Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
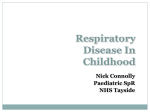
RESPIRATORY SYSTEM DR. REEM ALI Fall Semester 2015-2016 Functions of Respiratory System Taking in O2 and breathing out the CO2 Maintenance of acid-base balance Regulation of H2O and heat balance Production of speech Facilitate the sense of smell Respiratory system during childhood years infants are obligatory nasal breathers and they use their abdominal muscle for breathing Use more accessory muscles for breathing At 2yrs the Rt bronchus become shorter, wider & more vertical Walls of the airways are small in size and have less cartilage thus lung collapse after expiration is easier than in adult Assessment of Respiratory Function Inspection breathing: Rate Regularity Symmetry of movement Depth Effort and the use of accessory muscles (during sleep/quietly awake) Auscultation: airway patency & adventitious sounds Palpation & percussion: painful area and tissue density Normal breath sounds Bronchial sounds Over trachea, bronchi Loud, harsh and high pitched Longer in expiration Vesicular sounds Air moving in and out alveoli Quiet and low pitched Longer in inspiration Bronchovesicular sounds Near main stem bronchi Moderately pitched Equal in inspiration and expiration phases Adventitious sounds Crackles (Rales) Wheezes Result of air passing through fluid in small airways Simulated by rubbing a few strands of hair between fingers next to the ear Most common during inspiratory phase Associated with COPD and pulmonary edema Air passing through narrowed small airways In expiration Associated with asthma Pleural friction rub Pleural surfaces rubbing across each other Grating sound Associated with inflammation of the pleura Noisy Breathing Snoring Indicates partial obstruction of the upper airway that causes vibration of the air as it passes the nasopharynx and oropharynx May cause sleep apnea Stridor A harsh, continuous crowing sound Mostly occurs during inspiration Croup (Laryngotracheobronchitis) Wheezing Whistling/musical sound Indicates a narrowing of the airways Mainly heard during expiration Accompanied by tightness of the chest and labored breathing Mostly caused by asthma Respiratory Distress (RD) Clinical Manifestations Increased RR > 60 breath/min; Restlessness & apprehension Retractions: chest sinking with each breath mostly observed interiorly at lower costal margins (Subcostal retraction) Cyanosis around the mouth, fingernail Grunting during expiration Nasal flaring indicates labored breathing Wheezing & Cough Clubbing caused by chronic hypoxia Use of accessory muscles of respiration A child with RD should be kept NPO to Decrease the work of breathing and prevent aspiration Respiratory Distress (RD) Chest Retractions Nail Clubbing O2 therapy To treat hypoxemia Delivered by mask, nasal cannula, tent, hood, face tent or ventilator Should be ordered by physician Should be humidified before administered to the patient Therapeutic Techniques Aerosol /nebulizer therapy: used to administer medication and avoid systemic side effect Observe patient during aerosol therapy b/c it may cause bronchospasm Therapeutic Techniques Therapeutic Techniques Chest physiotherapy (CPT) When the children get a chest infection, the inability to take good deep breaths and cough forcefully may make the clearance of excess thick phlegm more difficult. This is when chest physiotherapy is useful CPT helps to clear the lungs and get the phlegm into the mouth where it can be spat out, or to the back of the throat where it can be swallowed CPT uses of postural drainage in adjunctive techniques including percussion, vibration, deep breathing & coughing exercise Therapeutic Techniques: Postural drainage Used to facilitate removing secretion from airways by gravity. Before meals but following other respiratory therapy 20-30 minutes Therapeutic Techniques: CPT Vibration used to move secretions during exhale Hand held vibrators Breathing exercises are used to help the child increase air entry into the lungs and enlarge the tracheobronchial tree Expiration after deep breaths carry out secretions and stimulate cough Blowing (pinwheel toy) stimulate deep breathing Cough exercise Children are encouraged to cough 1-2 after a deep breath Therapeutic Techniques: CPT Percussion This is when the child's chest is clapped gently with cupped hands to help shake the secretions loose. Most children find this quite soothing and effective, even though it may sound as it hurts. Respiratory Distress (RD) A child with RD should be kept NPO to Decrease the work of