Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Innate immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
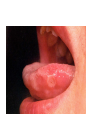
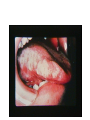
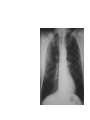
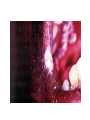
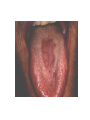
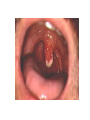
Immune System and Natural History of HIV Infection Vijay Kandula, MD MPH AAHIVS Adjunct Assistant Professor Division of Public Health, Department of Family and Preventive Medicine University of Utah, Salt Lake City Components of the Immune System • Organs • Cells • Molecules •Immunoglobulins •Complement system Organs of the Immune System Tonsils and adenoids Lymph nodes Lymphatic vessels Thymus Lymph nodes Spleen Peyer’s patches Appendix Lymph nodes Bone marrow Lymphatic vessels Cells of the Immune System Bone graft Macrophage Mast cell Eosinophil Marrow Bone Erythrocytes Basophil Monocyte Megakaryocyte Hematopoietic stem cell Multipotential stem cell Myeloid progenitor Neutrophil cell Platelets Lymphoid progenitor cell Dendritic cell T lymphocyte Natural killer cell B lymphocyte B Cells Antigen-specific B cell receptor Class II MHC and processed antigen are displayed Antigen Antibodies B cell Lymphokines Antigen-presenting bacteria Plasma cell Activated helper T cell B Cells produce Antibodies • What do they do? • Can be protective: E.g Hepatitis A and B, Varicella…. • Not protective: HIV, Hepatitis C •How do we use them? • To protect against infection: E.G Hep A Ig if travelling • To diagnose • Window period? T Cells Resting helper T cell Activated helper T cell CD-4 Cell Resting cytotoxic T cell Activated killer cell CD-8 Cell Phagocytes and Their Relatives Monocyte Eosinophil Mast cell Macrophage Dendritic cell Neutrophil Basophil Complement C2 C3 C3a C5a C1 C6 C8 C5b IgG Antigen C7 C4 Enzyme C3b C5 C5b C9 Kinds of Immunity Active immunity Passive immunity Naturally acquired Naturally acquired Artificially acquired Artificially acquired Immune System Disorder • Though immune system defends the body – Imbalance leads to problems • Three common immune system disorders: • allergies • autoimmune diseases • immunodeficiency diseases Disorders of the Immune System: Allergy Interleukins Allergen IgE Mediators Symptoms B cell Mature helper T cell Plasma cell Mast cell Disorders of the Immune System: Autoimmune Disease Pancreas Cytotoxic T cell Beta cell Immunodeficiency Diseases • weakened immune response. • the immune system fails to develop normally. • Affected by drugs and other diseases • Infection: Acquired immunodeficiency disease is AIDS. – Allergies result when antigens from allergens bind to • • • • histamines. pathogens. mast cells. T cells. – An example of an autoimmune disease is • • • • polio. multiple sclerosis. asthma. smallpox. 403 – In Type I diabetes, antibodies attack • • • • connective tissues around the joints. neuromuscular junctions. insulin-producing cells in the pancreas. epinephrine-producing cells in the adrenal cortex. – The retrovirus HIV causes • • • • AIDS. myasthenia gravis. asthma. polio. – The principle targets of the HIV virus are the body’s • • • • red blood cells. helper T cells. connective tissue in the joints. B cells. T Helper cell also know as? Why is natural history important? • Helps to predict the progression of HIV infection • This might help to identify the best moment to start anti-retroviral therapy • Helps targeted drug development to arrest the infection at each of the various stages • What is Public Health importance? HIV Life Cycle Videos 1st thisBasic http://www.youtube.com/watch?v=6gGEU6vw 4J0&feature=related second http://video.about.com/aids/How-AIDSAffects-the-Body.htm thrid http://www.youtube.com/watch?v=RO8MP3w Mvqg&feature=related How HIV infects the body Natural History of HIV Infection CD4 Count, Viral Load