Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Synaptogenesis wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Development of the nervous system wikipedia , lookup
Sensory substitution wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Neural engineering wikipedia , lookup
Node of Ranvier wikipedia , lookup
Microneurography wikipedia , lookup
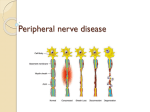
OS 211 [A]: Integration, Coordination, and Behavior Lec 34: Peripheral Neuropathy December 6, 2013 Geraldine S. Espritu, MD TOPIC OUTLINE I. Overview II. Peripheral Nerve Damages III. Basic Physiology IV. Examination V. Generalized/Polyneuropathy VI. Focal Neuropathy VII. Others 1 Will take years to get to the degeneration stage If nerve has a demyelinating problem (sheath loss stage), it is usually reversible because the neuron is still intact, but once disconnection occurs, damage is permanent Legends: From the Powerpoint presentation and 2016 From the lecture 2016A From our lecture Hello guys! Ma’am said to focus on table 6 and table 7 (pages 5 and 6) for her 5 questions. Her favorite questions are still the same as in 2016A’s exam (in boxes), so we just added a few more notes from her very short lecture. I. OVERVIEW A. PERIPHERAL NERVES For your nerve to function, everything needs to be healthy: neuron, myelin and axon Myelinated by individual Schwann cells (instead of oligodendrocytes in the CNS which are myelinated like an octopus) 1:1 ratio of peripheral nerve to Schwann cell Damage confined to neuron, axon and myelin Figure 2. Typical Process of Damage in Peripheral Nerves. NEURONAL/NEUROPATHY Best way to kill a nerve is to cut its axon (neuron), faster than to demyelinate it Most common problem: if anterior horn or dorsal root is attacked (eg. Herpes Zoster) In a war, you want to preserve the headquarters, the headquarters is the dorsal root Attack the headquarters to destroy the government If you attack the myelin only, you only hit the satellite stations Figure 1. The Peripheral Nerve BASIC PRINCIPLES Functional Classification of a Nerve: o Motor o Sensory o Autonomic Normal nerve integrity and function rely on the proper functioning of the four components: o Neuron o Axon o Myelin o Connective Tissue – there are a lot of diseases that affect the connective tissue or vascularization of the nerve that would cause damage (ex. Diabeties, ischemia, drugs, alcohol) Interruption or impairment of any of these structures can lead to transient or permanent nerve injury. Symptoms parallel function: motor, sensory, autonomic Also can be affected by problems of supply (glucose, protein) PERIPHERAL NERVE DAMAGE Pathology: o Axonal o Demyelinating o Combined II. PERIPHERAL NERVE DAMAGES A. TYPICAL DAMAGE PROCESS Starts with demyelination, then compression, then disconnection (here damage is permanent) and then degeneration (retrograde damage, takes years) SEAN, MISH, KYLE Figure 3. Neuropathy on Dorsal Root Ganglion. Table 1. Neuronal vs. Axonal Degeneration. Description Classification and Prognosis Examples Neuronal Degeneration Primary Inherited disorders: e.g. Degenerative loss/destruction of spinal muscular disorder of neuron cell body with no nerve cell bodies atrophies, amyloidosis possibility of accompanied by Motor Neuron Disease recovery degeneration of their peripheral and Toxic: cadmium central axons poisoning Polio virus Breakdown of the axon and myelin sheath that progresses toward the nerve body Axonal Degeneration Axonal polyneuropathies Recovery is delayed and often incomplete Most toxic/metabolic neuropathies POLIO A lot of people have polio-like symptoms now Page 1 / 6 Lec 34: Peripheral Neuropathy Polio is acute, acquired in childhood One limb is shorter than the other Anterior (L3) horn cells are destroyed Once neuron is targeted, there’s no way of recovery. Once you grow up with polio, damage doesn’t go away ALS (not mentioned by Ma’am) Motor neuron disease Degenerative disease with slow muscle atrophy. All motor neurons affected, not just one limb (versus polio). improper manufacture (congenital) of myelin sheaths with relative sparing of axons Syndrome Hereditatry disorders of Schwann cell-myelin metabolism: e.g. metachromatic leukodsytrophy, DejerineSottas disease III. BASIC PHYSIOLOGY OS 213 In acquired disorders, recovery is dependent on remyelination or demyelinated segments, which can take from days to several months A. MYELIN Myelin is a good insulator and