Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
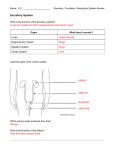
W507 – Basic human biology and target organs Respiratory System • Structure • The lung as a route of entry • The lung as a target organ – Particles – Gases • Occupational lung disease Respiratory System Structure Naso-pharynx (head airways) Nose, Mouth, Pharynx (throat) Tracheobronchial region Conducting airways in chest (trachea, bronchi, bronchioles) Alveolar region (deep lung) Gaseous exchange with blood (respiratory bronchioles, alveoli) Source: Tranter 1999 – reproduced with permission Naso-pharynx / head airways • Nose/Nasal Cavity (Turbinates) - Warms, moistens & filters air as inhaled. - Large, moist, ciliated surface, large blood supply • Mouth breathing – bypasses nasal filter • Pharynx (throat) Tracheo-bronchial region Structure: • • • • • Trachea (1) Main Bronchi (2) (Left & Right Lung) Bronchi (15 divisions) Bronchioles (10 divisions) Terminal Bronchioles With each division the total cross-sectional area increases – trachea 2cm2 – terminal bronchioles 80 cm2 • Flow rate decreases Lining of airway: • Lined with mucous membranes which are lined with cilia (small hairs) that can sweep trapped particles up to the throat (Mucociliary escalator) Alveolar Region Gas exchange occurs across the thin walls (one or two cell thickness) of the alveoli and respiratory bronchioles Alveoli • Air sacs surrounded by blood capillaries • Approximately 300-600 million alveoli with total surface area 100-200m2 • No cilia, so particles may remain within alveoli for long periods (months or even years) • Phagocytes (macrophage cells) travel throughout alveoli and may engulf and digest deposited particles Alveolar region – gas exchange • Thin barrier between air in alveoli and blood in pulmonary capillary (0.5um) • Allows rapid diffusion of: – O2 (alveoli to blood) – CO2 (blood to alveoli) • O2 is bound to haemoglobin inside red blood cell • Oedema (accumulation of fluid) increases thickness of barrier and impairs diffusion Particle deposition in the respiratory system • A particles ability to reach the deep lung depends on chemical and physical structure, including size, density and shape • Diameter is generally the most important factor that affects whether (and where) a particle will deposit in the respiratory system • Strictly speaking it is the ‘aerodynamic diameter’ rather than the diameter that is important Deposition Mechanisms: Particles • Interception: head airways Large particles (10-100 µm aerodynamic diameter) too large to penetrate the passages between the nasal hairs or the nasal turbinates • Impaction: head airways and divisions of large bronchi Large particles (5-30µm) fail to negotiate branches in airways and impact at speed on the airway wall Deposition Mechanisms: Particles • Sedimentation: small bronchioles and alveoli Smaller particles (1-5µm) follow the air stream, but eventually settle (sediment) out under their own weight due to gravity • Diffusion: alveoli Small particles (<1µ) remain suspended in the air stream and are often exhaled. Diffusion occurs in the alveoli where the airflow is negligible. Particles move at random (Brownian Motion) until they collide with the alveolar membranes Particle Clearance • Irritant receptors (nose & bifurcation of large bronchi) reflex sneezing, coughing, constriction of bronchi to limit further penetration • Mucociliary escalator (nasal passage and tracheobronchial tree) Particles trapped in mucous lining the airway. Moved by cilia to pharynx (throat) for swallowing • Macrophage (deep lung) Particles either engulfed and digested by macrophage then transported by lymphatic system to blood; Or, particles destroy macrophage – particles remain in lungs and bound in connective tissue ISO 7708: 1993 Curves • Inhalable fraction: % of particles that can enter the nose or mouth during breathing and is therefore liable to deposition anywhere in the respiratory tract. In practical terms maximum particle size is about 100 µm. • Respirable fraction: % of particles that can reach the deep lung (the alveolar region). Particle sizes of respirable dust generally up to 10 µm. • Alveolar deposition: Increases as particle size decreases; however, then decreases because a significant % of very small particles are exhaled immediately. Particle penetration & deposition: ISO 7708: 1993 curve Gases and vapours - lung as route of entry • Main risk from lipid soluble gases and vapours – pass through alveoli into blood – E.g. CO, H2S, mercury, organic vapours What features of the lung facilitate absorption? What effect does work rate have? Lung penetration by gases • Highly water soluble gases (e.g. ammonia, formaldehyde) only reach the upper respiratory tract – readily dissolve / absorb