and Clinical Course of Untreated HIV Infection in Adults Primary Infection Seroconversion 10,000,000 Intermediate Stage AIDS 1,000,000 1,000 100,000 Plasma HIV Viral Load 10,000 Viral Load 1,000 AIDS 100 CD4 Cells CD4 500 Cell Count 200 10 1 4-8 Weeks 5-10 Years to AIDS Natural History of HIV Infection Survival with AIDS 1 Year 18 Time to Death from Diagnosis of AIDS 1981-1987 Proportion surviving 1.0 0.8 0.6 0.4 0.2 0 0 10 20 30 40 50 60 Months after OI diagnosis Source : National AIDS case surveillance data,27CDC Primary HIV Syndrome - Rash Cerebral Toxoplasmosis Swollen Posterior Cervical Lymph Nodes Seborrheic Dermatitis Natural History of HIV Infection 32 Folliculitis Oral HSV Ulcer and Angular Cheilitis Aphthous Ulcers Dermatomal Herpes (Varicella) Zoster Dermatomal Herpes (Varicella) Zoster Oral Candidiasis Oral Hairy Leukoplakia Pulmonary Tuberculosis With mild –moderate immunosuppression (CD4 > 200) usually presents with typical upper lobe cavitary disease Bacterial Pneumonia Streptococcus pneumoniae Kaposi’s Sarcoma Usually, multiple dark raised lesions. Lesions themselves are not itchy and are rarely painful. Kaposi’s Sarcoma Lymphedema from Kaposi’s Sarcoma Involvement of regional lymph nodes with distal edema is common. Node disease and swelling may be painful. Oral Kaposi’s Sarcoma Implies involvement of internal organs such as gastrointestinal tract Severe Chronic Herpes Simplex Ulcers Persistence for > 1 month is an AIDS-defining condition Umbilicated papules of Molluscum contagiosum and Cryptococcus have the same appearance Pneumocystis carinii (jiroveci) Pneumonia or PCP Subacute or acute illness of more than one week, with fever, severe shortness of breath and cough with little or no sputum Breath sounds may be normal. Bilateral interstitial infiltrates on x-ray are typical. Oesophageal Candidiasis HIV infected patient with oral candidiasis and chest (sub-sternal) pain with swallowing has presumed Candida oesophagitis. Endoscopy would prove the diagnosis but is unnecessary if the patient responds to antifungal therapy. Cryptococcal Meningitis Spinal fluid: may have increased lymphocytes, may have increased protein. Budding yeast seen in spinal fluid in 60-80% with India ink preparation. Enhancing Mass Lesion of the Brain Single ring enhancing lesion with oedema on brain CT scan Primary brain lymphoma versus Toxoplasmosis versus Tuberculoma CNS Toxoplasmosis Response to empiric therapy Cytomegalovirus Retinitis Afebrile patient; reduced vision in one or both eyes; painless; external eye exam normal Retinal exudate and hemorrhage follow retinal vessels Natural History of HIV without Treatment: 10,000,000 1,000,000 100,000 Acute HIV 800 Virologic set-point varies from patient to patient HIV antibodies asymptomatic Minor HIV-related symptoms 500 10,000 Opportunistic infections 1,000 200 100 100 50 10 HIV Viral Load (copies/mL) Months 1 3 about 6mths // Years 5 0 10 yrs CD4 (cells/mL) HIV in plasma (“viral load”) CD4 (T Cell) count Typical course of HIV infection in an untreated person Acute HIV 800 HIV antibodies CD4 count cells/ul 10^6 Minor HIV-related symptoms Virologic set-point varies from patient to patient HIV RNA copies /ml 200 10^2 1 3 about 6mths // Time 5 10 yrs † Outcome with Treatment: low viral load, normal CD4 800 10,000,000 1,000,000 500 100,000 10,000 1,000 200 100 100 50 Months 10 HIV Viral Load (copies/mL) 1 3 about 6mths // HIV in plasma (“viral load”) Years 5 10 yrs 0 CD4 (cells/mL) CD4 (T Cell) count Match the disease with CD4 level at which they are likely to occur Opportunistic Infections CD4 Threshold level CMV Retinitis <50 cells/µl Cryptococcus Meningitis <100 cells/µl Pneumocystis pneumonia <200 cells/µl Cerebral toxoplasmosis <200 cells/µl Oral Candida <200 cells/µl Persistent generalized adenopathy >500 cells/µl Herpes zoster >=500 cells/µl Pulmonary Tuberculosis Any CD Count