Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropharmacology wikipedia , lookup
Drug discovery wikipedia , lookup
Cell encapsulation wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Theralizumab wikipedia , lookup
Discovery and development of tubulin inhibitors wikipedia , lookup
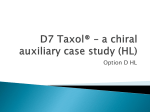
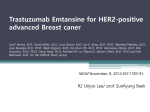
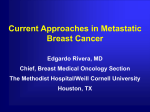
Drug Deliv. and Transl. Res. (2011) 1:420–428 DOI 10.1007/s13346-011-0042-2 RESEARCH ARTICLE Paclitaxel- and lapatinib-loaded lipopolymer micelles overcome multidrug resistance in prostate cancer Feng Li & Michael Danquah & Saurabh Singh & Hao Wu & Ram I. Mahato Published online: 25 October 2011 # Controlled Release Society 2011 Abstract Paclitaxel is a potent chemotherapeutic agent for treating refractory prostate cancer. However, its prolonged treatment develops multidrug resistance. Since lapatinib interacts with and inhibits P-gp activity, our objective was to determine whether the combination therapy of these two drugs can synergistically treat resistant prostate cancer. Our recently synthesized lipopolymer, poly(ethylene glycol)block-poly(2-methyl-2-carboxylpropylene carbonate-graftdodecanol) (PEG–PCD), was used to efficiently load both drugs into PEG–PCD micelles since they are hydrophobic. Lapatinib inhibited P-gp function but not its expression. Co-treatment of DU145-TXR cells with 0.5 μM paclitaxel and 5 μM lapatinib resulted in up to 138-fold reversal compared to paclitaxel alone. These formulations killed almost 70% and 80% of DU145-TXR cells when 0.5 μM paclitaxel was combined with lapatinib at a dose of 1 and 5 μM, respectively, while monotherapy had no effect. Combination therapy induced apoptosis and cell cycle arrest at mitotic phase. Xenograft tumor growth in athymic nude mice was significantly regressed when PEG–PCD micelles carrying lapatinib and paclitaxel were given intravenously twice a week. Furthermore, this combination therapy synergistically decreased antiangiogenic activity compared to the control or their monotherapy. In conclusion, lipopolymeric micelles carrying lapatinib and paclitaxel have the potential to treat resistant prostate cancer and can successfully deliver drugs to tumors while minimizing toxic effects associated with solubilizing agents. F. Li : M. Danquah : S. Singh : H. Wu : R. I. Mahato (*) Department of Pharmaceutical Sciences, University of Tennessee Health Science Center, 19 S Manassas, CRB 224, Memphis, TN 38103-3308, USA e-mail: [email protected] URL: http://www.uthsc.edu/pharmacy/rmahato Keywords Lipopolymer . Prostate cancer . Lapatinib . Paclitaxel . Multidrug resistance Introduction Prostate cancer is the second common male cancer in the USA. Although the majority of patients respond well to androgen ablation therapy, chemotherapy, and radiotherapy at the beginning, many patients relapse over time and become resistant to chemotherapy [1, 2]. This is mainly due to the over-expression of multiple drug-resistant (MDR) transporters in prostate cancer cells (Fig. 1). These transporters, such as P-glycoprotein (P-gp), breast cancer resistance protein, and multiple drug resistance protein, increase drug efflux and reduce drug accumulation in tumor cells [3–5]. The prognosis of patients with MDR cancer is poor, due to the lack of effective clinical interventions. Also, many commonly used chemotherapy drugs such as paclitaxel have inherent toxicity associated with their use. Thus, there is an urgent need for effective therapies for MDR prostate cancers while reducing the side effects associated with the drug or its delivery mechanism. Several strategies have been used to overcome MDR, including developing of novel anticancer agents [6] using novel delivery systems, such as liposomes [7], solid lipid nanoparticles [8], polymer–drug conjugates [9], and the use of MDR transporter inhibitor [10]. Lapatinib is a dual tyrosine kinase inhibitor what targets both human epidermal growth factor receptor (EGFR) and epidermal growth factor receptor 2 (HER2). Lapatinib blocks autophosphorylation reaction and the downstream of events. Lapatinib was approved by the FDA for treating advanced breast cancers [11]. Studies indicate that lapatinib can inhibit the function of ATP-binding cassette (ABC) Drug Deliv. and Transl. Res. (2011) 1:420–428 421 Lapatinib Resistance MDR transporters Sensitization Paclitaxel Fig. 1 Schematic diagram showing paclitaxel and lapatinib combination therapy for treating MDR cancer transporters and thus sensitize MDR cancer cells to chemotherapeutic agents (Fig. 1) [12–14]. Lapatinib has also been reported to decrease the percentage of cancer stem cells and improved the long-term survival of patients [15]. Moreover, several studies have demonstrated the potential of lapatinib for treating prostate cancer. For example, Liu et al. have shown that inhibiting HER2 using lapatinib is capable of disrupting androgen function in prostate