into moist mucous membranes • Penetration to deep lung increases if: – Exposure is high – Gas molecules are adsorbed onto particles • e.g. SO2 on soot particles • Less water soluble gases (e.g. phosgene) will tend to reach the deep lung The lung as a target organ • Irritation / Inflammation - Upper respiratory tract (URT) - Deep lung • Pneumoconioses - Fibrotic - Benign • Emphysema • Lung cancer • Respiratory sensitisation - Rhinitis Occupational asthma Extrinsic allergic alveolitis Byssinosis Acute Irritation / Inflammation • Upper Respiratory Tract - Coughing, irritation of mucous membranes – high exposures can cause release of fluid (oedema) - Irritant mists, fumes, dusts (e.g. chromium acid mists, metal oxide fumes, MMMF) - Highly water soluble gases (e.g. ammonia, hydrogen chloride) • Deep lung - Irritation of mucous membranes and pulmonary oedema - High exposure to many metal fumes (e.g. cadmium oxide which can cause an acute chemical pneumonitis) - Low water soluble gases (e.g. phosgene, nitrogen dioxide) Fibrotic pneumoconiosis Macrophage system • Very effective in removing most dust particles from lungs. • However in some situations macrophages are unable to engulf or remove the particle. • In these situations chemicals released from the macrophage can cause scarring (or fibrosis) which if widespread may be fatal. Examples include – – – – Coal worker’s pneumoconiosis (coal dust) Silicosis (crystalline silica) Asbestosis (asbestos) Hard metal disease (cobalt, tungsten) Benign pneumoconiosis • Non-fibrotic disease • Changes may be seen on X-Ray, but breathing not usually impaired. • Insoluble deposits including: - Iron oxide - Tin oxide - Barium sulphate Emphysema and bronchitis Emphysema • progressive destruction of the alveoli walls causing merging of alveoli • fewer, larger alveoli, leading to less surface area • breathlessness, cough • chronic condition – can be caused by cadmium oxide, smoking Chronic Bronchitis • excess mucous, chronic infection of the bronchioles • often secondary to other disease Lung cancer • Abnormal growth of cells in the lungs – – – – – Asbestos Rubber fume Chromium (VI) Arsenic Smoking etc • Usually a tumour develops in the bronchi – Symptoms include coughing, pain and breathing obstruction – Cells from the cancer may spread to other parts of the body – Often fatal Respiratory sensitisation • Allergic Rhinitis – Rapid allergic reaction affecting nose, throat and eyes – Nose can become ‘blocked’ or excessively runny – Eyes become swollen, red, itchy and watery – Can be caused by a wide range of substances including pollen, organic dusts and some chemicals Respiratory sensitisation • Occupational asthma – – – – Inflammation and allergic constriction of bronchi Narrowing of airways and increased mucus production Tight chest, breathlessness, wheezing, difficulty breathing out Allergic reaction often occurs after repeated exposure after which the person becomes sensitised to very low exposure levels • Respiratory sensitisers include – – – – – – Isocyanates Solder fumes Some metals (e.g. platinum, cobalt) Organic materials such as latex, animal proteins, vegetable dust Detergents Enzymes Respiratory sensitisation • Extrinsic allergic alveolitis – Inflammation of the terminal bronchioles and alveoli • Acute effects – Delayed flu-like symptoms lasting 48 hours – Fever, headache, muscle pain, cough • Chronic effects – Fibrosis, weight loss, breathlessness on exertion, disabling • Causes – Inhalation of respirable fungal spores, dried animal proteins – There are a number of industry specific terms including ‘Farmers Lung’ (Mouldy grain, hay). Respiratory sensitisation Byssinosis • Caused by exposure to dust produced during machine spinning and weaving of cotton and other vegetable fibres such as flax and hemp. • Symptoms develop after many years of exposure and include tight chest, breathlessness, cough. In chronic cases breathing difficulty due to irreversible airway obstruction which can be disabling. Skin • Structure & function • Skin as a route of entry • Skin as a target organ - dermatitis - other skin conditions Skin Structure Source: Tranter 1999 – Reproduced with permisssion Skin Structure and Function • Epidermis – can be divided into 3 cell layers - cornified - granular - germinative • Dermis - connective and elastic tissue which also contains: -hair follicles -blood vessels -sweat glands -nerve fibres -sebaceous glands • Subcutaneous layer - contains fat cells - insulates, cushions Skin as a route of entry • Properties of toxins - solubility: lipid soluble agents permeate better than water soluble e.g. phenol, solvents, organo-phosphate pesticides • Properties of skin which increase permeation - warm, moist skin: prolonged sweating, skin folds - damaged skin: pre-existing disease, physical damage, defatting • Exposure - chemical trapping: under gloves or clothing Skin as Target Organ Dermatitis = Any inflammatory disease of the skin • Symptoms: reddening of skin (erythema), scaling and cracking – may also become swollen and itchy and sometimes blistered • Dermatitis is very common and difficult to treat successfully • Can be divided into two categories – Irritant contact dermatitis – Allergic contact dermatitis Irritant Contact Dermatitis • About 70% of occupational skin disease • All workers exposed may be affected, provided exposure is repeated and prolonged • Typical skin irritants – – – – – – Detergents Alkalis (lime, cement, caustic) Acids Organic solvents Oxidising and reducing agents Some plants Dermatitis Allergic Contact Dermatitis • About 20% of occupational skin disease – Only sensitised workers affected – once sensitised symptoms occur even on very low exposures • Examples include: – Nickel (‘nickel itch’) – electroplating, jewellery – Epoxy resins (adhesives) – Latex (gloves etc) • Causative agent often confirmed by patch testing Other skin conditions Folliculitis – Pores blocked by oils, greases, waxes – Causes acne like lesions • Chloracne – type of folliculitis caused by chlorinated hydrocarbons. Pigmentation Disturbances • De-pigmentation - some phenols • Hyper-pigmentation - tar and some insecticides - can cause reddening and darkening of skin - silver salts – can cause blue-grey discolouration Ulceration of skin • Ulceration of skin is a well documented effect of exposure to hexavalent acid – Chromic acid in electroplating industry – Also some cements that contain hexavalent chromium – Other examples include: • Antimony • Mercury fulminate Skin Cancer • Malignant tumour – UV exposure • Most common cause – associated with production of melanomas (cancer of melanin producing cells in the skin) – – – – Polycyclic aromatic hydrocarbons (PAH) Coal tar, asphalt Soot Arsenic Nervous System • Structure and function • Nervous system as a target organ – Structural damage to neuron – Functional damage to the nerves Nervous System • Controls the activities and functioning of the body – Also responds to external stimuli in a precise, rapid manner • Anatomical Divisions: – Central Nervous System (CNS) • brain & spinal cord – Peripheral Nervous System (PNS) • all other nerves Nervous system • Nervous system can also be divided into two functional divisions • Motor nerves – control movement (muscles) – somatic control voluntary movement – autonomic control involuntary movement (e.g. heart beat, breathing) • Sensory nerves – involved in the sensation of touch, pain, temperature, vibration, sight, sound, balance Nerve cell (neuron): functional unit (Source: Multiple Sclerosis Trust – reproduced with permission) • Cell Body: makes proteins for all parts of neurone with central nucleus • Axons: long projections along which nerve impulses travel rapidly • Myelin sheath: fatty substance that insulates the axons and speeds up conduction • Post-synaptic membrane: nerve or muscle cell Transmission of nerve impulse (signal) • Nerve impulses transmitted along axon as electrical signals – Signal caused by rapid polarisation and depolarisation of the axon which changes the balance of sodium and potassium ions between the axon and the outside – Signal reaches the end of the axon (the synaptic knob) which is located close to the target cell – Gap between the synaptic knob and the target cell is called the synapse or synaptic gap Normal synaptic transmission • Arrival of nerve impulse triggers release of chemical neurotransmitters (e.g. acetylcholine) into synaptic gap. • Acetylcholine travels across gap to the target cell or neuron. This triggers a response in the target cell • Enzyme (acetylcholinesterase) destroys the acetylcholine to prevent continued stimulation of the target cell Nervous system as a target organ Structural damage to neuron • Lead – damages myelin sheath slowing nerve impulse transmissions • Mild symptoms – tiredness • Severe cases – peripheral neuropathy producing muscle weakness, often showing as ‘wrist drop’ or ‘foot drop’ • n-Hexane – causes swelling of axon and degeneration of axon and myelin sheath • Symptoms include muscular weakness and sensory motor loss particularly to hands and feet Nervous system as a target organ • Structural damage to neuron – Manganese – damages axon • Symptoms resemble Parkinson’s disease with tremor and difficulty in walking and speaking – Mercury – damages the sensory nerves • Symptoms include hearing, speech and vision problems. Also tremors and shaking and psychiatric disturbances – Organo-metallics (e.g. methyl mercury and tetra ethyl lead) – can readily reach the brain • Symptoms include irritability, memory