Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Human leukocyte antigen wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
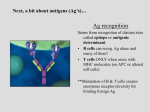
Microbiology 8/26/2008 Major Histocombatibility Complex (MHC) Transcriber: Marc Vance 39:39 Quiz (#2): 1.) The dominant immunoglobulin isotype in human saliva and tears is: a. Monomeric IgG b. Polymeric IgA with J chain and Secretory Component c. Monomeric IgM 2.) The isotype of immunoglobulin in human newborn cord blood that is transferred through the placenta is: a. IgM b. IgG c. IgE - Extra question - What would happen if IgM could transfer through the placenta into the fetus? You could have hemolysis because a lot of antibodies to ABO blood groups are IgM antibodies, and incompatibilities between ABO blood types can occur between mother and fetus, in which case you’d have hemolysis of the fetal red blood cells. Slide 1: Title Slide Slide 2: MHCs (Major Histocompatability Complexes) have two different classes, MHC I and MHC II, each with its own expression and function. B and T cells recognize antigen differently. The antigen receptor on B cell is immunoglobulin (Ig), a transmembrane protein secreted by plasma cells. T cell antigen receptor, TCR, is also a transmembrane protein that is displayed on CD4 helper T cells and the CD8 cytotoxic T cells. Slide 3: B cells can recognize native protein antigens in solution or on bacterial or viral cell surfaces. The secreted antibody is an effector molecule by itself, meaning it can operate at a distance. For example, you can do an ELISA assay you can order your antibodies from California and use them in Birmingham. This won’t work while doing a T cell assay. Most of your plasma cells are in your bone marrow where they secrete antibodies, which can react quickly to neutralize infections all over the body. So antibodies are designed to act at distance. Slide 4: A 3-D image of antigen-antibody interaction (a lysozyme and an Ig shown here, illustrating that antibody recognizes 3-D conformations). There are many different antibody epitopes, meaning that there are various patterns on that lysozyme that a B cell could recognize. Slide 5: T cells, unlike B cells, do not recognize native protein antigens. T cells recognize “processed antigen” - broken down peptides from degraded antigens that are bound to MHC proteins. Microbiology: Major Histocompatability Complex (MHC) Marc Vance Slide 6: The lysozyme shown here could be recognized in its 3-dimensional conformation by an antibody. For a T cell to recognize it, it must be denatured and broken up by proteases into peptides. If this was a foreign lysozyme, our T cells could recognize certain peptide sequences, but only after they are bound to MHC. Slide 7: A T cell receptor (here it is called TCR 2) is shown recognizing an antigenic peptide complexed on a MHC molecule of an antigen presenting cell. Slide 8: T cells require direct cell-to-cell interaction to perform their antigen-specific functions. Slide 9: The MHC complex was discovered during study of inbred strains of mice. The colonies were virtually genetically identical, but due to recessive mutations from inbreeding some of the colonies developed tumors at a high incidence rate while others didn’t. In an attempt to understand the nature of the tumors (and therefore cancer), they were transplanted from a tumor-stricken mouse to a tumorfree mouse. In some colonies the tumor was rejected, on others it would grow. Healthy tissue was then transplanted from a tumor-free mouse onto a tumor-stricken mouse, and that was rejected as well. This showed that the growth/rejection of the tissue was not related to the tumor; it was the MHC complexes in the tissue that signaled it to be foreign. In transplantation between two individuals, these MHC molecules are the major antigen that you need to match if you want the tissue to be accepted. This helps to explain the name – it’s the “major” factor to overcome to make sure the tissue is “histocompatible”. It’s called a “complex” because several genes on chromosome 6 are linked together that encode the proteins that comprise it. While transplantation immunology was how MHCs were discovered, their main function is to display peptide antigens (self and non-self) to T cells, which survey all the body’s cells for this reason. Self antigens elicit no response from T cells, whereas non-self will trigger an immune response. Slide 11: MHC Class I is expressed by all nucleated cells in the body (not expressed by erythrocytes). Its function is to present peptides to CD8+ T cells, which are primarily cytotoxic “killer” T cells (Tc cells). The Tc cells kill virus infected-cells, tumor cells, or any abnormal cells. The images show a Tc cell killing virus infected cells. It is important that all of our nucleated cells express MHC Class I because virtually any nucleated cells could become infected with a virus. Slide 12: MHC Class II is expressed on much fewer cell types. It’s mainly expressed by antigenpresenting cells (APCs; 3 main types - dendritic cells, B cells, macrophages). MHC Class II presents peptide to CD4 T cells (helper T cells, aka Th cells). The APCs present antigen to Th cells, at which point the Th cells can either 1.) Help B cells proliferate, differentiate, isotype switch, or 2.) Help activate macrophages. Remember, MHC Class II –> CD4, MHC Class I –> CD8 