cancer [16]. Also, Shaw and coworkers elegantly demonstrated targeting of Hedgehog-ErbB signaling using cyclopamine and gefitinib or lapatinib inhibited proliferation of androgen-independent prostate cancer cells [17]. Additionally, it is noteworthy that lapatinib is currently being evaluated in phase II clinical trial for the treatment of early stage hormone-dependent or metastatic prostate cancer [18]. Phase III clinical trials using combination of lapatinib and paclitaxel have significantly improved clinical outcomes in HER-2-positive breast cancer patients [19]. This addition of lapatinib allows the use of a lower dose of chemotherapeutic drug which can reduces the toxic side effects of therapy. Polymeric micelles are prepared from amphiphilic diblock copolymers and used for hydrophobic drug delivery. It forms a core–shell structure by self-assembly. The hydrophobic core of micelles is capable of loading hydrophobic drugs and thus avoids the use of toxic solubilizing agents in the delivery of poorly soluble anticancer drugs [20, 21]. The stealth properties associated with hydrophilic PEG corona of micelles prevent their aggregation, restrict plasma protein adsorption, prevent recognition by the reticuloendothelial system, and minimize rapid elimination from the bloodstream. The small size of micelles ensures their accumulation preferentially in the tumor via effective permeation and retention effects [22, 23]. For targeted delivery of drugs into tumors, the micelles need to be stable in the blood circulation. The stability of micelles can be improved through the engineering of the hydrophobic core. In our previous study, we designed a lipopolymer poly(ethylene glycol)-block-poly(2-methyl-2carboxylpropylene carbonate-graft-dodecanol) (PEG–PCD) for micellar drug delivery. This lipopolymer showed significantly improved stability and good drug loading for many poorly soluble drugs [5]. In the current study, we used lipopolymer PEG–PCD micelles to formulate lapatinib and paclitaxel. Firstly, we optimized the micelle formulation and characterized the formulation with analytical and biophysical methods. Then, the anticancer effects of lapatinib- and paclitaxel-loaded micelles were determined with in vitro cell-based assays, focusing on their effects to overcome MDR in prostate cancers. We also tested their abilities to inhibit MDR tumor growth in vivo with athymic mice xenograft tumor models established with MDR prostate cancer cells. Our aim in this study is to replace the use of commonly used solubilizing agents such as DMSO and Cremaphor-EL which are known to induce cellular and organ toxicity. Materials and methods Materials Hydroxybenzotriazole, 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide, dodecanol, triethylamine, 1,8-diazabicyclo [5.4.0]undec-7-ene (DBU), 2,2-bis(hydroxymethyl) propionic acid, methoxypoly(ethylene glycol) (mPEG; Mn = 5,000, PDI=1.03) and all other reagents were purchased from Sigma Aldrich (St. Louis, MO, USA) and used as received. DU145-TXR cells were provided by Professor Evan T. Keller of the University of Michigan. Synthesis of poly(ethylene glycol)-block-poly(2-methyl-2carboxyl-propylene carbonate-graft-dodecanol) PEG–PCD was synthesized as described previously [24]. Firstly, poly(ethylene glycol)-block-poly(2-methyl2-benzoxycarbonyl-propylene carbonate) (PEG–PBC) was synthesized through a ring-opening polymerization from monomer MBC, using mPEG as a macro-imitator and DBU as a catalyst. Then, protective benzyl groups in PEG–PBC was removed by hydrogenation to get poly (ethylene glycol)-block-poly(2-methyl-2-carboxyl-propylene carbonate) (PEG–PCC). Finally, lipopolymer PEG–PCD was obtained after conjugation of dodecanol lipid pendant groups to PEG–PCC. Lipopolymers and intermediate polymers were characterized with following methods: (1) nuclear magnetic resonance (NMR). 1H NMR spectra were recorded on Varian (500 MHz) using deuterated chloroform (CDCl3) as a solvent unless otherwise noted. The chemical shifts were 422 calibrated using tetramethylsilane as an internal reference and given in parts per million; (2) gel permeation chromatography (GPC). The weight (Mw) and number (Mn) average molecular weight and polydispersity index of synthesized polymers were determined by a Waters GPC system equipped with a GPC column (AM Gel 103/5) and a differential refractive index detector. THF was used as an eluent at a flow rate of 1 mL/min. A series of narrow polystyrene standards (700–40,000 g/mol) were used for calibration. Preparation and characterization of lipopolymeric micelles Lipopolymer micelles were prepared with a film dispersion method as previously described with some modifications [6]. Briefly, 30 mg of lipopolymers and given amount of drugs were dissolved in 0.5 mL CH2Cl2, before the solvent was removed under reduced pressure. The resulting film was hydrated in 3 mL saline (0.9%) and sonicated for 1 min. The residual free drug was removed by