facilitates conduction The thicker the myelin, the faster the nerve conduction Myelinated nerve is 50x faster Myelin also serves as a protector Compression or entrapment mononeuropathies; CTS B. PERIPHERAL NEUROPATHY 1. Variety of syndromes that result from lesions of the peripheral nerve o Cranial nerve (except I and II) Smelling and vision; they are not peripheral nerves because they are outpouchings of the cortex. o Spinal nerve (motor, sensory, autonomic) 2. Mononeuropathy (single) 3. Mononeuropathy multiplex (multiple) 4. Generalized/polyneuropathy Figure 4. Myelinated nerves. (Left) Healthy nerves surrounded by myelin, (right) myelinated nerve in high resolution. PHYSIOLOGICAL EFFECTS OF DEMYELINATION Impede salutatory conduction Temporary inductions by heat and exercise, hyperventilation, smoking, fatigue If with myelin: like the LRT which only stops at some points, faster If without myelin: like a jeepney which stops everywhere, slower Worst case if everything is demyelinated Surrounding Schwann cells can be generous and give myelin sheath to the demyelinated axon Recovery is good in demyelination 2016A: Favorite question! 1. All are peripheral nerves except I and II. All spinal nerves are considered part of peripheral nerves. CN I and II do not have Lower Motor Neurons. HISTORY Determine whether presenting symptom is sensory, motor, autonomic Evolution, order of body parts involved (symmetrical vs. asymmetrical) Onset, duration, temporal course (acute, sub acute, progressive, relapsing or remitting) – the most important questions to ask o 2016A: Onset important. Classify the disease based on how fast the damage is: if fast, axonal; if slower, demyelinating Exposure to toxin, concurrent medical history, family history, medications, injury, prior infection, dietary habits o Ex. Silver tooth filling or gold teeth can cause dementia because of prolonged exposure. Choose the white pasta for your teeth! SENSORY SYMPTOMS Sensory involvement is an important diagnostic key This is usually the only reason why they go to the doctor For peripheral nerves, important to remember your dermatomes! SYMPTOMS OF NEUROPATHY Fig. 5. Conduction in Myelinated and Demyelinated Fibers. Myelinated nerve fibers (top) conduct faster while demyelinated nerve fibers (bottom) conduct more slowly. SEGMENTAL DEMYELINATION Table 2. Segmental Demyelination. Know the classification and examples. Description Classification and Prognosis Examples Breakdown Immune-mediated acquired demyelinating neuropathies: Acquired or e.g. Guillian-Barré SEAN, MISH, KYLE Recovery does not occur in congenital disorders Table 3. Symptoms Of Neuropathy. A positive symptom is an abnormal or exaggerated feeling of something that isn’t felt normally, whereas a negative symptom is not feeling the stimulus that is being given to you. System Positive Negative Cramps Weakness Motor Fasciculations Fatigability Myokynesia (quivering) Hypotonia Restless legs Arreflexia Tightness Deformities (pes cavus, claw hand) *especially if hitting a motor nerve Parasthesias Loss of vibration sense Sensory Tingling Loss of joint position sense (large fiber) Arreflexia Sensory ataxia (positive Romberg test) Hypotonia Sensory Burning, jabbing pain Loss of pain sense Page 2 / 6 Lec 34: Peripheral Neuropathy (small fiber) Autonomic (dysesthesias) Hyperhidrosis (excessive sweating) Excess saliva Loss of temperature sense Orthostasis Erectile dysfunction Bowel and/or bladder dysfunction Anhidrosis NOTE: Treatment of hyperhidrosis is botox. It is a neuromuscular junction blocker, but it has no connection to the autonomic functions. Even neurologists are still baffled as to why botox works for hyperhidrosis. Table 4. Sensory Symptoms. Positive Burning Pricking pain Electric, shock-like feelings Tightness Hypersensitivity to touch Negative Numbness Deadness Feeling of wearing gloves or walking on stilts Loss of balance Painless injuries OS 213 1. Motor System Evaluation Gait Reflexes Abnormal movements Tone Strength 2. Sensory Testing Testing position Palpate for pulse Testing with pinprick Testing with cotton wool Testing with a tuning fork 3. Approach Compare distal sensation to proximal sensation Look for symmetry by comparing one side to the other Test each of the dermatomes TEST FOR NEUROPATHY 1. Monofilament Screening Test 2. Nerve conduction velocity measurements 3. Testing for reflex - can give one an idea if there is a disruption in the reflex arc