.3
4.7
-13.0
-7.7
-3.2
-9.8
0.3
-16.3
30.0
16.8
41.0
36.0
18.3
40.0
67.7
31.7
19.2
24.5
19.2
31.5
48.5
52.2
22.7
6.4
4.5
16.9
10.4
13.4
5.6
16.8
5.0
6.5
2.5
5.6
11.1
7.8
12.4
2.4
Mean control PC (mean baseline SD) = 6.9±3.2 cm
Mean control AC = 8.5 ±4.8 throws
Measures of the throwing are: baseline = average horizontal location (± 1 SD) of the last eight impacts before donning the prisms [the
performance coefficient (PC) is the SD]; during = average of first three impacts upon donning the prisms; adapted = average of the last
three impacts with the prisms still on; after = average of the first three impacts upon first removing the prisms (negative after-effect);
adaptation coefficient (AC) = the time constant of an exponential decay function fitted to the horizontal displacement data of the
subject's throws during adaptation to prisms (serves as a measure of the rate of adaptation).
hit near the centre of the target. The trial-to-trial scatter
varied with the throwing skill of the individual. When the
subject first donned the prisms, she threw in the same
direction as gaze and hit to the left of the actual target. With
repeated throws there was a gradual shift in location of
the impacts away from the direction of gaze and toward the
actual target location. For each control subject this shift
followed a stereotyped curve.
When the prisms were removed the subject threw to the
opposite side of the target with an error of almost the same
magnitude as the initial prism throw (the 'negative aftereffect'; Fig. 1C). Repeated throws followed a curve that was
roughly the inverse of the adaptation curve. This observation
was consistent across control subjects. The adaptation curve
was well fitted by a simple exponential decay function. For
the curves in Fig. 1C, the AC values are 5.0 throws for the
adaptation and 8.9 throws for the significant after-effect (see
equations in Fig. 1C). This subject had a PC value of 3.2 cm.
Table 1 gives quantitative data on the prism adaptation of
the 15 control subjects in the basic prism adaptation paradigm.
Their averaged AC was 8.5±4.8 throws (range 2.4—16.9
throws). The residuals of the curve-fits for each subject were
normally distributed, indicating validity of the curve fitting
procedure. The averaged PC was 6.9±3.2 cm (range 3.212.6 cm). There was no correlation between the AC and PC
values (r = - 0 . 2 1 ; P = 0.45 for r = 0). The cut-off value
for performance impairment was 13.3 cm (see Methods).
The cut-off value for slowed versus normal rates of adaptation
was 18.1 throws (see Methods).
Effect of neural lesions on adaptation and
performance
Patients are identified by their initials throughout this paper
(see Table 2 for details).
Diffuse cortical disease
Two subjects with advanced pan cerebellar cortical lesions
showed deficits in adaptation. Patient DE showed no
significant after-effect with the right arm. There was a
significant after-effect with the left arm but the throws were
too variable to be fitted with an exponential decay function.
Patient DJ had action tremor, overshoots and decomposition
of reaching movements and impaired precision pinch. This
patient passed no criteria for adaptation (there was no
significant after-effect) or for adequate performance (left
hand PC = 17.5 cm).
Posterior inferior cerebellar artery (PICA)
territory infarcts
Five patients with cerebellar infarcts in the distribution of
the PICA who had no lasting brainstem signs had slow or
no adaptation. Patient WF (Fig. 2A and B) had a right-sided
(and to a lesser extent, left-sided) PICA territory infarct
resulting in skewed gaze, mild right-sided gait ataxia (walked
without assistance), right-sided reach overshoot and clumsy
hand movements. Yet this patient could throw close to the
Eye-hand coordination and the cerebellum
1187
B 100
u
z 50
HI
N-50
o
PATIENT WF (RIGHT SIDE)
-100
PATIENT WF (LEFT SIDE)
D 100
E
u
50
LU
o
%o
o
§-50
tr
O
-100
PATIENT CK (RIGHT SIDE)
-100
PATIENT TL (RIGHT SIDE)
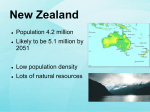
Fig. 2 Absent or diminished prism adaptation in two patients with PICA territory cerebellar infarcts and preserved adaptation in another
despite ataxia with a posterior vermal lesion. Bilaterally impaired adaptation in patient WF with bilateral PICA territory infarcts throwing
with right (A) and left (B) arms. (C) Slowed adaptation in patient CK with a right PICA infarct (AC = 23.6 throws). (D) Presence of
adaptation and a significant negative after-effect despite ataxic performance in patient TL with surgical midline splitting of the posterior
vermis. Line drawings of lesions are based on MRI/CT scans.
centre of the target with the right hand (Fig. 2A). Wearing
base-right prisms, the patient's gaze and right-hand throws
were to the left, without adaptation. However, upon removal
of the prisms the patient showed a significant after-effect
with throws more rightwardly displaced than the control
throws. But this after-effect was different from that seen
during prism adaptation in control subjects. Repeated throws
showed no trend back toward the centre of the target. Lefthand throws showed no significant after-effect (Fig. 2B). A
parasagittal right-sided MRI brain scan of this patient (Fig.
3 A) showed a PICA territory infarct of the inferior cerebellum.
Patient CK (Fig. 2C) had a right PICA territory cerebellar
infarct that also involved the inferior cerebellar peduncle.
On initial examination he had ataxia of the right leg in gait
with frequent falls to the right. There was no dysmetria on
reaching or clumsiness in the subject's hand movements.
