Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
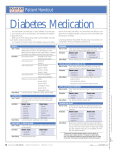
Hypglycaemic Drug Therapy Insulin Therapy Summary of Insulin Classifications Insulin Regimes Oral Hypglycaemic Drugs These will be linked to the following: Insulin therapy There are a large and confusing number of insulin preparations available. If patients are satisfied with their treatment and achieving satisfactory control in the absence of hypoglycaemia, no modification of their regimen is required. Most insulin currently in use is biosynthetically manufactured of human sequence or analogues with altered pharmacokinetic properties. Many patients prefer the ultra shortacting analogues/mixtures for convenience. Some patients prefer to use animal derived insulin in the belief that use of human sequence insulin may cause loss of awareness of hypoglycaemia. Although such a conviction is quite widespread among the users, carefully conducted scientific studies have consistently failed to provide evidence to support this hypothesis. Some preparations are available in both human and porcine versions (e.g. human and porcine actrapid) which can result in confusion in prescribing and dispensing. It is important to realise that such preparations although similar in their characteristics are not interchangeable, and patients should not be inadvertently changed from one to the other. When patients are deliberately changed from animal to human/analogue insulin a dose reduction of 25% is advised. Insulins are most conveniently classified by duration of action as shown in the following table. Summary of insulin classification Ultra short acting Short acting analogues Immediate onset Humalog, Novorapid Duration up to 4 hours Peak action 60 minutes Short acting Soluble insulin Onset 30 minutes Duration up to 5 hours (Human) Actrapid, Velosulin, Humulin S, Insuman Rapid , Pork Actrapid , Peak action 3 hours Hypurin Bovine Neutral, Hypurin Porcine Neutral. Intermediate acting a: Isophane insulin (contains protamine) Onset 90 minutes Duration: 16-20 hours (Human Insulatard, Humulin I, Insuman Basal, Pork Insulatard, Hypurin Bovine Isophane, Hypurin Porcine Isophane. Peak action: 4-12 hours Intermediate acting b: Lente insulin (contains zinc 30% amorphous, 70% crystalline) Onset 120 minutes Monotard, Humulin Lente, Hypurin Bovine Lente. Duration: 24 hours Peak action: 6-18 hours Long acting (a) Ultralente insulin (contains crystalline zinc) Onset 4 hours Ultratard, Humulin Zn, Hypurin Bovine Protamine Zinc. Duration greater than 24 hours Long acting (b) Lantus (insulin glargine) Duration greater than 24 hours Mixed preparations Fixed mixtures of soluble and isophane insulin Biphasic onset and duration of action (Human) Mixtard (10 20 30 40 50) Actrapid / Insulatard in ratios of 10/90 to 50/50 Humulin M2, M3 or M5 Humulin S / Humulin I in ratios of 20/80 to 50/50 Insuman Comb 15, 25 or 50 Insuman Rapid/ Basal in ratios of 15/ 85 to 50/50 Humalog Mix 25 or 50 Lispro/LisproProtamine in ratios of 25/75 or 50/50 Novomix 30 Aspart/Aspart Protamine in a ratio of 30/70 Pork Mixtard 30 Pork Actrapid /Pork Insulatard in a ratio of 30/70 Hypurin Porcine 30/70 Mix Note Ultra short-acting insulins (e.g. Humalog, Novorapid and mixtures i.e. Humalog Mix 25 or 50 and Novomix 30) should be injected immediately before eating or after food. Other insulins should be injected subcutaneously 30 minutes before eating. Insulin regimens Initiation of insulin Patients are normally commenced on human insulin or an insulin analogue, in either a twice daily or a multiple injection regimen. The choice of the initial regimen and subsequent modifications should be made in consultation with the patient, taking due regard of the patient’s occupation and lifestyle. The precise insulin formulation may be determined by the patient’s preferred insulin delivery device. Most patients prefer to use pen devices. Once daily injections Single daily injections do not usually result in good glycaemic control, and are relatively rarely used. Such a regimen may be appropriate for patients where the therapeutic goal is only to prevent ketosis or suppress symptomatic hyperglycaemia, and where there are practical problems with insulin delivery, or particular concern over the risks of nocturnal hypoglycaemia. Elderly patients living alone and patients requiring injections to be given by a district nurse may fall into this category. An intermediate acting lente or isophane insulin is usually most suitable in this context. The long acting basal analogue insulins are under clinical evaluation. Twice daily injections This is a commonly used regimen, and suitable for patients starting on insulin. A combination of short and intermediate acting insulins is taken before breakfast and before the evening meal. Multiple injections This arrangement, involving up to 4 injections a day, has the main advantage of increased flexibility with regard to exercise, meal timing and meal size. It is most likely to work effectively in a well-motivated patient, prepared to do regular and frequent blood glucose testing The majority use an insulin analogue or soluble insulin before each meal, and an injection of an intermediate or long acting insulin usually before bedtime to provide background cover. Oral hypoglycaemic drugs These drugs are suitable for people with Type 2 diabetes when blood glucose control through dietary measures alone proves inadequate. At present five types are available; biguanides (metformin), sulphonylureas, prandial glucose regulators, the thiazolidinediones and the -glucosidase inhibitor