IV. EXAMINATION A. COMPLETE PHYSICAL EXAM NOTE: TAKE GOOD HISTORY *Look and Locate: Compare right and left, memorize dermatomes Systemic disorders o Diabetes o Vasculatis o Lupus Orthostatic hypotension Atrophy, Swelling Skin changes, Mees’ lines o Look for rashes Figure 7. Tests for Neuropathy. V. GENERALIZED/POLYNEUROPATHY A. Herpes Zoster B. SLE Classic picture of advanced, diffuse neuropathy with distal wasting, weakness, absent tendon reflex, & glove & stocking distribution Distal nerves are affected first Usually sensory fibers are affected first before motor fibers Something generalized is affecting a lot of your nerves at one time It involves generalized medical conditions: o Endocrine o Toxicologic Patients undergoing chemotherapy may exhibit pain and numbness because of the toxic effects of the medications. o Nutritional Common among those who don’t eat meat or with Vit D deficiency o Vasculitis A. DIABETIC NEUROPATHY C. Lupus-like symptoms, can be rheumatoid arthritis. D. Hand atrophy Figure 6. Physical Exam. Look and locate signs of Herpes Zoster, SLE, Lupus-like symptoms, atrophy and diabetic foot. Grandparents’ feet can be patchy, which can indicate that circulation is compromised. E. Diabetic foot: dry skin, discoloration, poor perfusion to toes B. NEUROLOGIC EXAM Optic pallor Deep tendon reflex Pain, light touch, position, vibration sense Palpate peripheral nerve trunks Most common, rising Complications: neuropathy An estimated 10-65% of patients with diabetes have some form of peripheral neuropathy. Neuropathy is estimated to be present in 7.5% of patients at the diagnosis of diabetes. If you are a diabetic, wish for a positive neuropathy. Everything will be heightened, including kisses 50% have distal symmetric polyneuropathy, and 25% have compression or entrapment neuropathies (mainly carpal tunnel syndrome). Patients complain of ‘ngalay’ or tingling Diabetes affects all 4 major components: o Metabolic changes (sorbitol) o Microcirculation o Neuropathy o Retinopathy CLASSIFICATION OF DIABETIC NEUROPATHY 1. Diffuse Somatic Neuropathy Sensorimotor Distal symmetrical sensorimotor polyneuropathy o Primarily small-fiber neuropathy o Primarily large-fiber neuropathy o Mixed 2. Focal Neuropathy – numbness of feet and hands or problems of nerve roots Mononeuropathy (CTS) Monnoneuropathy multiplex Amyotrophy (nerve roots) NEUROPATHIC PAIN SEAN, MISH, KYLE Page 3 / 6 Lec 34: Peripheral Neuropathy A. Diffused Type B. Focal Type C. Focal Type Figure 8. Diabetic Neuropathy. Diffused and Focal type VASCULAR THEORY 1. Endoneurial ischemia develops because of increased endoneurial vascular resistance to hyperglycemic blood. 2. Various metabolic factors, including formation of advanced glycosylation end products, also have been implicated. 3. Leading to capillary damage, inhibition of axonal transport, Na+/K+ATPase activity, and finally to axonal degeneration METABOLIC THEORY 1. Proposes that hyperglycemia causes increased levels of intracellular glucose in nerves, leading to saturation of the normally used glycolytic pathway. 2. The extra glucose is shunted into the polyol pathway and converted to sorbitol and fructose by the enzymes aldose reductase and sorbitol dehydrogenase. 3. Accumulation of sorbitol and fructose leads to reduced nerve myoinositol, decreased membrane Na+/K+-ATPase activity, impaired axonal transport, and structural breakdown of the nerve, causing slowing of conduction velocities Figure 9. Pathogenesis Of DM Nephropathy Based On The Vascular Theory. Did not discuss that much, she discussed the metabolic theory diagram more. NERVE DIES OUT DUE TO ISCHEMIA/POOR FLOW TO NERVE Figure 10. Pathogenesis of DM Neuropathy based on the Metabolic Theory. Reduced blood flow shuts down pump, hyperglycemia increases neurovascular resistance, and increased sorbitol decreases blood flow – also contributing to the damage. This looks complicated, but just look at the source: exercise and control of blood sugar. ASIDE FROM ISCHEMIA, HIGH SUGAR CONTENT CAUSES MORE DAMAGE BECAUSE OF IMBALANCE (FRUCTOSE, SORBITOL) WHICH ARE IMPORTANT FOR THE NERVE. MANAGEMENT OF DM NEUROPATHY SEAN, MISH, KYLE OS 213 Primary concern: Control of Blood Sugar (stop whatever is attacking the nerve) Ameliorate painful symptoms Improve neurovascular circulation - decreased circulation (leading to nerve death) is the main reason why DM patients have neuropathy 2016A: Usually have foot cut off because patients