However, the subject could not perform the 'sleights of hand'
he had practiced for years (fancy card shuffling; tracking a
single card during shuffling; flipping coins on hand, wrist
and elbow into the air and catching all three in the same
hand). His adaptation was slowed, as indicated by a larger
than normal AC of 23.6 throws. A horizontal MRI brain
scan (Fig. 3B) showed a PICA territory infarct involving the
posterior cerebellum. In addition, the scan showed
88
T. A. Martin et
Table 2 Prism performance and adaptation results for patients
Patient
Age
Sex
Lesion
Scan
(years)
Corticonuclcar
Diffuse cortical
DE** 56
DJ * 22
PICA distribution
WF
61
CK
44
JR
77
JM
49
LL
60
Vermal distribution
44
RLI
T L **
15
SCA distribution
LFI
60
WD
71
FT** 47
Input
Climbing
DH
RL2
MM
VB
LW
fibre
68
48
45
63
75
Baseline
(cm+SD)
F
F
OPCA
Cerebellar cortical atrophy
MRI
MRI
M
M
M
M
MRI
CT
MRI
MRI
F
R and L PICA infarct
R PICA inlaid
L PICA infarct
R and L Vert.Art.Occl.; R PICA
infarct; Sup. vermal infarct
R Post. inf. cerebellar infarct
CT
-
M
F
Tumor removal
Tumor removal
MRI
MRI
-
M
M
M
R SCA infarct
L SCA infarct; old R PICA infarct
R Cerebellar haemorrhage with evac.
CT
CT
MRI
F
M
M
M
F
PM
PM
PM
PM
PM
MRI
MRI
MRI
MRI
_
with IOH
with IOH
with IOH
with IOH
after stroke
Right arm
Left arm
During
(cm)
-0.6±9.2
_
Adapted
(cm)
-2.2
1.3
_
_
-42.8
-15.3
-23.2
-55.5
2.7
5.2
_
-
-24.7
_
-
1.0±5.l
-4.5+12.6
3.9+14.9
-38.2
-27.5
-33.3
-23.6
-0.8
-3.7
7.017.0
_
_
-33.3
_
-23.7
2.4+8.5
6.1±10.5
-1.4±13.3
-1.7±5.8
_
After
(cm)
21.7
_
**
_
Baseline
(cm + SD)
4.6+12.2
12.5117.5
During
(cm)
Adapted
(cm)
After
(cm)
AC
(throws)
-11.0
-8.7
-8.3
-9.5
8.5
-2.5
*
**
23.6
2.6
53.7
_
3.217.9
-0.314.3
-1.417.7
5.4+4.3
-50.7
-35.2
-27.7
-34.8
-61.7
-20.7
-12.0
1.7
18.0
12.8
12.7
24.0
-
3.914.0
-9.8
-0.8
6.8
_
-
-7.4+9.6
-4.6115.4
-22.3
-25.8
-28.5
-5.3
7.0
32.5
3.7
**
11.2
34.7
23.3
8.1
1.6
**
8.8 + 8.2
-8.5 + 8.7
9.7131.2
-29.3
-35.2
-2.5
-2.6
-8.7
-10.5
26.1
31.3
36.2
8.5
10.5
**
11.015.4
-2.217.4
0.613.5
3.9+3.2
_
-40.8
-37.2
-23.3
-38.7
_
-5.8
-28.2
-21.3
-19.2
25.0
_
_
23.5
2.5
11.0
32.7
_
23.4
27.9
59.1
_
-0.7
4.3
4.7
_
1.2
-8.3
AC
(throws)
-
_
-
Mossy tibrc—pontine involvemcnt-'alaxic hemiparcsis'
LF2
82
F
L Ataxic hcmiparesis
NF
73
M
L Pontine infarct
GS
65
M
R Pontine infarct
Mossy fibre-peduncular involvement
RN
58
M
R Middle peduncle infarct
DS *
74
F
L Middle+Inf. peduncle infarct
Output
Cerebellar
LE
JJ *
DW
thulumus
50
M
55
M
57
F
Other
MA
RS
21
51
M
M
-
CT
CT
MRI
CT
L Cerebellar thulumus lacune
L Cerebellar thulumus infarct
R Cerebellar thulumus infarct and
R Red nucleus infarct
MRI
MRI
MRI
PM without 1OH
PM without 1OH
MRI
MRI
-7.2±11.0
-6.9+16.3
12.7 ±6.3
-55.8
-29.0
-14.5
-30.1
-2.7
6.2
-6.8
22.2
24.8
—
5.6
-
-4.3+5.5
7.9±9.7
-1.1+3.2
-20.2
-20.3
-30.3
3.3±11.3
O.2±23.5
-32.7
-43.5
-2.0
34.2
12.3
19.7
-1.7
-4.5
20.3
11.5
4.2'
-2.6+6.1
0.0±17.6
-32.0
-29.0
-21.3
-11.7
19.3
42.0
42.4
l.3±8.2
6.4+20.8
-49.8
-60.3
-3.2
-19.7
44.2
3.7
4.4
0.6±10.0
2.2±5.4
-63.0
-36.7
-17.7
-17.0
28.0
14.0
2.7
10.0
*
-
-
-
-21.3±I7.5
9.2±I4.2
-68.3
-28.3
-44.8
-24.0
28.8
35.8
10.8
-42.3
-6.3
25.7
17.8
2.4+3.9
-
14.3
9.7
-
7.0
4.4
*
Patient lesions organized by area of lesion and by general structure involved. In addition to confirmation of the lesions by imaging techniques {see Scan) all subjects presented
with clinical findings consistent with their lesions. Throwing data are listed for each subject, depending on the arm used to throw. When time permitted subjects were tested
bilaterally. The data (Baseline. During, Adapted, After and AC) are calculated as described for Table 1. Bold numerals under 'Left arm' or 'Right arm' indicate that the subject did
not have a statistically significant after-effect when throwing with that arm. T h o s e patients who had exceedingly poor performance, showing a high degree of variability in their
baseline throwing accuracy and no significant after-effect {see Methods). **Subjects with significant after-effects but impaired or variable performance as follows: Subjects DE, TL
and FT showed significant after-effects but such large variability in their performance that the throws could not be fitted with an exponential curve. Subject W F showed a
small significant after-effect but no noticeable adaptation while wearing prisms; the throws could not be fitted with an exponential curve. AC = adaptation coefficient;
evac. = evacuation; Inf. = inferior; IOH = inferior olive hypertrophy; L = left side; occl. = occlusion; OPCA = olivo-ponto-cerebellar atrophy; PM = palatal myoclonus;
post. = posterior: R = right side; Sup = superior; vert. art. = vertebral artery.