centrifugation at 12,000 rpm for 5 min. The supernatant was filtered using a 0.22-μM filter. Whenever we used both paclitaxel and lapatinib, they were co-dissolved for drug loading in the same micelles. The particle size distribution of micelles was determined by dynamic light scattering with Malvern Nano ZS. To determine drug loading, 10 μL of drug-loaded micelle solution was dissolved with acetonitrile and the drug concentration determined using a reverse-phase high performance liquid chromatography (RP-HPLC; Waters, Milford, MA, USA) with a UV detector at 227 nm. A C18 column (250×4.6 mm, Alltech, Deerfield, IL, USA) was used. The mobile phase was composed of 50:50 V/V water and acetonitrile at 1 mL/min. Lapatinib and paclitaxel concentration was calculated based on peak area. MTT assay Drug-resistant prostate cancer cell DU145-TXR was used to determine the cell growth inhibition ability of drugloaded micelles. Cells were cultured in DMEM media supplemented with 10% fetal bovine serum and 1% antibiotic–antimycotic at 37°C in humidified environment of 5% CO2. Cells were seeded in 96-well plates at a density of 5,000 cells per well before treatment with drug-loaded micelles as indicated. At the end of treatment, cell culture medium was replaced by 100 μL medium with 0.5 mg/mL 3-(4,5-dimethyl-thiazol-2-yl)-2, 5-diphenyl tetrazolium bromide (MTT) and incubated for 1 h at 37°C. Then, the medium was removed and 200 μL of DMSO was added into each well to dissolve the formazan crystals. The absorbance was measured in a microplate reader at a wavelength of 560 nm. Cell viability was expressed as Drug Deliv. and Transl. Res. (2011) 1:420–428 the percentage of control group. Cell viability (%)= (Atest/Acontrol)×100%. DMSO controls were included in all experiments where it was used to solubilize paclitaxel and lapatinib. Calcein AM assay Cells were seeded into a black wall clear bottom 96-well plate at a density of 20,000 cells per well a day before experiment. After treating cells with various concentrations of test compounds in 50 μL Dulbecco’s phosphate buffered saline (DPBS) for 20 min at 37°C, 50 μL calcein AM (10 μM) in DPBS were added to each well and incubated at 37°C for additional 20 min. Fluorescent intensity in each well was determined using a SpectraMax M2/M2e spectrofluorometer (Sunnyvale, CA, USA) at the excitation wavelength of 494 nm and emission wavelength of 517 nm. Propidium iodide staining and cell cycle analysis Cells were cultured in a 24-well plate to 90% confluence and then treated for 24 h. Cells were trypsinized and fixed in 70% ice-cold ethanol. After washing with PBS containing RNAse (1 mg/mL), cell pellet was re-suspended in 5 μg/mL propidium iodide staining solution for 15 min at the room temperature. Cell cycle distribution was measured by flow cytometry (Becton, Dickinson, NJ, USA). Results from 10,000 fluorescent events were obtained for analysis. TUNEL assay TdT-mediated dUTP nick-end labeling (TUNEL) assay was performed using DeadEnd Fluorometric TUNEL System (Promega, Madison, WI, USA). Briefly, DU145-TXR cells were grown on Lab-tek chamber slide and treated with lapatinib, paclitaxel, and their combination for 24 h. At the end of treatment, cells were fixed with acetone at −20°C for 10 min, washed with PBS, and equilibrated with buffer at the room temperature for 10 min. Then, it was incubated with a staining agent, composed of nucleotide and rTdT, in a humidified chamber at 37°C for 1 h and protected from light. The reaction was terminated with 2× standard sodium citrate buffer and washed with PBS to remove unincorporated fluorescein-12-dUTP. The washed specimens were then counterstained with 4′, 6-diamidino-2-phenylindole (DAPI) and visualized with Zeiss AxioVision fluorescent microscope. In vivo anticancer efficacy study All animal experiments were performed in accordance with the NIH animal use guidelines and the protocol approved by the Animal Care and Use Committee at the University of Drug Deliv. and Transl. Res. (2011) 1:420–428 423 Tennessee Health Science Center. Xenograft flank tumors were established in 8-week-old male athymic nude mice (Charles River) by subcutaneous injection of five million DU145-TXR prostate cancer cells suspended in 1:1 media and matrigel. When tumors reached approximately 100 mm3, mice were randomized and assigned to different treatments. PEG–PCD micelles containing both lapatinib and paclitaxel were injected twice a week at the dose of 5 mg/kg each as a combination therapy via the tail vain injection. For the monotherapy, micelles carrying either lapatinib or paclitaxel were also injected at the dose of 10 mg/kg. Tumors were measured with a caliper prior to each injection, and their volumes were calculated using the formula: (width2 ×length)/2. At the end of study, tumor tissue was excised from the mice and weighed. Results Effect of lapatinib and paclitaxel on MDR prostate cancer cells To determine whether lapatinib can reverse MDR in