cannot feel and has an eroded wound; if more than 70% occlusion, amputate Wearing wedges can help prevent focal compressions in your legs Do an ultrasound first before you amputate B. GUILLAINE-BARRE SYNDROME Autoimmune response triggered via infection or vaccination o Immune cells attack Schwann cells leading to demyelination o Mediated by antibodies (but also CMI) Background: Classic Guillaine-Barré syndrome (GBS) is an acute, ascending, and progressive neuropathy characterized by weakness, paresthesias, and hyporeflexia. You get an infection through vaccination, colds or cough. After two weeks, walking feels heavy, then eventually becomes paralyzed. In severe cases, muscle weakness may lead to respiratory failure. Severe labile autonomic dysfunction may also occur. Maximal weakness typically occurs 2 weeks after the initial onset of symptoms but may evolve early and abruptly. Begins as numbness Attacks the virus, then your own nerve EPIDEMIOLOGY AND ECONOMIC IMPACT Most common acute neuropathy in clinical practice. GBS affects between 1-4 per 100,000 of the world’s population annually. Sex: predominant in males 1.5:1 (sees a lot of females now together with males) Age: all ages o Bimodal distribution o Peaks at 15-35 and 50-75 years old The costs in the US have been estimated as $110,000 for direct health care and $360,000 in lost productivity per patient. AUTOIMMUNE THEORY Impede salutatory conduction Targets the Schwann cells GBS is believed to result from an autoimmune response triggered by an antecedent illness or by any of a long list of medical conditions. Usually when patient clears out a vaccine or has an infection, immune cells attack Schwann cells leading to demyelination The autoimmune response seems to have both humoral and cellmediated components. Recognized variants: AIDP, AMAN (Acute Motor Axonal), MFS, AMSAN (Acute Motor Sensory Axonal) AIDP: humoral immune reaction to schwann cell membrane or myelin AMAN and MFS are strongly associated with non protein anti ganglioside antibodies (antiGQ1b antibodies for MFS and anti GD1a anti GM1 for AMAN) Common pathology is loss of myelin due to antibody attack on schwann cell and myelin sheath. In a subset of patients with GBS, axonal damage results from a direct cellular immune attack on the axon itself. Segmental pattern Figure 11. Segmental Demyelination and Remyelination: Sural Nerve Biopsy. This is the common pathology in GBS. The internodal segment (arrow) shows marked reduction of myelin thickness compared to the adjacent internodes, indicating remyelination of a focally demyelinated axon. JUST TARGETS THE SCHWANN CELL, JUST A NODE NOT THE WHOLE NERVE Teased nerve fiber preparation. CAUSES 2/3 of patients have a history of GI or respiratory infection from 1-3 weeks prior to onset of weakness. Page 4 / 6 Lec 34: Peripheral Neuropathy Table 5. Causes of GBS Infections Chlamydia Campylobacter jejuni Hepatitis B Mycoplasma pneumonia Cytomegalovirus Epstein-Barr virus Human Immunodeficiency Virus (HIV) Vaccinations Group A streptococci Rabies Swine flu Influenza *When you get a vaccine, make sure you don’t have other infections (cough, cold, UTI) because you might develop an immune response and have GBS. FEATURES OF GBS Onset Weakness: o Most often symptomatic in legs o Pain: Low back & legs o Paresthesias: Distal Weakness o Starts as distal, ascending weakness o Distribution: Proximal + Distal; Symmetric o Severity: Quadriplegia in 30%; Bedbound another 30% o Respiratory failure Cranial Nerves (70%) o VII (FACIAL DIPLEGIA) Extra-ocular: Miller-Fisher (atypical, frozen eyeball) Tongue: Symmetric; Common (50%) Sensory: Paresthesias: Initial symptom in 50% o Eventually occur in 70% to 90% o Pain Prominent in 70% PROGNOSIS AND TREATMENT GBS is a monophasic disease, symptoms start to resolve or plateau by the 4th week of illness; once you get the cells out of the body, symptoms will go away Watch out for respiratory failure Weakness usually resolves with supportive care but best if with treatment (IVIG agent binds with IVIG then flush out or plasma exchange remove the offending agent) o Remove the offending agent SUPPORTIVE CARE Most important in the treatment of GBS is excellent general care and intensive care Respiratory support o 2016A: Respiratory failure is the most common cause of death Fluids and nutritional support Monitoring and good nursing care 2016A Questions: 2. What differentiates DM from GBS? Acute (GBS) vs. Chronic (DM). Sensory (DM) vs. Motor (GBS). GBS leads to death because of respiration failure (paralyzed muscles of breathing), DM spares trunk muscles. 