Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Heritability of autism wikipedia , lookup
Medical genetics wikipedia , lookup
BRCA mutation wikipedia , lookup
Population genetics wikipedia , lookup
Microevolution wikipedia , lookup
Birth defect wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Frontonasal dysplasia wikipedia , lookup
Oncogenomics wikipedia , lookup
Koinophilia wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Down syndrome wikipedia , lookup
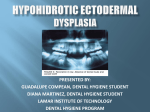
Atlas of Genetics and Cytogenetics in Oncology and Haematology INIST-CNRS OPEN ACCESS JOURNAL Cancer Prone Disease Section Short Communication Schöpf-Schulz-Passarge syndrome (SSPS) John A McGrath St John's Institute of Dermatology, King's College London (Guy's Campus), London, United Kingdom (JAM) Published in Atlas Database: July 2012 Online updated version : http://AtlasGeneticsOncology.org/Kprones/SchopfSchulzPassargeID10138.html DOI: 10.4267/2042/48372 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2012 Atlas of Genetics and Cytogenetics in Oncology and Haematology Identity Clinics Other names Keratosis palmoplantaris with cystic eyelids, hypodontia, and hypotrichosis. Eccrine tumours with ectodermal dysplasia. Note SSPS is an eponymous form of ectodermal dysplasia first described in 1971 by Erwin Schöpf, Johann Schulz and Eberhard Passarge in a report of two sisters with eyelid cysts, hypodontia, hypotrichosis, palmoplantar hyperkeratosis and nail dystrophy. Inheritance Autosomal recessive. Fewer than 100 cases of SSPS have been reported. Heterozygous carriers may show some ectodermal anomalies (predominantly hair/nails in females, teeth in males). Phenotype and clinics SSPS is characterized by eyelid cysts (apocrine hidrocystomas), palmoplantar keratoderma, hypodontia, hyperhidrosis, hypotrichosis and onychodystrophy, as well as other, often variable, ectodermal developmental anomalies (Schöpf et al., 1971; Monk et al., 1992). SSPS shows clinical overlap with odonto-onychodermal dysplasia (OODD), but the eyelid cysts are a typical sign of SSPS. Some features may not present until adulthood and diagnosis can be delayed (Granger et al., 2012). The presence of ectodermal abnormalities in some carriers can lead to confusion in the mode of inheritance (Craigen et al., 1997). Eyelid cysts (apocrine hidrocystomas) that can also extend to the peri-ocular regions and nasal bridge. Atlas Genet Cytogenet Oncol Haematol. 2012; 16(12) 940 Schöpf-Schulz-Passarge syndrome (SSPS) McGrath JA p.Arg248X, and p.Cys376X), nine missense mutations (p.Ile116Thr, p.Arg128Gln, p.Ala131Thr, p.Ala131Val, p.His143Tyr, p.Val145Met, p.Phe228Ile, p.Gly266Cys, and p.Arg360Cys) and one frameshift mutation (p.Glu52fsX29) (Adaimy et al., 2007; Bohring et al., 2009; Nagy et al., 2010; Wedgeworth et al., 2011; van Geel et al., 2010; Catori et al., 2011; Cluzeau et al., 2011; Petrof et al., 2011; Granger et al., 2012). Of note, cases classified clinically as SSPS or OODD may harbour the same WNT10A gene mutation(s). The two most frequently observed mutations are p.Cys107X and p.Phe228Ile. Moreover, homozygous or compound heterozygous mutations involving p.Cys107X have been found in both SSPS and OODD, demonstrating that these two disorders are indeed allelic and that the precise phenotypic consequences are influenced by more than just this particular mutation in WNT10A alone. There is no genotype-phenotype correlation with regard to neoplastic risk. Neoplastic risk The neoplastic risk in SSPS is controversial. Some authors consider that SSPS can be associated with an increased risk of benign as well as malignant skin tumours (Monk et al., 1992). Reports include an increased incidence of benign adnexal tumours, such as eyelid hidrocystomas or eccrine syringofibroadenomas (Starink, 1997), and possibly a higher risk of malignant skin tumours such as squamous cell carcinoma, basal cell carcinoma and eccrine porocarcinoma (Bohring et al., 2009; Monk et al., 1992; Starink, 1997). Treatment There is no effective treatment for SSPS. Hyperhidrosis of the palms may respond partially to tap water iontophoresis (although use of anti-cholinergics may induce excessive systemic side-effects such as dry mouth, dizziness and drowsiness). Systemic retinoids can exacerbate skin peeling, although low doses may help some individuals. The apocrine hidrocystomas can be improved by electrocautery. Regular skin examination to detect non-melanoma skin cancer may be advisable. Regular dental care/surgery is indicated in most cases. Hair/nail cosmesis may help some individuals. Psychological support should be offered, as necessary. To be noted Note It is also noteworthy that individuals who are heterozygous for WNT10A mutations may show some clinical abnormalities. Hair, nail, teeth and skin