prostate cancer cells, paclitaxel resistant prostate cancer cells DU145-TXR were treated with the combination of paclitaxel and lapatinib. As shown in Fig. 2, the IC50 of paclitaxel was 2,069±597 nM in the absence of lapatinib, indicating DU145-TXR cells were resistant to paclitaxel. However, the IC50 of paclitaxel decreased to 79±29 nM at lapatinib concentration of 1 μM and to 15±8 nM at lapatinib concentration of 5 μM. These results suggest that lapatinib can sensitize DU145-TXR to paclitaxel. This study proved the feasibility of using lapatinib and paclitaxel combination to overcome MDR in prostate cancers. Viable Cells (%) 120 100 Preparation and characterization of drug-loaded lipopolymer micelles PEG–PCD lipopolymer were synthesized as described previously [5]. The synthesized PEG–PCD lipopolymer were characterized with 1H NMR, GPC. The Mn calculated based on 1H NMR is 11,560. We also used GPC to determine the apparent Mn and Mw of lipopolymer PEG– PCD, which was 10,800 and 14,986, respectively. To determine paclitaxel and lapatinib loading efficiency into PEG–PCD lipopolymer micelles, drug concentration in the formulations was determined by HPLC after dissolving the drug-loaded micelles with acetonitrile. Due to the different retention time for paclitaxel (4.7 min) and lapatinib (7.1 min), we could simultaneously determine their concentrations (Fig. 3a). We first tested the ability of PEG–PCD micelles to load a single drug, either paclitaxel or lapatinib. As shown in Fig. 3b, c, both these drugs could be effectively loaded into lipopolymer micelles. For both paclitaxel and lapatinib, the final drug concentration in the formulation increased from around 0.5 to 2 mg/mL with increase in theoretical loading (weight ratio of initial drug/ polymer) from 5% to 20%. The drug loading efficiency was almost 100%, indicating all the drugs can be effectively loaded into micelles at this range. As shown in Fig. 3d, we could simultaneously load both paclitaxel and lapatinib into PEG–PCD micelles and reach final drug concentration to at least 1 mg for each drug. The drug loading efficiencies were also around 100% for both drugs in all of these three formulations. The particle size of PEG–PCD was approximately 60 nm for all the tested formulations, and the incorporation of drugs had almost no effect on particle size and the inhibition of MDR prostate cancer cell proliferation by paclitaxel- and lapatinib-loaded lipopolymer micelles. Effect of drug-loaded PEG–PCD micelles on DU145-TXR cells PTX PTX+LAPA 1µM 80 PTX+LAPA 5µM 60 40 20 0 0 500 1000 1500 2000 PTX nM PTX PTX + 1µM LAPA PTX+ 5µM LAPA IC50 SD (nM) 2069 597 79 29 15 8 fold reversal 26.2 138.0 Fold of reversal = IC 50, no Lapatinib / IC50, with Lapatinib Fig. 2 Effect of lapatinib on reversing MDR in DU145-TXR cells. Percentage of viable cells was determined by MTT assay at 48 h post-treatment. Data are the means±SD (n=4). Fold of reversal= IC50, no lapatinib/IC50, with lapatinib. PTX paclitaxel, LAPA lapatinib The anticancer effect of paclitaxel- and lapatinib-loaded PEG–PCD micelles were tested in vitro on MDR prostate cancer cells DU145-TXR (Fig. 4). No obvious toxicity was observed in cells treated with blank micelles, lapatinib (2 μM) or paclitaxel (0.5 μM) alone for 48 h, while the combination of lapatinib (2 μM) and paclitaxel (0.5 μM) significantly reduced the cell viability to around 23% of the control group. The combination of lapatinib (1 μM) and paclitaxel (0.25 μM) also showed significant inhibition of DU145-TXR cell proliferation, with the cell viability of 35% of the control group. These results further confirmed that lapatinib and paclitaxel-loaded PEG–PCD micelles can overcome MDR in prostate cells and effectively inhibit the proliferation of resistant prostate cancer cells in vitro. 424 Drug Deliv. and Transl. Res. (2011) 1:420–428 A B 2 Concentration (mg/mL) 0.014 0.012 0.010 AU Fig. 3 Determination of drug concentrations in paclitaxeland/or lapatinib-loaded lipopolymer micelles. a HPLC chromatography of paclitaxel and lapatinib; b effect of theoretical loading on paclitaxel solubility; c effect of theoretical loading on lapatinib solubility; d drug concentration in paclitaxel and lapatinib co-loaded lipopolymer micelles 0.008 Lapatinib 0.006 0.004 0.002 Paclitaxel Paclitaxel 1.5 1 0.5 0 5 10 20 Theoretical Loading (%) 0.000 1 2 3 4 5 6 7 8 9 Retention time (Min) D Drug Concentration (mg/mL) C Concentration ( mg/mL) 2.5 2 Lapatinib 1.5 1 0.5 0 5 10 20 Theoretical Loading (%) Inhibition of P-gp activity in MDR cancer cells by lapatinib To determine whether lapatinib overcomes MDR in cancer cells, we performed calcein AM assay to determine the effect of lapatinib on P-gp activity [6]. The intracellular accumulation of calcein, which is a fluorescent P-gp substrate, was observed with a fluorescent microscope and also quantitatively determined by a spectrofluorometer. As shown in Fig. 5a, lapatinib treatment led to dose-dependent