3. What is the most common pathology of GBS? Mostly demyelinating, sometimes attacks axon first. DIAGNOSTIC STUDIES Diagnosis usually is made on clinical grounds and confirmed by tests Lumbar puncture and spinal fluid analysis o Why do a lumbar puncture? Because myelin is protein. The protein disintegrates and can sometimes be found in the CSF. Most, but not all, patients have an elevated level of CSF protein (>400 mg/L), with no elevation in CSF cell counts “Protein cell dissociation” High protein because myelin is punctured, thus high myelin OS 213 Wrist drop = radial nerve Trigeminal neuralgia – from chin then goes all the way up (video) When the whole side of the face is paralyzed, the lesion is peripheral (Bell’s Palsy) When the forehead is spared, the lesion is central (e.g. Stroke) B. FACIAL NERVE Figure 11. Left: Areas of possible nerve damage. Right: Bell’s Palsy VII. OTHERS Acute vs. Chronic Starts as focal but become generalized o Hansen’s disease (leprosy): increase due to lack in funding of medication o Lead o Mercury o Diabetes o CTD (Connective Tissue) Mixed sensory and motor Mixed axonal and demyelinating o Autoimmune o Paraneoplastic o Toxicologic/chemotherapy 2016A Questions: 4. The following should cause mixed axonal and demyelinating neuropathy except… Autoimmune paraneoplastic, toxicologic/chemotherapy cause it, rule out these. Table 6. Etiology. May get 2 questions from here. As a doctor, you should know the etiology so you can manage appropriately. Structure Disease Anterior Horn Cell Poliomyelitis Dorsal Root Ganglia Herpes Zoster Myelin Sheath Guillain Barre Axons Arsenic Myelin and Axon Alcohol/Nutritional Blood Vessels Diabetes Connective Tissue SLE, Amyloid Cheap hair dye with chemicals can cause frequent headaches Plastic or paint of toys may also contain toxic chemicals VI. FOCAL NEUROPATHY Involves only one nerve. Unlike polyneuropathy, the symptoms of focal neuropathy are specific for the nerve injured or affected. Commonly in the hand, leg or lower back. Any nerve can be affected Often due to compression = demyelinating Trauma = both axonal and demyelinating Example: carpal tunnel syndrome Trigeminal neuralgia = “kumakapal, sumasakit” A. NEURALGIA SEAN, MISH, KYLE Page 5 / 6 Lec 34: Peripheral Neuropathy Figure 12. Normal sural nerve biopsy. Normal density of myelinated nerve fibers. One micron thick toluidine blue-stained plastic-embedded cross section. All the nerves should be round and healthy with good blood flow. Myelin has good supporting tissue. MARAMING MALIIT NA MYELIN FIBERS Leprosy Diphtheria METABOLIC/ENDOCRINE Renal/Hepatic Failure Hypothyroidism TOXIC Lead Arsenic DRUG INDUCED: INH OS 213 Sensory Motor Sensory/sensorimotor Sensory/sensorimotor Motor Sensory Sensory VII. SUMMARY First: Determine if patient has peripheral neuropathy Second: Determine pattern of peripheral neuropathy involvement Third: Determine the underlying cause Treat/Correct cause as well as the symptoms END OF TRANSCRIPTION Appendix. Posterior and Anterior Dermatomes Figure 13. Amyloid neuropathy: sural nerve biopsy. Amyloid deposits (arrows) in the endoneurium, in a patient with amyloid neuropathy caused by a transthyretin gene mutation. Congo red stain paraffin section. Dead Sural nerve shows occlusion with amyloid deposits. There is no myelin, integrity and supportive tissue. HAS AMYLOID, NO MORE MYELIN (Common in connective tissue diseases and amyloid neuropathy) Figure 14. Lepromatous neuropathy: sural nerve biopsy. Several Schwann cells contain Mycobacterium leprae bacilli (arrow). Electron microscopy, original magnification x5500. There is no myelin and the shape gone, last fiber of whole sural nerve. It attacks everything myelin, including axon supporting tissue. Leprosy is coming back because the WHO cut off the funding for their drug. Table 7. ACQUIRED. More questions from this table. Disorder Diabetes NUTRITIONAL Vitamin B, Vitamin E, Alcoholic IMMUNE MEDIATED GBS CIDP MNCB VASCULITIS PARANEOPLASTIC Lung CA Lymphoma INFECTIOUS Herpes SEAN, MISH, KYLE Presentation Sensory, sensorimotor, focal, multifocal Sensory Sensorimotor Acute: motor, sensory, autonomic, opthalmoparesis Chronic: motor sensorimotor, demyelinating Multifocal motor Multifocal Sensory Motor, Sensorimotor Sensory radiculopathy Page 6 / 6