loss, convulsions and psychiatric disturbances Blood Brain barrier • Selective barrier which protects most of brain against water soluble toxins • but permeable to lipid soluble toxins (e.g. organometals, solvents) • Matures 6 months after birth (consequence?) Most tissues Blood brain barrier Nervous system as a target organ • Functional damage to nerve – Organic solvents – act as CNS depressants • High affinity for lipid rich tissues (e.g. myelin sheath) and absorb into it causing swelling and impairing nerve impulse transmission • Acute narcotic and anaesthetic effects: drowsiness, loss of feeling, unconsciousness, death • Chronic effects: possible long-term damage to neurons Nervous system as a target organ • Functional damage to nerve – Organo-chlorine pesticides – polarisation and depolarisation of axon is prolonged • Symptoms include tremors caused by nerves becoming hyper-excitable – Organo-phosphorous pesticides – interfere with chemical transmission across the synapse • Acetylcholine not hydrolysed by target cell enzymes leading to reactivation of target cell • Symptoms include excessive muscle contractions, convulsions and paralysis Circulatory system • Components and function • Blood as a target organ – – – – – Haemolysis Carboxyhaemoglobin formation Methaemoglobin formation Anaemia Leukaemia Circulatory system • Main components of cardiovascular or circulatory system are the heart, the blood and the blood vessels • Blood vessels – Arteries – bring oxygenated blood pumped from the heart to the tissues – Veins – bring de-oxygenated blood back to the heart – Blood passes from arteries to veins through capillaries – the thinnest and most numerous of the blood vessels Blood composition and function Main function is transport O2 from lungs to tissues, CO2 from tissues to lungs Also transports nutrients, heat, waste, toxins. 55% Plasma - fluid component (water, electrolytes, proteins) Thrombocytes (platelets) - blood clotting Leucocytes (white blood cells) - defence (phagocytic cells and cells involved in immunity) 44% Erythrocytes (red blood cells) - transport O2 and CO2 bound to haemoglobin Red blood cell (erythrocytes) • Responsible for transport of oxygen – Main component is haemoglobin (Hb) – large complex molecule composed of protein (globin) and pigment (haem) that contains ferrous iron – Produced from stem cells in blood marrow (together with white blood cells and platelets) – Lifespan 120 days – Normal forms of Hb are • Oxyhaemoglobin (HbO2) • Carbaminohaemoglobin (HbCO2) White blood cell (leucocytes) • Main function is to protect the body against infection from invading organisms • Two main types – Phagocytic cells – scavenger cells – physically engulf and destroy foreign bodies and bacteria – Immunocytic cells – complex mechanism – produce antibodies that directly attack specific organisms such as viruses Blood as a target organ • Haemolysis (breakdown of red blood cells) – Occurs when cell membrane is damaged and cell destroyed – Breakdown products reach the kidney and may damage or overload kidney function – Characterised by appearance of blood breakdown products in urine which turns red – Causes: arsine (arsenic trihydride) and stibine (antimony hydride) Blood as a target organ • Carboxyhaemoglobin formation – Oxygen transported by haemoglobin as oxyhaemoglobin • However, carbon monoxide binds strongly to haemoglobin forming carboxyhaemoglobin which prevents uptake of oxygen • As levels of carboxyhaemoglobin increase, ability of blood to transport oxygen decreases – Symptoms: headache, lethargy, dizziness, unconsciousness, death – Sources: Incomplete combustion, engine and boiler exhausts, metal smelting and processing • Note: exposure to dichloromethane can also lead to elevated carboxyhaemoglobin levels as carbon monoxide is produced as a breakdown product of dichloromethane metabolism Blood as a target organ • Methaemoglobin formation – Methaemoglobin is an oxidation product of haemoglobin that has no oxygen-carrying capacity • Iron in the red blood cells is converted from the ferrous (II) state to the ferric (III) state • Methaemoglobin can be produced after exposure to some aromatic amines such as aniline Blood as a target organ • Anaemia – Condition when amount of haemoglobin in blood is reduced – May be caused by substances that affect normal production of haemoglobin in the bone marrow – Can be caused by inorganic lead and benzene • Leukaemia – Group of blood disorders where abnormal white blood cells are produced in large quantities which replace or crowd out normal white blood cells – Can be caused by benzene Liver – structure and function • One of the largest organs in the body • Main functions – Metabolism of fats, carbohydrates & proteins – Biotransformation of alcohol, hormones