s
s.
I
I
a
a
S.
8
TO
OO
V©
1190
T. A. Martin et al.
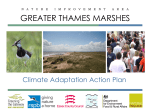
Fig. 3 Magnetic resonance images of four patients with lesions of the olivocerebellar system. (A) Patient WF had a right-sided (and to a
lesser extent, left-sided) PICA territory infarct. (B) Patient CK had a right PICA territory infarct involving the inferior cerebellar
peduncle. (C) Patient TL had a lesion of the vermis, with surgical midline splitting of the posterior vermis (lobules VI-X) through to the
fourth ventricle to remove an ependymoma. (D) Patient MM had palatal myoclonus with inferior olive hypertrophy.
involvement of the inferior cerebellar peduncle (see inset).
No other patient with a PICA territory infarct showed
involvement of the inferior cerebellar peduncle.
Three other subjects (JR, JM, LL) with infarcts in the
PICA distribution showed impaired or no adaptation when
throwing with the arm ipsilateral to the lesion. Patient JR
had a left PICA distribution infarct, initially presenting with
adduction of the ipsilateral leg with falling to that side,
overshoot on reaching, clumsy hand movements and a
transient right extensor plantar response. There was no
Fig. 4 Absent or diminished prism adaptation in patients with palatal myoclonus and inferior olive hypertrophy (A-C) or with (E and F)
ataxic hemiparesis: A, patient RL2 showed no prism adaptation; B, patient DH had slow prism adaptation (AC = 23.4 throws);
C, patient MM had slow prism adaptation (AC = 27.9 throws). D: patient RS with palatal myoclonus but without inferior olive
hypertrophy had significant after-effect and a normal rate of adaptation (AC = 10.0 throws). Patient LF2 had left-sided ataxic
hemiparesis; significant after-effect was absent for the left arm (E) but present for the right (F). Line drawings of inferior olive lesions
are included for those subjects who had known or suspected inferior olivary damage.
Eye-hand coordination and the cerebellum
-100
-100
PATIENT RL2 (RIGHT SIDE)
1191
PATIENT DH (RIGHT SIDE)
D 100
100
o
5 50
50
111
1
O.
A
eo
D
U
a.
n
a
_l
1
1-50
-100
§ -50
en
O
PATIENT MM (RIGHT SIDE)
-100
PATIENT RS (RIGHT SIDE)
PATIENT LF2 (LER SIDE)
-100
PATIENT LF2 (RIGHT SIDE)
§ -50
-100
1192
T. A. Martin et al.
significant after-effect on the left. He had normal adaptation
on the right (AC = 2.6 throws and a significant after-effect).
Patient JM had bilateral vertebral artery occlusions with old
small infarcts of the superior vermis and a more recent large
right PICA distribution infarct. He presented with sustained
nystagmus on right lateral gaze, decreased hearing on the
right, a transient right extensor plantar response, and an
inability to stand. The brainstem and corticospinal tract signs
subsequently cleared. There was a markedly slow adaptation
with the right arm (AC = 53.7 throws). Patient LL had a
small infarct in the right posterior inferior cerebellum and
showed no significant after-effect with the ipsilateral right
arm. Within months of the PICA distribution infarct(s), all
these patients walked independently and had little or no
ataxia of arm or hand movements.
Patient WD entered the hospital because of a left superior
cerebellar artery (SCA) territory infarct with ataxia of the
left arm and leg (see below). A CT scan at that time revealed
an older and apparently silent large PICA territory infarct on
the right side. This subject had no ataxia on the right and
was the only one with a PICA distribution infarct to show
normal prism adaptation of throwing with the ipsilateral arm.
effect. The second patient (DH; Fig. 4B) also had palatal
myoclonus, dysarthria, and ataxia of gait. There was apparent
adaptation after donning the prisms, but at a rate slower than
normally seen in control subjects (AC = 23.4 throws). An
after-effect, though small, was significant. The third patient
(MM; Fig. 4C) had palatal myoclonus, dysarthria,
disequilibrium, and ataxia of gate. Adaptation was slowed
(AC = 27.9 throws), but there was a significant after-effect.
The involvement of the inferior olive can be seen on his
MRI scan (Fig. 3D). The fourth patient (VB) had palatal
myoclonus, dysarthria, and mild ataxia of gate. Adaptation
was very slow (AC = 59.1 throws), but there was a significant
after-effect.
A fifth patient (LW) developed bilateral palatal myoclonus
and right-sided ataxia of arm and leg following a stroke. She
had no neurological deficits in the left extremities and was
tested using the left arm. Adaptation was impaired and there
was no significant after-effect.