acarbose. See Section Error! Reference source not found. for guidance on the role of these drugs in the context of diet and other management strategies. Since in practice the majority of patients are overweight, metformin is usually the drug of first choice. Early sulphonylurea treatment may be appropriate in the thin symptomatic patient without ketonuria. Patients should be educated about their drugs and should carry documentation of any risk of hypoglycaemia. Metformin Action Indications Metformin works principally by reducing insulin resistance. Primary drug treatment of overweight Type 2 diabetics. As an adjuvant to other hypoglycaemic therapy in Type 2 patients. Metformin may be continued in some obese patients with Type 2 diabetes who ultimately require insulin therapy, to maximise insulin sensitivity and minimise weight gain on insulin. Side Effects Diarrhoea, lethargy, anorexia, malabsorption of B12 and folate Lactic acidosis is a very rare but often fatal side effect. It occurs almost exclusively in alcoholics, patients with renal or severe cardiac failure, liver disease, and those who are undergoing surgery or are shocked. Caution Contraindicated in renal failure (creatinine >150µmol/l), liver disease and alcoholism. Discontinue temporarily during severe intercurrent illness. Discontinue for 48-hours following the injection of x-ray contrast media. Dose Initially 500mg daily with main meal, increasing gradually in 500mg increments to a maximum of 1g tds. The dose is often limited by diarrhoea. Sulphonylureas Action Potentiates the pancreatic Indications Primary drug treatment of non-obese patients with Type 2 diabetes. Primary drug treatment of overweight Type 2 patients unable to take usual first line agents. As adjuvant therapy with other agents. Side Effects Hypoglycaemia Weight gain Other side effects are rare. Drugs The three most commonly used sulphonylureas in Grampian are Gliclazide, Glipizide and Glimepiride, the last having the advantage of a once daily single tablet dose. Chlorpropamide and Glibenclamide are particularly prone to cause hypoglycaemia and should not be initiated, and their continued use should be reviewed periodically. Doses It is usually appropriate to start with a small dose before breakfast, increasing progressively according to blood glucose response. The drug should always be taken before meals. Gliclazide 40-320mg daily (doses > 80mg should be divided). Also available as a 30mg modified release tablet (equivalent to 80 mg of standard preparation) – to achieve maximum dose range, patient required to ingest several tablets before breakfast. Glimepiride 1-6 mg as a single daily dose. Glipizide 2.5-20 mg (doses >10 mg should be divided). Prandial glucose regulators Action These agents act as insulin secretagogues, potentiating the post-prandial secretion of insulin that is impaired in the Type 2 diabetes. The postprandial hyperglycaemia associated with increased cardiovascular mortality in the DECODE Study can be improved by using these agents, with dosage timed according to meals. However, the evidence of an improvement in the clinical end-points of reduced cardiovascular events and mortality is not yet available. Indications Repaglinide – As monotherapy or in combination with metformin Nateglinide – In combination with metfomin Side effects Both agents can precipitate hypoglycaemia Caution Dose main meals; daily. Avoid in severe hepatic impairment Repaglinide (Novonorm) - initially 500mcg within 30 minutes before main meals (1mg if transferring from another oral hypoglycaemic), adjusted according to response at 1-2 week intervals. Up to 4 mg as single dose; max daily dose 16mg. Nateglinide (Starlix) - initially 60 mg 3 times daily within 30 minutes of adjust according to response to maximum 180mg 3 times Thiazolidinediones Action A relatively new group of agents acting at the level of the PPAR-gamma receptor to promote insulin sensitivity. To be effective, patients require to have sufficient endogenous insulin production. The maximum therapeutic benefit may not be apparent until after eight weeks. Indications Can be used as monotherapy although Metformin is the drug of first choice. As an adjunct to Metformin in the overweight patient with Type 2 diabetes or with sulphonylurea therapy when Metformin cannot be tolerated in an efficacious dose. Not licensed for use with insulin. Side-effects May promote weight gain and fluid retention Caution Avoid in hepatic impairment – Do not initiate if AAT 2.5 x upper normal limit Use requires a commitment to LFT monitoring on a two-monthly basis for the first year of therapy; thereafter, monitoring periodically is recommended. If AAT is 3x upper normal limit, therapy should be discontinued. Absolute Avoid use in patients with left ventricular impairment or heart failure. Contraindication Dose Pioglitazone (Actos) - 15-45mg once daily Rosiglitazone (Avandia) 4mg daily in combination with a sulphonylurea 4-8mg daily may be used in combination with Metformin Acarbose Action An alpha-glucosidase inhibitor which acts within the gut to slow digestion and absorption of carbohydrates. Indications Primary drug treatment of patients with Type 2 diabetes (especially the obese) if other drugs are contraindicated. As an adjuvant to other oral agents or insulin. Side effects Flatulence and GI disturbance. As mono therapy it does not cause hypoglycaemia. Caution Insulin or sulphonylurea induced hypoglycaemia in patients taking acarbose must be treated with glucose (dextrose) Dose tolerance 25-50mg daily increased very gradually to 50-100mg tds according to