pg. 2 Microbiology: Major Histocompatability Complex (MHC) Marc Vance Slide 13: Shown is a Th cell helping a B cell. The B cell’s MHC Class II complex binds with the Th cell’s TCR. The Th cell then secretes IL-4 (a cytokine which promotes isotype switching) directly into the B cell. Slide 14, 15: Both MHC classes are membrane-bound glycoproteins with 4 domains: 2 membrane proximal domains and 2 membrane distal domains that form a peptide binding cleft. Class II MHCs have two chains – alpha and beta, each with two domains. The peptide sits in a cleft in between the two chains. Class I MHCs have a longer alpha-chain with three domains; the peptide binding site is made entirely out of the alpha chain. Class I has a short beta domain (Beta-2 microglobulin). The overall structure of the two MHC classes are very similar. Slide 16: The 3-D structure of MHC is ideal for binding/loading proteins. Slide 17: A “top” view. The peptide “sits” in the cleft. This is what the T cells “see” and recognize. Slide 18: Peptides bound by MHC Class I are bound at each end, while the ends of peptides in the MHC Class II cleft are not bound, it “lays on top” of the MHC protein. An aside – MHC’s must have a peptide associated with it to reach the cell surface. Most of the time it displays a self peptide; only during infection is it a foreign peptide. Slide 19, 20, 21: A B cell is shown expressing both Class I and Class II MHCs. At resting state (no infection), both MHCs are exhibiting self peptide. When an antigen (tetanus toxoid, for example) binds to this B cell’s Ig, it is internalized and degraded into peptides. Newly synthesized MHC Class II’s pick up this new foreign peptide and begin to display it on the cell surface. Meanwhile, your T cells are always patrolling the body for foreign antigens. When a Th cell with affinity for this tetanus peptide comes along, it can bind to the B cell and activate it through cytokines. B cells then proliferate and then differentiate into plasma cells. Slide 22: MHC polymorphisms are allelic variations in MHC genes. This makes organ transplantation difficult. Comparing chromosomes from each parent, the MHC gene sequences are different; hence even siblings would have differences in MHCs. Only identical twins could have the exact same MHC proteins. These polymorphisms are concentrated in the peptide binding regions. Slide 23: A plot of average person-to-person variability in MHC Class I proteins – most are in the alpha-1 and alpha-2 (which makes up the peptide binding site). This allows different MHC proteins to bind different peptides – which is a good thing (slide 26 explains why). Slide 24: The gene complex that makes the HMC – called HLA (Human Leukocyte Antigen; they were originally found on leukocytes). Class I has three different genes; they each encode an alpha-chain, which then associates with beta-2 microglobulin. So every chromosome will yield three different Class I molecules. Class II has three different pairs of alpha and beta chains (DR, DQ and DP); therefore 3 different Class II molecules are expressed per chromosome as well. And since we have two sets of chromosomes (one from each parent), each cell has 6 Class I’s and 6 Class II’s and they are all coexpressed. This diversity of MHC molecules increases the probability of protein binding. pg. 3 Microbiology: Major Histocompatability Complex (MHC) Marc Vance Slide 25: These MHC polymorphisms are at the population level – if we sequenced the variable regions from 100 B cells, each B cell would have a different variable region. All of one person’s MHC genes are the same but comparing person-to-person there is a lot of variation. Note that there are no gene rearrangements with MHC as were seen in the T cell and B cell receptor genetics. Slide 26:.Roughly 1 out of every 3 to 5 T cells can react to foreign MHC, whereas maybe 1 in 1000 T cells can recognize a foreign peptide. This is why transplantation is so difficult - it is so easy to illicit an immune response from a mismatched MHC protein. This helps to illustrate the need for immunosuppressant drugs. A positive of the MHC polymorphisms is that you can change the peptide binding specificity. If we only had one MHC, a viral pathogen could mutate until it was no longer recognized and it would basically be invisible to us. This genetic diversity at a population level helps to ensure that a mutated virus could not infect and kill all humans. Some people might get killed by a virus because their T cells couldn’t detect it, but others’ T cells would. This MHC polymorphism benefits us as a species. An aside - The most common tissue clinically transplanted is the blood. No immunosuppressants are needed for blood transfusions. This is because red blood cells are non-nucleated and they don’t express MHC. They elude natural killer cell’s attention because erythrocytes also lack other target receptors that the NK cells look for Slide 27: The reason for the dual system of Ab-Ag and MHC is illustrated here. With a viral infection, you have infected cells filled with virus as well as extracellular virus molecules to deal with. You need to 1.) Tag and phagocytize the free viruses, which requires Ig, and 2.) Eliminate the infected cells, which is done by Tc cells which need MHC to do their job. Without both of these sides of the immune system, you could not effectively clear the virus. pg. 4