breathing and prevent aspiration Micro-organisms R/T Respiratory System Bacterial pathogens Bordetella pertussis (gram negative): pertussis or whooping cough Streptococcus pneumoniae (gram positive): sinusitis, otitis media and meningitis Haemophilus influenze (gram negative): acute meningitis, URTI (otitis media) Klebsiela pneumoniae (gram negative): pneumonia Mycobacterium tuberculosis: tuberculosis Pseudomonas aeruginosa (gram negative): hospital acquired infections, respiratory equipment can be source which cause sepsis, pneumonia and URTI Pharmacology R/T Respiratory System Disorders Bronchodilators reverse bronchoconstriction thus opening the air passages in the lungs by acting : Stimulating beta-adrenergic sympathetic nervous system receptors short acting beta agonists (ventolin); A quick relief of acute exacerbations and for the prevention of exercise-induced airway constriction.. long acting (Foradil) directly relaxing bronchial smooth muscles ( Aminophylline, Theophylline) Major Side Effect Dizziness (decrease in BP), CNS stimulation, Palpitation, GI irritation Pharmacology R/T Respiratory System Disorders Corticosteroids Anti-inflammatory effect Control Asthma and improve pulmonary function Inhaled preparation (Fluticasone) oral (Prednisone), IV (hydrocortisone) Major side effect Inhaled: oropharyngeal candiadiasis (fungal infection), growth retardation and osteoporosis Oral : with long-term use immunosuppression, increase Wt, osteoporosis, gastric ulcer, Pharmacology R/T Respiratory System Disorders Mucolytic Agents and Expectorants To liquefy secretions in the respiratory tract, thus promoting a productive cough Mucolytic directly breaking up mucous plugs (inhalation) Expectorants increase respiratory tract secretions (oral) Major side effect GI irritation Skin rash Oropharyngeal irritation Pharmacology R/T Respiratory System Disorders Antitussives To suppress the cough reflex Preparation with Narcotic (Codeine) without Narcotic (Tessalon) Major side effect Drowsiness Nausea Dry mouth (anticholingeric effect of antihistamine in combination products) Pharmacology R/T Respiratory System Disorders Antihistamines To relieve symptoms of common cold and allergies Act by blocking the action of histamine at receptor sites, also exert antiemetic, anticholinergic and CNS depressant effect Major side effect Drowsiness, GI Dizziness irritation Dry mouth (anticholingeric effect of antihistamine in combination products) Respiratory Dysfunction 1. Upper respiratory tract infections 2. Lower respiratory tract infections 3. Long-term respiratory dysfunction 4. Physical defects of respiratory tract 5. Foreign body Aspiration Respiratory Dysfunction Upper respiratory tract infections Otitis media Croup (laryngotracheobronchitis) Epiglottitis Respiratory Dysfunction: Otitis Media (OM) Acute infection of the middle ear Prevalent Caused between 6 months to 2 years.. by Streptococcus pneumonia or Haemophilus influenza Noninfectious caused by blocked Eustachian tube secondary to URI, allergy There is a relationship between formula-fed infants and OM Acute OM rapid short onset of signs and symptoms lasting for 3 weeks OM with effusion middle ear inflammation with fluid present Respiratory Dysfunction: Otitis Media (OM) Chronic OM may last more than 3 months Prolonged OM may have consequences: Functional: hearing loss which may affect speech, language and cognition development Structural: tympanic membrane retraction which leads to impaired sound transmission of the tympanic membrane); associated with the dramatic relief of pressure and pain Perforation (rupture Infection Respiratory Dysfunction: Otitis Media (OM) Clinical Manifestations Acute Pain: OM.. infant rubs ear or rolls head from side to side Temp. 40, Vomiting & diarrhea loss of appetite Tympanic membrane is bright red and bulging, no light reflex Discharge from the external auditory canal Respiratory Dysfunction: Otitis Media (OM) Clinical Manifestations OM with effusion No fever and No pain (mostly occurs after viral infection of URI) fullness in the ear Tympanic membrane gray and bulging After a few weeks-months fluid become thick (glue ear) causing possible loss of hearing Respiratory Dysfunction: Otitis Media (OM) Treatment Antibiotic, antipyretic, analgesic drugs Chronic OM: Nursing Diagnosis Pain; surgery ; insertion of tympanotomy tube Risk for injury; Altered family process Nursing care Assess pain, S&S of infection Provide comfort, prevent complications Educate family about treatment (ear drop) and complications possible Respiratory Dysfunction: Otitis Media (OM) Instillation of ear drops For the child under 3 years of age pull the auricle down & back For an older child, pull the auricle up and back Respiratory Dysfunction: Croup (Laryngotracheobronchitis (LTB)) Laryngotracheobronchitis (croup), refers to the inflammation or irritation of the larynx and trachea and bronchial passageways Mostly affect children under 5 years with peak between 6 months to 3 years Most common causative agents; parainfluenza virus Respiratory syncytial Influenza A &B virus virus (RSV) Respiratory Dysfunction: Croup (Laryngotracheobronchitis (LTB)) CM: Gradual onset and low grade fever Inspiratory stridor suprasternal retractions, barking cough and hoarseness .. Respiratory distress, possible hypoxia Respiratory acidosis Respiratory Dysfunction: Croup (Laryngotracheobronchitis (LTB)) Treatment Maintain patent airway, high humidity with cool mist (constrict edematous blood vessels) Ibuprofen NPO if there is respiratory distress and start IV fluid For sever cases Nebulized epinephrine or dexamethasone Possible intubation Respiratory Dysfunction: Croup (Laryngotracheobronchitis (LTB)) Nursing Care Observation and assessment of respiratory status Prepare for possible intubation if the patient develops signs of airway obstructions including: increased HR, RR, retractions, flaring nares increased restlessness Provide comfort, spasm) avoid eliciting gag reflex (Laryngo- Respiratory Dysfunction: Epiglottitis Acute obstructive inflammatory process of epiglottis Mostly occurs in children 2-6 years Most often the causative agent is Hemophilus influenza B Abrupt symptoms Respiratory Dysfunction: Epiglottitis CM sore throat and pain on swallowing fever, muffled voice Tripod & stridor, sit drooling saliva, irritable and restless & possible retraction epiglottis red, inflamed, large, cherry red and edematous airway obstruction leads to hypoxia and acidosis.. Respiratory Dysfunction: Epiglottitis Treatment IV fluid until the patient can swallow Antibiotic Corticosteroids to reduce the edema Tracheal Nursing intubation in severe cases Care Reduce the anxiety Comfortable position Avoid using tongue depressor to inspect epiglottius Monitor respiratory status Croup Epiglottitis Age 6 month- 3 year 2 yr- 6 yr Season Fall/winter Anytime Worst S/S Night and morning 24hrs History URI, gradual onset Sudden onset, no URI Fever Low-grade Med-high Drooling NO YES Cough YES NO Position Sitting, lying Tripod sit Stridor Inspir/ expiration Inspiration voice Hoarse Muffled Respiratory Dysfunction Lower respiratory tract infections Acute bronchitis Bronchiolitis/respiratory syncytial virus (RSV) Pneumonia Respiratory Dysfunction: Acute Bronchitis Inflammation of trachea , bronchi & bronchioles Common in children older than 6 yrs acute bronchitis usually occurs in association with viral respiratory tract infection.. Causative agent of acute bronchitis is Mycoplasma pneumonia (bacteria). Other causes include chemical agent Respiratory Dysfunction: Acute Bronchitis CM: productive cough sometimes retrosternal pain during deep.. breathing or coughing It is a self-limited disease (5-10 days) Treatment rest, use of antipyretics, adequate hydration Symptomatic treatment Respiratory Dysfunction: Bronchiolitis/Respiratory Syncytial Virus (RSV) Infection of the lower respiratory tract Rarely occurs in children over 2 years old (peak 2-5 months) Primarily occurs in winter & spring 50% of cases caused by RSV, bacteria also cause bronchiolitis The bronchi and bronchioles are inflamed that leads to obstruction of the airway Narrowing of the airways during expiration causes overinflation (emphyasema) Respiratory Dysfunction: Bronchiolitis/Respiratory Syncytial Virus (RSV) Starts with URT infection then spreads to lower tract CM; Earlier S&S; poor feeding and irritability Initial S &S; Rhinorrhea, low-grade fever, pharyngitis and possible OM, conjunctivitis, cough Progressive sign increased cough, air hunger, tachypnea, retractions & cyanosis Severe S&S, RR >70, listless, apneic spells Respiratory Dysfunction: Bronchiolitis/Respiratory Syncytial Virus (RSV) Symptomatically treatment antiviral medication may be used Humidity O2 Fluid & rest If the pt is tachypnea NPO Respiratory Dysfunction: Pneumonia Is an inflammation of pulmonary parenchyma Types of pneumonia based on the way the child gets the infection or the germ; Aspiration pneumonia; occurs when food or drink accidently gets into lungs Community Acquired pneumonia Most common type Caused by viruses, bacteria or chemical irritants Mostly occurs in winter and spring