and organic chemicals to increase water solubility for excretion by kidneys – Production of bile to aid fat digestion in small intestine – Storage of iron and some vitamins – Production of plasma proteins Position in circulation Position in circulation • Receives high flow of oxygenated blood from hepatic artery and • Partially deoxygenated blood from small intestine via hepatic portal vein • Blood returns to circulation via hepatic vein • Liver is first organ to receive blood from digestive tract and is therefore liable to be exposed to high concentrations of substances absorbed from gastrointestinal tract Liver – structure and function • Liver is main site for biotransformation – Metabolic changes detoxify (or in some cases produce metabolites that are more toxic) – In either case the liver may be at risk • Liver lobules – Groups of cells that lie between the hepatic artery and portal vein and the hepatic vein – Blood that may contain toxins passes over these cells which contain enzymes that are involved in the biotransformation process – Detoxified blood passes into the central vein for return to the circulatory system The liver as target organ • Fat accumulation in liver as product of biotransformation – Causes – exposure to chlorinated hydrocarbons, excessive consumption of alcohol • Cirrhosis – build up of fibrous tissues – Causes – exposure to many organic solvents, excessive consumption of alcohol – May be a pre-cursor of liver cancer • Note: for above effects there may be synergistic effects from alcohol and solvents The liver as target organ • Liver cancers – In addition to cancers linked to fibrous changes (e.g. cirrhosis) of the liver, there are a few specific examples of substances that can cause liver cancer – Arsenic – Vinyl chloride monomer – exposure has been linked to angiosarcoma (a rare liver cancer) Structure and function of the kidneys Range of functions – Excretory functions • Filtration of normal metabolic waste products from the blood • Excretion of water-soluble toxins and metabolites and excess salts from urine – Regulatory functions • Regulation of sodium, potassium and other salt levels • pH (acidity) of blood • Body water and blood fluid levels – Specialised functions • Production of some hormones and vitamin D Nephron function • The kidney plays a crucial role in regulating electrolytes in the human blood (e.g. sodium, potassium, calcium). • pH balance is regulated by the removal of excess hydrogen ions (H+) from blood. • Kidneys remove urea from the body, a nitrogenous waste product from the metabolism of proteins. Kidneys as a target organ • Vulnerability – route of excretion for water soluble toxins & their metabolites – reabsorption of water concentrates toxins in tubules – high blood flow • Kidneys damaged by wide range of substance – those that: – interfere with oxygen supply – damage the glomeruli – block / damage tubules or interfere with tubular reabsorption Kidneys as a target organ • Acute renal failure (renal shutdown) – Urine production decreases allowing urea and other waste products to accumulate in blood – Examples of substances that can cause acute renal failure include: • Arsine and stibine - can cause breakdown of red blood cells which can block the tubules. Appearance of haemoglobin in urine can cause it to turn red. Kidneys as a target organ • Chronic kidney damage or renal failure – Can occur when a significant number of nephrons are damaged or die – Remaining nephrons are overloaded. Proteins and glucose are found in urine – Heavy metals e.g. cadmium, mercury and lead • Characteristic low-molecular weight proteins are found in the urine as result of kidney damage by cadmium – Halogenated hydrocarbons e.g. carbon tetrachloride and chloroform • Biotransformation of these substances in the liver produces a metabolite that damages kidney tissue Reproductive system • Exposure to some substances may affect ability to produce offspring • Males – Reduced sperm count or sperm motility • Causes: some pesticides, oestrogen (pharmaceutical manufacture), some glycol ethers, lead • Females – Menstrual disorders • Causes: carbon disulphide, inorganic mercury – Increased risk of miscarriage • Some glycol ethers, lead, some anaesthetic gases Reproductive system • Exposure to some substances may affect the development of the unborn child – Termed developmental toxicants or teratogens that can affect the embryo or foetus – Often relatively non-toxic to the mother – Organic mercury – can affect development of brain cells leading to CNS defects – Thalidomide – caused upper and lower limb defects – Lead – can cross the placental barrier and can cause severe swelling of the brain and destruction of neurons. It can also cause spontaneous abortion or premature birth