abnormalities may all occur in heterozygotes; this probably accounts for the initial difficulties in classifying SSPS/OODD as either autosomal dominant or autosomal recessive disorders (the latter is correct). The mutation p.Phe228Ile appears to have a population frequency of ~0,5% and it has been estimated that approximately half of all individuals who are heterozygous for this missense mutation will manifest some form of ectodermal defects (Bohring et al., 2009). This equates to ~1 in 400 of the general population displaying some clinical anomaly affecting hair, teeth, nails, sweat glands, or a combination thereof, as a direct consequence of this WNT10A gene sequence variant. Evolution Many of the features of ectodermal dysplasia only manifest or worsen during adulthood. In some individuals with SSPS, the apocrine hidrocystomas tend to become larger and more numerous with age. Prognosis Life expectancy is normal; the main challenge is the symptomatic management of whichever ectodermal pathologies cause the patient the most concern. Genes involved and proteins WNT10A Location 2q35 Note WNT10A is a key signalling molecule that regulates cell-cell interactions and which is involved in multiple developmental processes in embryogenesis. In adult tissues it inhibits the β-catenin degradation complex and is involved in hair follicle and tooth morphogenesis (Logan and Nusse, 2004). Mutations Note Mutations in WNT10A underlie SSPS, OODD and some cases of hypohidrotic ectodermal dysplasia. Thus far, 16 different WNT10A mutations have been reported. These include six nonsense mutations (p.Trp9X, p.Cys107X, p.Arg128X, p.Glu233X, Atlas Genet Cytogenet Oncol Haematol. 2012; 16(12) References Schöpf E, Schulz HJ, Passarge E. Syndrome of cystic eyelids, palmo-plantar keratosis, hypodontia and hypotrichosis as a possible autosomal recessive trait. Birth Defects Orig Artic Ser. 1971 Jun;7(8):219-21 Monk BE, Pieris S, Soni V. Schöpf-Schulz-Passarge syndrome. Br J Dermatol. 1992 Jul;127(1):33-5 Craigen WJ, Levy ML, Lewis RA. Schöpf-Schulz-Passarge syndrome with an unusual pattern of inheritance. Am J Med Genet. 1997 Aug 8;71(2):186-8 Starink TM. Eccrine syringofibroadenoma: multiple lesions representing a new cutaneous marker of the Schöpf syndrome, and solitary nonhereditary tumors. J Am Acad Dermatol. 1997 Apr;36(4):569-76 Logan CY, Nusse R. The Wnt signaling pathway in development and disease. Annu Rev Cell Dev Biol. 2004;20:781-810 941 Schöpf-Schulz-Passarge syndrome (SSPS) McGrath JA Adaimy L, Chouery E, Megarbane H, Mroueh S, Delague V, Nicolas E, Belguith H, de Mazancourt P, Megarbane A. Mutation in WNT10A is associated with an autosomal recessive ectodermal dysplasia: the odonto-onycho-dermal dysplasia. Am J Hum Genet. 2007 Oct;81(4):821-8 Cluzeau C, Hadj-Rabia S, Jambou M, Mansour S, Guigue P, Masmoudi S, Bal E, Chassaing N, Vincent MC, Viot G, Clauss F, Manière MC, Toupenay S, Le Merrer M, Lyonnet S, Cormier-Daire V, Amiel J, Faivre L, de Prost Y, Munnich A, Bonnefont JP, Bodemer C, Smahi A. Only four genes (EDA1, EDAR, EDARADD, and WNT10A) account for 90% of hypohidrotic/anhidrotic ectodermal dysplasia cases. Hum Mutat. 2011 Jan;32(1):70-2 Bohring A, Stamm T, Spaich C, Haase C, Spree K, Hehr U, Hoffmann M, Ledig S, Sel S, Wieacker P, Röpke A. WNT10A mutations are a frequent cause of a broad spectrum of ectodermal dysplasias with sex-biased manifestation pattern in heterozygotes. Am J Hum Genet. 2009 Jul;85(1):97-105 Petrof G, Fong K, Lai-Cheong JE, Cockayne SE, McGrath JA. Schöpf-Schulz-Passarge syndrome resulting from a homozygous nonsense mutation, p.Cys107X, in WNT10A. Australas J Dermatol. 2011 Aug;52(3):224-6 Nagy N, Wedgeworth E, Hamada T, White JM, Hashimoto T, McGrath JA. Schöpf-Schulz-Passarge syndrome resulting from a homozygous nonsense mutation in WNT10A. J Dermatol Sci. 2010 Jun;58(3):220-2 Wedgeworth EK, Nagy N, White JM, Pembroke AC, McGrath JA. Intra-familial variability of ectodermal defects associated with WNT10A mutations. Acta Derm Venereol. 2011 May;91(3):346-7 Van Geel M, Gattas M, Kesler Y, Tong P, Yan H, Tran K, Steijlen PM, Murrell DF, Van Steensel MA. Phenotypic variability associated with WNT10A nonsense mutations. Br J Dermatol. 2010 Jun;162(6):1403-6 Granger RH, Marshman G, Liu L, McGrath JA. Late diagnosis of ectodermal dysplasia syndrome. Australas J Dermatol. 2012 Jun 4; Castori M, Castiglia D, Brancati F, Foglio M, Heath S, Floriddia G, Madonna S, Fischer J, Zambruno G. Two families confirm Schöpf-Schulz-Passarge syndrome as a discrete entity within the WNT10A phenotypic spectrum. Clin Genet. 2011 Jan;79(1):92-5 Atlas Genet Cytogenet Oncol Haematol. 2012; 16(12) This article should be referenced as such: McGrath JA. Schöpf-Schulz-Passarge syndrome (SSPS). Atlas Genet Cytogenet Oncol Haematol. 2012; 16(12):940-942. 942