In contrast, two patients (RS; Fig. 4D and MA) with
'essential palatal myoclonus' (cf. Deuschl et al., 1994) but
without other neurological impairment and without damage
of the inferior olive as indicated by normal MRI scans had
significant after-effects and AC values in the normal range.
Vermis of cortex
Two of three patients with vermal lesions showed impairment
of adaptation. Patient JM, with the right PICA territory infarct
and slowed adaptation on the right, also had a small old
superior-posterior vermal infarct and no significant aftereffect on left handed throwing. Patient RL1 underwent
removal of a superior vermal tumor. Subsequently, there was
an ataxic wide based gait but normal reach and pinch. There
was no significant after-effect with the left arm. He had
significant after-effect with the right arm and an AC within
the normal range (AC = 3.7 throws). Nevertheless, patient
TL (Fig. 2D) had the largest lesion of the vermis in this
series, with surgical midline splitting of the posterior vermis
(lobules VI-X; Fig. 3C) through to the fourth ventricle to
remove an ependymoma. Three years after the surgery,
throwing with the dominant right hand showed poor
performance (PC = 15.4 cm), and we could not fit her
impact locations with a delay curve to get an AC value.
Nevertheless, the data appeared to show adaptation, and there
was a significant after-effect.
Disease of inferior olive
Four patients with 'symptomatic palatal myoclonus' (cf.
Deuschl et al., 1994), ataxia, and MRI-documented inferior
olive hypertrophy (a degenerative disease of the inferior
olive) showed slow adaptation or no significant after-effect;
results from three are shown in Fig. 4 (A-C). One (RL2;
Fig. 4A) had palatal myoclonus with simultaneous vertical
nystagmus, diaphragmatic and facial contraction, dysarthria,
hoarseness, and ataxia of gait, but with relatively little ataxia
of the upper extremities. There was no significant after-
Ataxic hemiparesis
Patient LF2 (Fig. 4E and F) had a stroke with ataxia without
weakness of the left arm and spastic weakness without ataxia
of the left leg. Throwing with the left arm showed no
significant after-effect (Fig. 4E). Throwing with the right
(unaffected) arm showed adaptation with a normal AC and
significant after-effect (Fig. 4F). Patient NF had a left pontine
infarct and GS a right pontine infarct, each with ataxia of
arm movement and spastic paresis of the leg on the side
opposite the lesion. Adaptation for all three subjects with
ataxic hemiparesis (LF2, NF, GS) was impaired in the arm
contralateral to the lesion (no significant after-effect). All
had normal adaptation (low AC and significant after-effect)
in the arm ipsilateral to the lesion.
Infarcts of cerebellar peduncles
Patients with middle cerebellar peduncular infarcts (RN, DS)
showed slightly different results from those of the ataxic
hemiparetics. Patient RN had an infarct in the right middle
cerebellar peduncle presenting as right maxillary pain, general
weakness, nausea and retching. On examination there was
mid-position nystagmus with slow phase to the right, right
maxillary hypesthesia, ataxia of the right leg in gait with
falling to the right, ataxia of the right arm in reaching with
overshoot but no tremor. On prism testing there was markedly
slowed adaptation (AC = 42.4 throws) on the right, but
significant after-effect bilaterally. Patient DS had a left-sided
infarct involving both the middle and the inferior cerebellar
peduncles, with severe ataxia of gait (falling to the left), and
leg and finger movements. There was no significant after-
Eye-hand coordination and the cerebellum
effect with the left arm. There was impaired performance in
both hands (left hand PC = 23.5 cm; right hand PC =
17.6 cm).
SCA territory infarcts and lateral hemisphere
deep haemorrhage
Cerebellar lesions in the SCA territory produced severely
ataxic limb movements, but did not impair adaptation. Two
subjects had infarcts in the territory of the SCA which
involved cortex in the superior intermediate zone and probably
also the dentate nucleus (Amarenco and Hauw, 1990;
Amarenco, 1991; Kase et al., 1993). Both had severe ataxia
of the ipsilateral limbs in walking, reaching and pinching.
Yet both had AC values in the normal range and significant
after-effects for both arms. Patient LF1 (Fig. 5A and described
in Goodkin et al., 1993) had a right SCA territory infarct
with ataxia of the right hand, arm and leg, with difficulty in
precise finger movements (absent precision pinch, permanent
inability to write), overshoots and decomposition during
reaching movements and frequent falls to the right. Patient
WD (Fig. 5B) had a left SCA territory infarct with ataxia of
the left arm and leg during reaching, pinching and walking.
Patient FT (also described as patient CBL-02 in Bastian
et al., 1996) underwent evacuation of a right-sided deep
cerebellar haemorrhage. Despite severe ataxia of the right
hand, arm and leg in manipulation, reaching, walking and
standing, he retained an ability to adapt in throwing. There
was a significant after-effect with both arms. His adaptation
could not be fit by an exponential curve due to the large
variability of his throws (right hand PC = 31.2 cm; left hand
PC = 14.9 cm). These patients ultimately walked only with
a cane or walker and they had persistent ataxia of the involved
extremities. However, they could adapt to prisms on throwing.
Cerebellar thalamus
Three patients had lesions presumed to involve regions of
the thalamus that receive input from the cerebellum (ventral
lateral nucleus, caudal division; ventral posterolateral nucleus,
oral division; ventral lateral nucleus, pars postrema; nucleus
X; see Asanuma et al., 1983a, b, c). Patient LE (Fig. 5C;
patient T-01 in Bastian and Thach, 1995) had a small infarct
in the left posterior ventrolateral thalamus, with right-sided
action tremor and ataxia of finger movements and action
tremor without ataxia in reaching. Gait was normal, and there
were no sensory impairments. Patient DW had an infarct
involving the right thalamus and red nucleus, with clinical
findings similar to those above except for paresthesiae in the
left arm and leg without objective deficit. Both LE and DW
had normal AC values and significant after-effects.