Respiratory Dysfunction: Pneumonia Fast breathing is a sign of pneumonia; 1 wk-2months 60 B/M or more 2mon- 12 mon 50 B/M or more 1 2months – 5 yrs 40 B/M or more Respiratory Dysfunction: Pneumonia The severity of pneumonia is classified based on: Not severe; Tachypnea only Severe pneumonia Wheezes stridor Retractions Cyanosis Nasal flaring Poor feeding convulsion Respiratory Dysfunction: Viral Pneumonia mostly caused by RSV in children under 5 yrs Gradual onset Viral infection make the pt susceptible to bacterial pneumonia Treatment is symptomatically O2 Comfort Fluid CPT Postural drainage Respiratory Dysfunction: Bacterial Pneumonia Streptococcus pneumonia is the most causative bacterium others causative agent; group B streptococcus, hemophilus influenza type b, group A streptococcus Abrupt onset CM: productive cough, tachypnea, fever, ronchi or fine crackles, chest pain, retraction, nasal flaring, cyanosis, lethargy Chest X-ray shows patchy infiltration Irritable Anorexia, vomiting, diarrhea and abdominal pain Respiratory Dysfunction: Bacterial Pneumonia Treatment Penicillin G ( for allergic pt erythromycin, chloramphenical, cephalosporin) Antipyretic, antitussive (cough) Rest Increase O2 fluid intake may be required for RD children Respiratory Dysfunction: Bacterial Pneumonia Nursing diagnosis: Ineffective breathing pattern R/T inflammatory effects of pneumonia Nursing Care Thorough respiration assessment (signs of Provide comfort and RD) O2, Cool humidification Encourage cough and deep breathing Increase fluid intake & Monitor I &O Provide rest & Maintain semi-fowler’s position Standard precautions & precautions use of air-borne and droplet Respiratory Dysfunction Long-term respiratory dysfunction Asthma Cystic fibrosis Respiratory Dysfunction: Asthma Chronic inflammatory disorder of the airway Asthma causes recurrent episodes of wheezing, breathlessness, chest tightness & cough particularly at night or in the early morning Associated with reversible airflow limitation or obstruction Asthma causes stimuli bronchial hyperresponsiveness to Respiratory Dysfunction: Asthma Factors aggravate asthmatic exacerbation Allergens (airpollution, dust), Irritants (odor spray, smoking) Changes in weather temperature, Cold air Environmental changes ( new home) Infections Animals Strong Food emotions additives, nuts, dairy product Other factors ( menses, pregnancy) Respiratory Dysfunction: Asthma The mechanisms responsible for the obstructive symptoms in asthma include: Inflammation and edema of the mucus membrane. Accumulation of tenacious secretions from mucus glands. Spasm of the smooth muscle of the bronchi and bronchioles, which decreases the diameter of bronchioles. Respiratory Dysfunction: Asthma CM: Asthmatic episode begins with: irritability, restlessness, headache, feeling tired Dyspnea Cough: hacking (harsh), irritative and nonproductive then cough becomes rattle & productive Prolonged expiratory phase with wheezing Flaring nares , distended neck veins Silent chest ( severe obstruction in status asthmaticus) Respiratory Dysfunction: Asthma Management Eliminate or avoiding irritant/ offending factors long-term control medication anti-inflammatory (Corticosteroids, Cromolyn sodium), bronchodilators (albuterol) Most long term or quick relief medications administered by inhaler CPT: relaxation and strengthen respiratory muscles Respiratory Dysfunction: Asthma Status Asthmaticus A severe prolonged asthma exacerbation that has not been broken with repeated doses of bronchodilators It is an emergency and may cause respiratory failure Symptoms Extreme difficulty in breathing, restlessness and anxiety Little or no breath sounds, inability to speak, cyanosis and heavy sweating Management by large doses of corticosteriod and bronchodilators, & O2 Asthma: Nursing Diagnosis Ineffective airway clearance R/T allergic response and inflammation Ineffective breathing pattern R/T bronchial edema, constriction and increased secretion Risk for suffocation R/T bronchospasm, edem and mucus secretion Activity intolerance R/T imbalance between O2 supply and demand Altered family process R/T having a child with chronic disease Risk for fluid volume deficit R/T insensible fluid loss ( hyperventilation & diaphoresis) & difficultly to take fluid, Risk for injury (respiratory acidosis & electrolyte imbalance) R/T hypoventilation and dehydration Asthma: Nursing Care Teaching Inhaler use Rinse mouth after use of Caution child the steroid inhaler & parent about overuse of inhaler Improve ventilation High fowler’s position Breathing