increase in intracellular calcein fluorescence. The fluorescent intensity increased with increase in lapatinib concentration from 0 to 20 μM. 120 2.5 Paclitaxel Lapatinib 2 1.5 1 0.5 0 Polymer (mg) Paclitaxel (mg) Lapatinib (mg) 10 0.5 0.5 20 1 1 10 1 1 We also quantitatively determined the fluorescent intensity with a spectrofluorometer (Fig. 5b). In the absence of lapatinib, the fluorescence intensity was approximately 50 RFU; however, it increased to around 800 RFU at a lapatinib concentration of 20 μM. In contrast, treatment with blank PEG–PCD micelles showed negligible effect on intracellular accumulation of calcein fluorescence. We next examined the effect of lapatinib on P-gp transport at the molecular level. From Fig. 5c, d, parent DU145 cells did not express MDR-1 and P-gp at detectable levels. In contrast, P-gp was overexpressed in DU145-TXR cells. Also, the treatment of DU145-TXR cells with 2 μM lapatinib for 24 h did not alter P-gp expression at both mRNA (Fig. 5c) and protein levels (Fig. 5d). Viable Cells (%) 100 Cell cycle and apoptosis of MDR prostate cancer cells 80 60 40 * 20 * 0 NT PEG-PCD LAPA 2µM PTX 0.5µM LAPA 2 µM LAPA 1µM PTX 0.5µM PTX 0.25µM Fig. 4 Anticancer effect of paclitaxel and lapatinib combination on MDR DU145-TXR cells. DU145-TXR cells were treated with micelles containing either lapatinib alone, paclitaxel alone, or combination of these two drugs for 48 h, and then cell viability was determined by MTT assay and expressed as a percentage of control. *p<0.01, compare with non-treated control (NT). PTX paclitaxel, LAPA lapatinib We also determined the effect of lapatinib- and paclitaxelloaded PEG–PCD micelles on DU145-TXR cells by analyzing cell cycle distribution and cell apoptosis by flow cytometry. Cells were treated with different formulations for 24 h before analysis. As shown in Fig. 6, the treatment of lapatinib (2 μM) or paclitaxel (0.5 μM) alone had no effects on the cycle distribution. In contrast, their combination showed significant effects on cycle distribution and cell apoptosis. The treatment of 2 μM lapatinib+0.5 μM paclitaxel caused cells in G0/G1 phase decreased from 29.0±2.1% in the control group to 4.7±0.2% in the Drug Deliv. and Transl. Res. (2011) 1:420–428 425 B 0 1 5 Lapatinib (µM) Fluorescence Intensity A 20 Lapatinib (µM) 1000 800 600 400 200 0 0 5 10 15 20 Lapatinib (µM) C 120 Control DU145 MDR -1 mRNA level (% of control) DU145-TXR LAPA MDR1 S19 100 80 60 40 20 0 Control LAPA DU145 DU145-TXR D DU145 DU145-TXR Control LAPA P-gp GAPDH Fig. 5 Effect of lapatinib on P-gp activity inhibition and expression. a Fluorescent images depicting dose-dependent increase in intracellular calcein fluorescence in DU145-TXR following treatment with lapatinib (2 μM). b Intracellular calcein accumulation in DU145 or DU145-TXR cells. c P-gp mRNA expression following treatment with 2 μM lapatinib for 24 h. d P-gp protein expression after 24 h treatment with 2 μM lapatinib. PTX paclitaxel, LAPA lapatinib combination group. Meanwhile, cells in G2/M phase increased from 50.7±4.0% in the control group to 61.1± 1.2% in the combination group. In addition, the apoptotic sub G1 phase cells increased from 0.4±0.2% in the control group to 25.1±2.5% in the combination group. These results indicated that the cells treated with lapatinib and paclitaxel combination therapy failed to undergo mitosis. This is consistent with the anticancer mechanism of A B G0/G1 G2/M S SubG1 70 ** 60 LAPA+PTX PTX LAPA Control % Cells 50 40 * 30 * 20 10 * 0 Fig. 6 Effect of paclitaxel and lapatinib combination on cell cycle and apoptosis of MDR prostate cancers. DU145-TXR cells were treated with PEG–PCD micelles formulated lapatinib (2 μM), paclitaxel (0.5 μM), and lapatinib (2 μM)+paclitaxel (0.5 μM). After 24 h Control LAPA PTX LAPA+PTX treatment, cell cycles were analyzed by flow cytometry after PI staining. a Cell cycle distribution; b quantitative analysis. *p<0.01; **p<0.05, compare with control. PTX paclitaxel, LAPA lapatinib 426 Drug Deliv. and Transl. Res. (2011) 1:420–428 paclitaxel, which is a microtubule inhibitor and can cause the arrest of the cell cycle at mitotic phase. The increased cell population in sub-G1 phase indicated that apoptotic cells were increased after treating with the combination therapy [25]. We also used TUNEL assay to further confirm that the combination of paclitaxel and lapatinib induced apoptosis in DU145-TXR cells. As shown in Fig. 7, neither paclitaxel (0.5 μM) nor lapatinib (2 μM) alone caused apoptotic cell death in DU145-TXR cells, while the combination of paclitaxel (0.5 μM) and lapatinib (2 μM) induced significant cell apoptosis. Effect of lapatinib and paclitaxel combination on tumor microvasculature Lapatinib- and paclitaxel-loaded lipopolymer micelles overcome MDR in vivo Discussion Encouraged by the in vitro anticancer effect of lapatiniband paclitaxel-loaded PEG–PCD micelles in MDR prostate cancer cells, we tested their ability to overcome