Patient JJ (Fig. 5D; patient T-02 in Bastian and Thach,
1995) had an infarct in the right posterior ventrolateral
thalamus. As with the above patients, there was action
tremor and ataxia of the left hand and finger movements,
1193
a normal reach except for action tremor, and a normal
sensory examination despite hemiparaesthesiae of numbness
and coldness. This patient passed no criteria either for
adaptation (there was no significant after-effect) or for
adequate performance (left hand PC = 17.5 cm; right hand
PC = 20.8 cm). The patient's throwing performance was
badly ataxic (Fig. 5D).
Summary of all patients
Table 3 shows the results across 29 lesions (27 patients, two
with two lesions each) with respect to both performance and
adaptation. In the upper left quadrant are those six out of 29
lesions causing neither significant impairment of performance
nor that of adaptation. This category includes the two patients
with palatal myoclonus without inferior olive hypertrophy,
and the one patient with an old apparently silent PICA
infarct. Two of the three patients with SCA infarcts and one
of the three with cerebellar thalamic infarcts also met criteria
for normal performance and adaptation, although all three
were clinically ataxic. In the lower right quadrant are those
lesions giving significant impairment of both performance
and adaptation. This category included only three out of 29
lesions: one with diffuse cortical atrophy and one each of
middle plus inferior peduncular and cerebellar thalamic
infarcts. In the lower left quadrant are those three out of 29
lesions giving significant impairment of performance only.
This category includes one out of three lesions of the vermis,
one out of three SCA infarcts, and one out of three cerebellar
thalamic infarcts. In the upper right quadrant are those 17 of
the 29 lesions giving significant impairment of adaptation
only. This is the largest category and includes all five of the
five patients with palatal myoclonus and known or suspected
inferior olive hypertrophy, five out of six of those with PICA
infarcts, all three out of three of those with ataxic hemipareses,
two out of three of those with vermal lesions, and one out
of two of those with middle peduncle lesions.
Of the 23 lesions causing impairment of performance or
adaptation or both, 20 of the lesions (in the lower left
and upper right quadrants) show a significant tendency for
dissociation of impairments of performance and adaptation.
Prominent amongst these are the high proportion of lesions
of the inferior olive, PICA territory cortex, vermis and
brainstem.
Discussion
Independent measures of performance and
adaptation show that they are dissociable
processes
The assessment of motor adaptation after cerebellar lesions
can be confounded by impaired motor performance (Bloedel
and Zuo, 1989; Welsh and Harvey, 1989). These authors
concluded that the apparent role of the cerebellum in coupling
the rabbit's nictitating membrane response to a tone could
1194
T. A. Martin et al.
-100
PATIENT LF1 (RIGHT SIDE)
-100
PATIENT WD (LEFT SIDE)
P lidkm—**r
-100
PATIENT LE (RIGHT SIDE)
-100
PATIENT JJ (RIGHT SIDE)
Fig. 5 Preserved prism adaptation in patients with infarcts of SCA territory cerebellum or of cerebellar thalamus. (A) Patient LF1 with a
right SCA infarct had a significant after-effect and a normal AC with the right hand. (B) Patient WD with a left SCA infarct had a
significant after-effect and a normal AC with the left hand. (C) Patient LE with a left cerebellar thalamus lacune had a significant aftereffect and a normal AC with the right hand. (D) Patient JJ with a left cerebellar thalamus infarct had a large PC. Line drawings of
lesions are based on MRl/CT scans.
be accounted for by performance deficits alone. Patients with
cerebellar lesions suffer impairment of performance both on
simple (Holmes, 1939; Hore et al., 1991) and complex tasks
(Holmes, 1939; Adams and Victor, 1989; Goodkin et al.,
1993) including ball throwing (Becker et al., 1990). It was
therefore necessary to have measures of performance and
adaptation that were independent, objective and quantitative
to see if deficits in the two were indeed associated. In the
present study, adaptation was gradual and well fitted by an
exponential decay curve; performance was measurable as
scatter in target impacts. This allowed us to dissociate deficits
in adaptation from deficits in performance. Most patients
showed impairment of one or the other, without an association
between the two. Only three patients failed to meet both the
criteria (for normal performance and normal adaptation).
Prism adaptation of throwing is localized within
the cerebellum and its inputs
Baizer and Glickstein (1974) reported in one macaque that
wedge prism adaptation during reaching was abolished by
Eye-hand coordination and the cerebellum
1195
Table 3 Summary of prism performance and adaptation results for patients
Unimpaired performance
Unimpaired adaptation
Impaired adaptation
n = 6 lesions
1/6 PICA—WD
2/3 SCA—WD, LF1
1/3 Cerebellar thalamus—LE
2/2 PM without IOH—MA, RS
n = 17 lesions
1/2 Diffuse cortical—DE
5/6 PICA—WF, CK, JR. JM, LL
2/3 Vermal—RL1, JM
5/5 PM with IOH—DH, RL2, MM, VB, LW
3/3 Ataxia hemiparesis—LF2, NF, GS
1/2 Middle and/or inferior peduncle—RN
0/2
0/3
0/5
0/3
0/2
Impaired performance
Diffuse cortical
Vermal
PM with IOH
Ataxic hemiparesis
Middle/inferior peduncle
0/3 SCA
0/3 Cerebellar thalamus
0/2 PM without IOH
n = 3 lesions
1/3 Vermal—TL
1/3 SCA—FT
1/3 Cerebellar thalamus—DW
0/2
0/6
0/5
0/3
0/2
0/2
Diffuse cortical
PICA
PM with IOH
Ataxic hemiparesis
Middle/inferior peduncle
PM without IOH
n = 3 lesions
1/2 Diffuse cortical—DJ
1/2 Middle and/or inferior peduncle—DS
1/3 Cerebellar thalamus—JJ
0/6
0/3
0/3
0/5
0/3
0/2
PICA
Vermal
SCA
PM with IOH
Ataxic hemiparesis
PM without IOH
Numbers shown as fractions (alb) represent the number of patients with a particular type of lesion within one quadrant (a) over the total
number of patients with this type of lesion (b). Criteria for impairment of performance and adaptation are described in the text. Patients'
initials (see Table 2) are listed in the appropriate quadrant next to the patients' lesions.