exercise Regular exercise (swimming) Assess environmental Allergens infections triggering factor Cystic Fibrosis (CF) Cystic Fibrosis (CF) Autosomal recessive trait disorder affect Exocrine (mucus –producing) gland Involves abnormality in electrogenic chlroide channels and its regulations (abnormal transport of chloride and sodium across an epithelium causing thick secretions Increased viscosity of mucous gland secretions & mechanical obstruction is responsible for most clinical findings Sweat gland: high Na & Cl (3-5 times higher than normal) sweat chloride test above 60 mEq/L are diagnostic Cystic Fibrosis (CF) Cystic Fibrosis (CF) Early manifestations Meconium Baby ileus in newborn infants tastes salty Failure to regain normal 10% weight loss at birth Presence of cough or wheezing during first 6 months of age Sweat chloride test > 60mEq/L Chest X-ray shows patchy atelactesis Cystic Fibrosis (CF): Clinical Manifestations Respiratory tract Increased viscosity of bronchial mucus with incomplete expectoration causes obstruction and serves as a media for bacterial growth Dry nonproductive cough, Wheezing Hypoxia, hypercapnia and acidosis, clubbing of finger Barrel-shaped Obstruction Scattered chest and distended neck veins interfering with expiration (emphysema) atelectasis and emphysema Cystic Fibrosis (CF): Clinical Manifestations GI tract High thick secretion blocked the ducts in pancreas leading fibrosis Marked impairment of pancreatic enzymes which affects digestion of fats and protein thus affecting normal growth Pancreas: Becomes fibrotic, decrease production of pancreatic enzymes Decrease in Lipase cause steatorrhea (fatty, foul, bulky stool) Decrease in Trypsin increase nitrogen in stool Decrease Amylase cause inability to break down polysacharides Increased bulk of feces ( undigested and unabsorbed fat and protein) Wt loss & FTT High incidence of DM in children with CF Cystic Fibrosis (CF): Clinical manifestations Cardiovascular; Cardiac enlargement Rectal prolapse Liver; possible cirrhosis from biliary obstruction Reproductive Delayed puberty in females, mostly males are sterile Integumentary: salty taste, risk of hypochloremic and hyponatremic Cystic Fibrosis (CF) affect the whole body Cystic Fibrosis (CF) affect the whole body Cystic Fibrosis (CF): Treatment Pulmonary problems Chest physiotherapy Bronchodilators Antibiotic therapy as indicators Gastrointestinal problems Pancreatic enzyme supplements Balanced nutritional intake Cystic Fibrosis (CF): Nursing Diagnosis Ineffective airway clearance R/T secretion of thick tenacious mucus Ineffective breathing pattern R/T mechanical tracheobronchial obstruction Altered family process R/T situational crisis Altered nutrition R/T inability to digest nutrients Respiratory Dysfunction Physical defects of respiratory tract Esophageal atresia Tracheoesophageal fistula Diaphragmatic hernia Esophageal Atresia & Tracheoesophageal Fistula Esophageal Atresia & Tracheoesophageal Fistula Most common type proximal esophagus ends in a blind pouch and distal esophagus is connected to the trachea Usually occurs in low birth weight May be associated with other abnormalities Occurrence is 1 in 800 to 5000 births Esophageal Atresia & Tracheoesophageal Fistula Indications Excessive salivation (drooling) in newborn chocking, coughing, cyanosis (3 Cs) sneezing & when newborn fed the fluid returns through the nose and the mouth Complication: aspiration and RD Tx: surgical repair Nursing diagnosis Ineffective airway clearance R/T abnormal opening between esophagus Impaired swallowing Foreign Body Aspiration Risk for old infant and 1-3 years Most common foreign body: food (peanuts), balloon, coins CM: chocking, gagging, cough Laryngotracheal obstruction: dyspnea, cough, stridor, hoarseness, possible cyanosis Bronchial obstruction: paroxysmal cough (sudden severe attack), wheezing, asymmetric breathing sound, dyspnea Progressive obstruction: discoloration of the face , no voice , unconscious and asphyxiation Foreign Body Aspiration Management 5 (For infants) times Back blow 5 times Chest thrust Foreign Body Aspiration Management For a child Heimlich maneuver: short, abrupt pressure against the abdomen (between umbilicus and xiphoid) to raise the intrarespriratory pressure Foreign Body Aspiration Management If the infant is conscious tongue-jaw lift (look for object), ventilate, continue blows and chest thrusts call for CPR If the child is unconscious Lie the child on the floor, CAB (compressions, airway and breathing), look for object, ventilate, 5 abdominal thrusts Call for CPR