MDR in vivo using athymic nude mouse xenograft model established with DU145-TXT MDR prostate cancer cells. When tumors reached approximately 100 mm3, mice were randomized into four groups of eight mice. Mice were treated with the tail vain injection of PEG–PCD micelles at a dose of 10 mg/kg paclitaxel as the monotherapy group or 5 mg/kg paclitaxel + 5 mg/kg lapatinib in the combination therapy group, respectively. In contrast to paclitaxel monotherapy, lapatinib and paclitaxel combination therapy significantly inhibited in vivo tumor growth (Fig. 8a). We also determined the weight of tumor at the end of the study, which also showed that the weight of tumors in the combination group was significantly less than those in paclitaxel monotherapy group. In addition, we did not observe any mortality and significant decrease body weight in mice after drug administration, indicating the negligible toxicity of PEG–PCD lipopolymer micelles used in this study (data not shown). A We examined the vessel density of xenograft tumors to determine the effect of lapatinib and paclitaxel combination on tumor neovascularization (Fig. 8b). While lapatinib treatment had some effect on angiogenesis, the combination of these two drugs strongly inhibited angiogenesis (less CD31-positive staining) compared to paclitaxel monotherapy or control. Hormone refractory prostate cancer is aggressive and resistant to prolonged treatment with paclitaxel and other chemotherapeutic agents due to the activity of cell surface drug transporters responsible for multidrug resistance. P-glycoprotein is one commonly overexpressed ABC transporters in a variety of MDR cancers including prostate cancer [26]. A promising approach to treat cancers overexpressing P-gp is to combine traditional chemotherapy drugs with P-gp inhibitors. Recently, various tyrosine kinase inhibitors including lapatinib have been shown to interact with and/or inhibit the activity of P-gp. Consequently, we hypothesize that co-administration of lapatinib and paclitaxel may potently kill MDR cancers since lapatinib will sensitize cells and potentiate paclitaxel activity. Our findings confirmed that lapatinib works by inhibiting P-gp function but not decreasing transporter expression since we observed dose-dependent increase in intracellular calcein fluorescence in DU145-TXR following treatment with lapatinib, but no effect on MDR-1 mRNA and P-gp protein levels. These results closely agree with the work of Dai et al. who showed similar results for MCF-7/adr cells [12]. Furthermore, Dunne and coworkers observed no B C TUNEL/DAPI Paclitaxel 0.5 µM TUNEL/DAPI Lapatinib 2 µM Fig. 7 Detection of paclitaxel and lapatinib combination induced cell apoptosis with TUNEL staining. Paclitaxel and lapatinib combination induced cell apoptosis in DU145-TXR Cells. DU145 cells were treated with a paclitaxel 0.5 μM, b lapatinib 2 μM, and c paclitaxel TUNEL/DAPI Paclitaxel 0.5 µM +Lapatinib 2 µM 0.5 μM+lapatinib 2 μM. After 24 h treatment, cells were subject to TUNEL staining and counterstained with DAPI. Images are overlay of green fluorescence from the TUNEL stain with blue fluorescence from DAPI Drug Deliv. and Transl. Res. (2011) 1:420–428 A 1500 427 B Control Tumor Volume (mm3) LAPA 10mg/Kg PTX 10mg/Kg 1000 LAPA 5mg/Kg + PTX 5mg/Kg 500 * * * 0 0 Injection 5 * * 10 15 20 Days Fig. 8 In vivo anticancer effect of paclitaxel- and lapatinib-loaded lipopolymer micelles on xenograft MDR prostate tumors. a Nude mice bearing 100-mm3 DU145-TXR tumors were given intravenous injection of PEG–PCD micelles containing lapatinib and paclitaxel were injected twice a week at a dose of 10 mg/kg for monotherapy and 5 mg/kg per drug for combination therapy. Tumor growth regression was significantly higher for combination therapy compared to monotherapy and control. Points are mean tumor size (n=8); bars, SE. b Tumor vessels for each treatment were stained with anti-CD31 antibody to assess antiangiogenic activity. PTX paclitaxel, LAPA lapatinib change in MDR1 mRNA levels upon treating A549-tax cells with increasing concentrations of lapatinib [26]. However, in contrast with our results (Fig. 5c, d), they observed a dose-dependent increase in P-gp protein levels which was attributed to posttranscriptional effects. Since we used similar doses of lapatinib in our study as Dunne et al., it is not clear what the underlying mechanistic differences are or whether these differences are merely cell line dependent. We developed paclitaxel- and lapatinib-loaded lipopolymer micelle formulations with high drug loading efficiency, small particle size (~60 nm) and narrow size distribution and performed in vitro cell-based studies to test our hypothesis. Paclitaxel (0.5 μM) and lapatinib (2 μM) combination effectively inhibited DU145-TXR cell proliferation in vitro, induced cell cycle perturbation, and increased cell apoptosis. In contrast, monotherapy with 0.5 μM paclitaxel or 2 μM lapatinib alone showed almost no effect