cerebellar lesion. Gauthier et al. (1979) reported that a patient
with 'non-acute cerebellar signs and palatal myoclonus' could
not adapt arm reaching to a target while wearing magnifying
lenses. Weiner et al. (1983) reported that patients with
cerebellar disease were impaired in adapting arm reaching
to a target while wearing laterally displacing prisms. They
further showed that adaptation was not impaired by disease
of corticospinal or basal ganglia systems. These studies
did not address lateralization or localization within the
olivocerebellar system. We have confirmed and extended
these results.
Focal damage of the inferior olive, PICA territory of
inferolateral cortex, superior vermis, inferior or middle
cerebellar peduncle, or basal pons all resulted in abnormal
adaptation. Lateralized infarcts in the PICA territory and
inferior peduncle usually produced abnormal adaptation on
the ipsilateral side to the lesion. Lesions in the basal pons
produced abnormal adaptation on the contralateral side to
the lesion. These lesions produced homolateral ataxia and
crural paresis (Fisher, 1978) and impaired adaptation in the
affected arm with normal adaptation with the uninvolved
arm. Two of the patients had small infarcts in the basis pontis
contralateral to the side of the deficits, presumed to involve
(i) the pontocerebellar nuclei which give off mossy fibres
that cross to the contralateral middle cerebellar peduncle and
(ii) the interspersed corticospinal tract also before it crosses
(but see Landau, 1989).
In contrast, the patients with cerebellar outflow lesions
usually adapted despite ataxia in the throwing arm. Two
patients with SCA territory infarcts involving anterior superior
medial cortex and the dentate nucleus and a third with an
evacuation of a right-sided deep cerebellar haemorrhage in
the SCA distribution all showed significant after-effect. Three
patients with lesions of cerebellar thalamus also had ataxic
pinching and manipulation but two of these three showed
normal prism adaptation.
Disease of inferior olive results in spared
performance and impaired adaptation of
throwing
The inferior olive is the exclusive source of climbing fibres
to the cerebellum (Szentagothai and Rajkovits, 1959). Cooling
of the inferior olive immediately increases firing rates of
Purkinje cells (Strata, 1985); damage eventually leads to
cerebellar atrophy and ataxia (Murphy and O'Leary, 1971).
Damage of the inferior olive is known to impair a variety of
types of motor adaptation (cf. Thach et al., 1992). The
question has been whether the impairment is primary or
secondary to cerebellar atrophy and errors of movement
performance. In the present study, all four patients with
'symptomatic palatal myoclonus' and inferior olive
hypertrophy (Deuschl et al., 1994) had progressive ataxia of
trunk and gait. However, on this task they had normal
throwing performance (PC =£ 13.3 cm; see Methods) with
1196
T. A. Martin et al.
absent or slowed adaptation. A fifth patient with a stroke,
bilateral palatal myoclonus and right-sided ataxia had normal
performance and abnormal adaptation in the good (left) arm.
Two patients with 'essential palatal myoclonus' (Deuschl
et al., 1994) and no additional neurological defects or
inferior olive hypertrophy showed normal performance and
adaptation. One of these patients (MA) has been described
elsewhere (patient no. 1 in Kane and Thach, 1989) where
we suggested that palatal myoclonus per se results directly
from lesions of the central tegmental tract which denervates
from the nucleus ambiguus and dorsolateral reticular
formation and commonly, but not necessarily, the inferior
olive. Since palatal myoclonus and inferior olivary hypertrophy may each occur one without the other (cf. also Deuschl
et al., 1994), we suggested that the association of the tremor
with the olive damage (and cerebellar ataxia) was fortuitous.
Is superior vermal cortex necessary for gazethrow adaptation?
Lesions of the superior vermal cortex might be expected to
interfere with eye-hand coordination. Vermal lobulus simplex
(lobule VI) has been shown to receive visual and auditory
information and tactile information from the head (Snider
and Eldred, 1952), and lobules V, VI and VII have been
shown to receive proprioceptive information from extraocular
muscles (Fuchs and Kornhuber, 1969). In this area, electrical
stimulation produces saccades (Ron and Robinson, 1973),
ablation produces saccadic dysmetria (Ritchie, 1976), and
Purkinje cells discharge in relation to saccades (Llinas and
Wolfe, 1977). While two out of three patients with superior
vermal lesions showed impaired gaze-throw adaptation, the
fact that the other one of the three patients (with the largest
lesion) met one of the criteria for adaptation, leaves this
localization of this function open to question.
What functions are localized in PICA territory
cortex?
First, prism adaptation of throwing is usually impaired
(without ataxia) by PICA distribution infarcts. Ataxia (without
impairment of adaptation) usually results from SCA
distribution infarcts. The PICA territory infarcts were the
most common focal lesions of cerebellar cortex to impair
adaptation. The PICA territory includes the inferior cerebellar
peduncle and the inferior olive climbing fibres where they
are most tightly collected together. Infarcts giving the
characteristic lateral medullary syndrome impair adaptation
of the vestibulo-ocular reflex presumably because of
involvement of the inferior cerebellar peduncle (Waespe and
Baumgartner, 1992). Since inferior olive disease commonly
impaired or prevented prism adaptation, one possibility is
that the PICA deficits in prism adaptation were also due to
involvement of the inferior cerebellar peduncle. This seems
unlikely to us: (i) only patient CK showed clear involvement
of the inferior peduncle on MRI or CT scanning; (ii) the
cases selected were without other brainstem signs and it
seems improbable that five out six of the PICA territory
infarcts could have involved the peduncle without showing
other brainstem signs. Secondly, basal pontine infarcts
associated with ataxic hemiparesis and impaired adaptation
are thought to interrupt the mossy fibre input to the lateral
hemispheres (PICA territory included). Finally, in a PET
study of adaptation of visually guided reaching to wedge
prisms, Zeffiro noted increased blood flow localized within
the lateral cerebellar cortex (italics ours; Zeffiro, 1995).
If the ablation and the activation localizations do indeed
correspond, this could be clinically useful. Even large PICA
distribution infarcts may produce few or no behavioural
deficits previously recognizable as cerebellar signs.
Of note is the fact that cerebellar 'cognitive functions'
including mental timing (Ivry et al., 1988), learning verbal
associations (Petersen et al., 1989; Raichle et al., 1994),
learning the Tower of Toronto game (Fiez et al., 1992)
and learning maze routes by finger tracing (Van Mier et al.,
1995) have all been localized to this previously 'silent' region
of the cerebellum. What these task performances might
have in common with gaze-throw adaptation remains to be
seen.
Acknowledgements
On a suggestion from Richard Held, Nigel Daw and Torsten
Wiesel developed this task for teaching medical students.
This work was supported by grants to W.T.T. from the
National Institutes of Health (NS12777) and the Office of
Naval Research (N00014-92-J-1827); to T.A.M. and H.P.G.
by NRSA 5 T32 GM07200 and to A.J.B. by the Foundation
for Physical Therapy Research (94D-18-BAS-01).
References
Adams RD, Victor M. Principles of neurology. 4th ed. New York:
McGraw-Hill Information Services, 1989.
Amarenco P. The spectrum of cerebellar infarctions. [Review].
Neurology 1991; 41: 973-9.
Amarenco P, Hauw J-J. Cerebellar infarction in the territory of the
superior cerebellar artery: a clinicopathologic study of 33 cases.
Neurology 1990; 40: 1383-90.
Asanuma C, Thach WT, Jones EG. Anatomical evidence for
segregated focal groupings of efferent cells and their terminal
ramifications in the cerebellothalamic pathway of the monkey. Brain
Res Rev 1983a; 5: 267-97.
Asanuma C, Thach WT, Jones EG. Cytoarchitectonic delineation
of the ventral lateral thalamic region in the monkey. Brain Res Rev
1983b; 5: 219-35.
Asanuma C, Thach WT, Jones EG. Distribution of cerebellar
terminations and their relation to other afferent terminations in the
Eye-hand coordination and the cerebellum
ventral lateral thalamic region of the monkey. Brain Res Rev 1983c;
5: 237-65.
Baizer JS, Glickstein M. Role of cerebellum in prism adaptation. J
Physiol (Lond) 1974; 236: 34P-35P.
Bastian AJ, Thach WT. Cerebellar outflow lesions: a comparison
of movement deficits resulting from lesions at the levels of the
cerebellum and thalamus. Ann Neurol 1995; 38: 881-92.
1197
Kane SA, Thach WT Jr. Palatal myoclonus and function of the
inferior olive: are they related? In: Strata, P. editor. The
olivocerebellar system in motor control. Berlin: Springer-Verlag,
1989: 427-60.
Kase CS, Norrving B, Levine SR, Babikian VL, Chodosh EH, Wolf
PA, et al. Cerebellar infarction. Clinical and anatomic observations
in 66 cases. Stroke 1993; 24: 76-83.
Bastian AJ, Martin TA, Keating JG, Thach WT. Cerebellar ataxia:
abnormal control of interaction torques across multiple joints. J
Neurophysiol 1996. In press.
Keating JG, Thach WT. Cerebellar motor learning: quantitation of
movement adaptation and performance in Rhesus monkeys and
humans implicates cortex as the site of adaptation [abstract]. Soc
Neurosci Abstr 1990; 16: 762.
Becker WJ, Kunesch E, Freund H-J. Coordination of a multijoint movement in normal humans and in patients with cerebellar
dysfunction. Can J Neurol Sci 1990; 17: 264-74.
Kohler I. The formation and transformation of the visual world
(translated by Fiss H.) Psychol Issues 1964; 3: 1-173.
Bloedel JR, Zuo C-C. The heterosynaptic action of climbing fibers
in the cerebellar cortex. In: Strata P, editor. The olivocerebellar
system in motor control. Berlin: Springer-Verlag, 1989: 246-64.
Darlington RB, Nathan RG. Radicals and squares, and other
statistical procedures for the behavioral sciences. Ithaca (NY):
Logan Hill Press, 1975.
Deuschl G, Toro C, Valls-Sole J, Zeffiro T, Zee DS, Hallett M.
Symptomatic and essential palatal tremor. 1. Clinical, physiological
and MRI analysis. Brain 1994; 117: 775-88.