on DU145-TXR cells. Co-administration of lapatinib and paclitaxel resulted in a 26and 138-fold reversal when lapatinib concentration increased from 1 to 5 μM. It is also noteworthy that decreasing the concentration of both drugs by 50% (i.e., 0.25 μM paclitaxel and 1 μM lapatinib) still resulted in a decrease in cell viability to approximately 30%. Our findings are supported by several in vitro data published in the literature. Coley et al. [27] have shown that the combination of GW282974A (lapatinib analog) and paclitaxel is synergistic in inhibiting proliferation of resistant ovarian cancer cell line (PEO1TaxR) [27]. Lapatinib has also been shown to increase cytotoxic activity of SN-38 and Topotecan in resistant glioblastoma, colorectal carcinoma, and ABCG2-transfected breast cancer cells [28]. Similar to in vitro study, the combination of 5 mg/kg paclitaxel and 5 mg/kg lapatinib significantly inhibited tumor growth in vivo compared with 10 mg/kg paclitaxel monotherapy (Fig. 8). These studies indicate that paclitaxeland lapatinib-loaded PEG–PCD lipopolymer micelles could be used to treat MDR prostate cancers. Since tumor growth requires formation of new blood vessels from pre-existing vessels, we hypothesized that combination of lapatinib and paclitaxel will be more potent compared to monotherapy in inhibiting angiogenic activity. To assess tumor vessel density, we performed immunohistochemical staining with anti-CD31 antibody. Our results suggest paclitaxel alone did not significantly alter microvessel density compared to control. In contrast, combined treatment with these two drugs appeared to be synergistic in decreasing antiangiogenic activity compared to the control or monotherapy. Although paclitaxel has been shown to exhibit antiangiogenic activity [29], our observations were different. This may possibly be due to the lower dose (10 vs 28 mg/kg) and paclitaxel resistant cells used in our study. Lapatinib is a selective and potent dual tyrosine kinase inhibitor of EGFR and HER2 and can stabilize tumor progression in monotherapy, a fact confirmed by our results in Fig. 8b. It also acts synergistically in combination with chemotherapy [30]. The antineoplastic activity of lapatinib and paclitaxel combination seen in our study suggests that at the concentrations used for the study, both inhibitions of angiogenesis as well as direct cytotoxic effects may be occurring. Further experiments to clarify the antineoplastic mechanisms and dysregulated signaling pathways involved in prostate tumors need to be carried out. Taken together our results confirm that the lipopolymer PEG–PCD successfully delivered a combination of lapatinib and paclitaxel to prostate cancer cells in vitro and in 428 vivo. Lapatinib reversed MDR in drug-resistant tumors and paclitaxel enhanced toxicity in P-gp overexpressing prostate cancer cells. Finally, our non-toxic lipopolymer described here avoids the use of solubilizing agents often required for formulating hydrophobic anticancer drugs, thereby avoiding any potential systemic or organ toxicity. Acknowledgments This work is supported by an Idea Award (W81XWH-10-1-0969) from the Department of Defense Prostate Cancer Research Program. References 1. Theyer G, Schirmbock M, Thalhammer T, Sherwood ER, Baumgartner G, Hamilton G. Role of the MDR-1-encoded multiple drug resistance phenotype in prostate cancer cell lines. J Urol. 1993;150(5 Pt 1):1544–7. 2. van Brussel JP, Mickisch GH. Multidrug resistance in prostate cancer. Onkologie. 2003;26(2):175–81. doi:10.1159/000071510. 3. Sanchez C, Mendoza P, Contreras HR, Vergara J, McCubrey JA, Huidobro C, et al. Expression of multidrug resistance proteins in prostate cancer is related with cell sensitivity to chemotherapeutic drugs. Prostate. 2009;69(13):1448–59. doi:10.1002/pros.20991. 4. Szakacs G, Paterson JK, Ludwig JA, Booth-Genthe C, Gottesman MM. Targeting multidrug resistance in cancer. Nat Rev Drug Discov. 2006;5(3):219–34. doi:10.1038/nrd1984. 5. Danquah MK, Zhang XA, Mahato RI. Extravasation of polymeric nanomedicines across tumor vasculature. Adv Drug Deliv Rev. 2011;63(8):623–39. doi:10.1016/j.addr.2010.11.005. 6. Li F, Lu Y, Li W, Miller DD, Mahato RI. Synthesis, formulation and in vitro evaluation of a novel microtubule destabilizer, SMART-100. J Control Release. 2010;143(1):151–8. doi:10.1016/j.jconrel.2009.12.028. 7. Rahman A, Husain SR, Siddiqui J, Verma M, Agresti M, Center M, et al. Liposome-mediated modulation of multidrug resistance in human HL-60 leukemia cells. J Natl Cancer Inst. 1992;84 (24):1909–15. 8. Dong X, Mattingly CA, Tseng MT, Cho MJ, Liu Y, Adams VR, et al. Doxorubicin and paclitaxel-loaded lipid-based nanoparticles overcome multidrug resistance by inhibiting P-glycoprotein and depleting ATP. Cancer Res. 2009;69(9):3918–26. doi:10.1158/ 0008-5472.CAN-08-2747. 9. Minko T, Kopeckova P, Pozharov V, Kopecek J. HPMA copolymer bound adriamycin overcomes MDR1 gene encoded resistance in a human ovarian carcinoma cell line. J Control Release. 1998;54(2):223–33. 10. Carcaboso AM, Elmeliegy MA, Shen J, Juel SJ, Zhang ZM, Calabrese C, et al. Tyrosine kinase inhibitor gefitinib enhances topotecan penetration of gliomas. Cancer Res. 2010;70(11):4499– 508. doi:10.1158/0008-5472.CAN-09-4264. 11. Medina PJ, Goodin S. Lapatinib: a dual inhibitor of human epidermal growth factor receptor tyrosine kinases. Clin Ther. 2008;30(8):1426–47. doi:10.1016/j.clinthera.2008.08.008. 12. Dai CL, Tiwari AK, Wu CP, Su XD, Wang SR, Liu DG, et al. Lapatinib (Tykerb, GW572016) reverses multidrug resistance in cancer cells by inhibiting the activity of ATP-binding cassette subfamily B member 1 and G member 2. Cancer Res. 2008;68 (19):7905–14. doi:10.1158/0008-5472.CAN-08-0499. 13. Kuang YH, Shen T, Chen X, Sodani K, Hopper-Borge E, Tiwari AK, et al. Lapatinib and erlotinib are potent reversal agents for MRP7 (ABCC10)-mediated multidrug resistance. Biochem Pharmacol. 2010;79(2):154–61. doi:10.1016/j.bcp.2009.08.021. Drug Deliv. and Transl. Res. (2011) 1:420–428 14. Collins DM, Crown J, O’Donovan N, Devery A, O’Sullivan F, O’Driscoll L, et al. Tyrosine kinase inhibitors potentiate the cytotoxicity of MDR-substrate anticancer agents independent of growth factor receptor status in lung cancer cell lines. Investig New Drugs. 2010;28(4):433–44. doi:10.1007/s10637-009-9266-0. 15. Li X, Lewis MT, Huang J, Gutierrez C, Osborne CK, Wu MF, et al. Intrinsic resistance of tumorigenic breast cancer cells to chemotherapy. J Natl Cancer Inst. 2008;100(9):672–9. doi:10.1093/jnci/djn123. 16. Liu Y, Majumder S, McCall W, Sartor CI, Mohler JL, Gregory CW, et al. Inhibition of HER-2/neu kinase impairs androgen receptor recruitment to the androgen responsive enhancer. Cancer Res. 2005;65(8):3404–9. doi:10.1158/0008-5472.CAN-04-4292. 17. Shaw G, Prowse DM. Inhibition of androgen-independent prostate cancer cell growth is enhanced by combination therapy targeting Hedgehog and ErbB signalling. Cancer Cell Int. 2008;8:3. doi:10.1186/1475-2867-8-3. 18. Sridhar SS, Hotte SJ, Chin JL, Hudes GR, Gregg R, Trachtenberg J, et al. A multicenter phase II clinical trial of lapatinib (GW572016) in hormonally untreated advanced prostate cancer. Am J Clin Oncol. 2010;33(6):609–13. doi:10.1097/COC.0b013e3181beac33. 19. Di Leo A, Gomez HL, Aziz Z, Zvirbule Z, Bines J, Arbushites MC, et al. Phase III, double-blind, randomized study comparing lapatinib plus paclitaxel with placebo plus paclitaxel as first-line treatment for metastatic breast cancer. J Clin Oncol. 2008;26 (34):5544–52. doi:10.1200/JCO.2008.16.2578. 20. Yamamoto T, Yokoyama M, Opanasopit P, Hayama A, Kawano K, Maitani Y. What are determining factors for stable drug incorporation into polymeric micelle carriers? Consideration on physical and chemical characters of the micelle inner core. J Control Release. 2007;123(1):11–8. 21. Leung SY, Jackson J, Miyake H, Burt H, Gleave ME. Polymeric micellar paclitaxel phosphorylates Bcl-2 and induces apoptotic regression of androgen-independent LNCaP prostate tumors. Prostate. 2000;44(2):156–63. 22. Maeda H, Wu J, Sawa T, Matsumura Y, Hori K. Tumor vascular permeability and the EPR effect in macromolecular therapeutics: a review. J Control Release. 2000;65(1–2):271–84. 23. Greish K, Nagamitsu A, Fang J, Maeda H. Copoly(styrene-maleic acid)-pirarubicin micelles: high tumor-targeting efficiency with little toxicity. Bioconjugate Chem. 2005;16(1):230–6. 24. Li F, Danquah M, Mahato RI. Synthesis and characterization of amphiphilic lipopolymers for micellar drug delivery. Biomacromolecules. 2010;11(10):2610–20. doi:10.1021/bm100561v. 25. Wang TH, Wang HS, Soong YK. Paclitaxel-induced cell death: where the cell cycle and apoptosis come together. Cancer. 2000;88 (11):2619–28. doi:10.1002/1097-0142(20000601)88:11. 26. Dunne G, Breen L, Collins DM, Roche S, Clynes M, O’Connor R. Modulation of P-gp expression by lapatinib. Investig New Drugs. 2010. doi:10.1007/s10637-010-9482-7. 27. Coley HM, Shotton CF, Ajose-Adeogun A, Modjtahedi H, Thomas H. Receptor tyrosine kinase (RTK) inhibition is effective in chemosensitising EGFR-expressing drug resistant human ovarian cancer cell lines when used in combination with cytotoxic agents. Biochem Pharmacol. 2006;72(8):941–8. doi:10.1016/j.bcp.2006.07.022. 28. Erlichman C, Boerner SA, Hallgren CG, Spieker R, Wang XY, James CD, et al. The HER tyrosine kinase inhibitor CI1033 enhances cytotoxicity of 7-ethyl-10-hydroxycamptothecin and topotecan by inhibiting breast cancer resistance protein-mediated drug efflux. Cancer Res. 2001;61(2):739–48. 29. Belotti D, Vergani V, Drudis T, Borsotti P, Pitelli MR, Viale G, et al. The microtubule-affecting drug paclitaxel has antiangiogenic activity. Clin Cancer Res. 1996;2(11):1843–9. 30. Steeghs N, Nortier JW, Gelderblom H. Small molecule tyrosine kinase inhibitors in the treatment of solid tumors: an update of recent developments. Ann Surg Oncol. 2007;14(2):942–53. doi:10.1245/s10434-006-9227-1.