Fiez JA, Petersen SE, Cheney MK, Raichle ME. Impaired nonmotor learning and error detection associated with cerebellar damage.
A single case study. Brain 1992; 115: 155-78.
Fisher CM. Ataxic hemiparesis. A pathologic study. Arch Neurol
1978; 35: 126-8.
Fuchs AF, Kornhuber HH. Extraocular muscle afferents to the
cerebellum of the cat. J Physiol (Lond) 1969; 200: 713-22.
Gauthier GM, Hofferer J-M, Hoyt WF, Stark L. Visual-motor
adaptation: quantitative demonstration in patients with posterior
fossa involvement. Arch Neurol 1979; 36: 155-60.
Goodkin HP, Keating JG, Martin TA, Thach WT. Preserved simple
and impaired compound movement after infarction in the territory
of the superior cerebellar artery. Can J Neurol Sci 1993; 20 Suppl.
3: S93-S104.
Harris CS. Adaptation to displaced vision: visual, motor, or
proprioceptive change? Science 1963; 140: 812-3.
Held R, Hein AV. Adaptation to disarranged hand-eye coordination
contingent upon re-afferent stimulation. Percept Mot Skills 1958;
8: 87-90.
Helmholtz HLF von. Treatise on physiological optics, Vol. 3, Sect.
29.Translated from the 3rd German edition by Southall JPC.
Menasha (WI): George Banta Publishing, 1924-5.
Holmes G. The cerebellum of man. The Hughlings Jackson Memorial
Lecture. Brain 1939; 62: 1-30.
Hore J, Wild B, Diener H-C. Cerebellar dysmetria at the elbow,
wrist, and fingers. J Neurophysiol 1991; 65: 563-71.
Ivry RB, Keele SW, Diener HC. Dissociation of the lateral and
medial cerebellum in movement timing and movement execution.
Exp Brain Res 1988; 73: 167-80.
Landau WM. Clinical neuromythology VI. Au clair de lacune: holy,
wholly, holey logic. Neurology 1989; 39: 725-30.
Llinas R, Wolfe JW. Functional linkage between the electrical
activity in the vermal cerebellar cortex and saccadic eye movements.
Exp Brain Res 1977; 29: 1-14.
Martin TA, Keating JG, Goodkin HP, Bastian AJ, Thach WT.
Localization of specific regions of the cerebellar system involved
in prism adaptation [abstact]. Soc Neurosci Abstr 1995; 21: 917.
Murphy MG, O'Leary JL. Neurological deficits in cats with lesions
of the olivocerebellar system. Arch Neurol 1971; 24: 145-57.
Petersen SE, Fox PT, Posner MI, Mintun M, Raichle ME. Positron
emission tomographic studies of the cortical anatomy of singleword processing. J Cogn Neurosci 1989; 1: 153-70.
Raichle ME, Fiez JA, Videen TO, MacLeod A-MK, Pardo JV, Fox
PT et al. Practice-related changes in human brain functional anatomy
during non-motor learning. Cereb Cortex 1994; 4: 8-26.
Ritchie L. Effects of cerebellar lesions on saccadic eye movements.
J Neurophysiol 1976; 39: 1246-56.
Ron S, Robinson DA. Eye movements evoked by cerebellar
stimulation in the alert monkey. J Neurophysiol 1973; 36: 1004-22.
Snider RS, Eldred E. Cerebro-cerebellar relationships in the monkey.
J Neurophysiol 1952; 15: 2 7 ^ 0 .
Strata P. Inferior olive: functional aspects. In: Bloedel JR, Dichgans
J, Precht W, editors. Cerebellar functions. Berlin: Springer-Verlag,
1985: 230-46.
Szentagothai J, Rajkovits K. Ober den Ursprung der Kletterfasern
des Kleinhirns. Anat Entwgesch 1959; 121: 130-41.
Thach WT, Keating JG, Goodkin HP. Inferior olive disease in man
impairs learning novel synergies [abstract]. Soc Neurosci Abstr
1991; 17: 1380.
Thach WT, Goodkin HP, Keating JG. The cerebellum and the
adaptive coordination of movement. [Review]. Annu Rev Neurosci
1992; 15: 403^2.
van Mier H, Tempel LW, Perlmutter JS, Raichle ME, Petersen SE.
Generalization of practice-related effects in motor learning using
the dominant and non-dominant hand measured by PET [abstract],
Soc Neurosci Abstr 1995; 21: 1441.
Vickers JN. Gaze control in basketball foul shooting. In: Findlay
1198
T. A. Martin et al.
JM, Kentridge RW, Walker R, editors. Eye movements, processes,
mechanisms and applications. Amsterdam: North Holland, 1994.
membrane reflex: performance deficits of the conditioned and
unconditioned response. J Neurosci 1989; 9: 299-311.
Waespe W, Baumgartner R. Enduring dysmetria and impaired gain
adaptivity of saccadic eye movements in Wallenberg's lateral
medullary syndrome. Brain 1992; 115: 1123^6.
Zeffiro T. Adaptation of visually-guided reaching to laterally
displaced vision: a regional cerebral blood flow study [abstract],
H u m B r a i n M a p p i n g 1 9 9 5 ; S u p p i 1: 333.
Weiner MJ, Hallett M, Funkenstein HH. Adaptation to lateral
displacement of vision in patients with lesions of the central nervous
system. Neurology 1983; 33: 766-72.
Welsh JP, Harvey JA. Cerebellar lesions and the nictitating
Received December 29, 1995. Revised March 12, 1996.
Accepted April 1, 1996