Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Childhood immunizations in the United States wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Inflammation wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Immune system wikipedia , lookup
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
DNA vaccination wikipedia , lookup
Molecular mimicry wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Common cold wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Henipavirus wikipedia , lookup
Innate immune system wikipedia , lookup
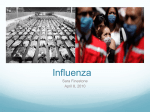
The 3rd International Medical Congress of Prof. Alireza Yalda Foundation in Medical Sciences 17-20th November 2012 Tehran The Role of Cytokine Storm in Influenza Pathogenesis Presented by: Talat Mokhtari-Azad Director of National Influenza Center WHO Collaborating Center School of Public Health, Tehran University of Medical Sciences 1 Some people get horribly sick from the flu, and even die. Others just rest for a few days. What’s behind this fateful variation? How is it that the flu virus can have such a variable impact on people? Nature 2011; 480 (8) S14 Influenza A virus tropism NATURE REVIEWS MICROBIOLOGY 2011; 595 (9) Influenza A virus tropism NATURE REVIEWS MICROBIOLOGY 2011; 595 (9) Influenza A virus tropism NATURE REVIEWS MICROBIOLOGY 2011; 595 (9) Influenza A virus tropism NATURE REVIEWS MICROBIOLOGY 2011; 595 (9) Viral and host factors influencing the pathogenesis of influenza A virus NA promotes efficient release of viral progeny from infected cells Viral factors PB1-F2 induces apoptosis, promotes bacterial growth and acts as interferon antagonist HA determines receptor binding, and antigenicity and tropism depending on the presence or absence of a polybasic clavage site: H5N1: PQRERRRKKR↓G H7N1: PEIPKR-RRR↓G H1N1: PSIQ-------SR↓G H3N3: PEKQ-----TR↓G H2N2: PQIE------ SR↓G The genotype of PB1, PB2, PA and NP determine viral replication competence NS1 is a multifunctional interferon antagonist NATURE REVIEWS MICROBIOLOGY 2011; 595 (9) Viral and host factors influencing the pathogenesis of influenza A virus Host factors Understanding health conditions that increase suseptibility: Elderly (>65 years of age) Children (< 2 years of age) Pregnant women Immunocompromised individuals Understanding health conditions that increase suseptibility: Asthma and COPD Cardiovascular disease Obesity Diabetes Increased and sustained inflammatory • responses contribute to disease severity Host factors influence viral infection by direct or indirect interactions with viral proteins during different stages of replication: Required factors include ATP6V0D1, CAMK2B, CLK1 and p27 restriction or regulatory factors NATURE REVIEWS MICROBIOLOGY 2011; 595 (9) NOVEL CONCEPT ABOUT INFLUENZA PATHOGENESIS -The sequence of HA cleavage site is a major determinant of disease severity ( local versus systemic) - PB1-F2 protein , which leading to apoptosis( e.g.1918/ H1N1 and in various isolates of H5N1), promotes and increases pathogenesis of secondary pneumonia infection - PB1-F2 cooperate with NS1 to inhibit INF response - NS1protein , which is an antagonist of INF-mediated antiviral host response and a modulator of adaptive immune responses , and can inhibit global host gene expression through its interaction with the nuclear cleavage and polyadenylation factors (cpsf4 or CPSF 30) - NS1 contributes to the cytokine dysregulation that is seen in human that succumb to HPAI H5N1 virus infection. 9 TISSUE TROPISM IN THE INFLUENZA PATHOGENESIS - Influenza has different disease phenotypes most commonly URT, conjunctives, pneumonia, and encephalitis - Seasonal flu has strong tropism to URT ( rhinitis, pharynitis, laryngitis), tracheo bronchitis - HPAIV H5N1 weak tropism to URT and strong tropism to LRT which may explain in part its failure to transmit efficiently among human - URT is lined by olfactory mucosa and HPAIV H5N1 replicate in olfactory mucosa of URL and virus spreads directly from OM to the olfactory bulb and rest of the CNS and causing severe meningitis, encephalitis 10 TISSUE TROPISM IN THE INFLUENZA PATHOGENESIS - H7N7 associated predominantly to conjunctivitis. And probably is mediated by a signal transduction pathway in corneal epithelial cells related to NF –kB - HpH5N1 and Hp AIV H7N1 have strong tropism to LRT and attaches abundantly to Clara cells lining bronchioles, type II pneumocyte lining alveoli, and alveolar - Macrophage in alveoli and this tissue tropism fit with the primary diagnosis in the acute stage by alveolar epithelial necrosis, flooding of alveolar lumina by edema fluid mixed with fibrin, erythrocytes, macrophages , and neutrophil and lining alveolar ducts by hyaline membranes -H5N1 induced significantly higher production of the cytokine( TNF (in macrophages and may explain in part the severity of LTR disease and high fatality rate of H5N1 infection infection 11 THE ROLE OF CYTOKINES IN THE IMMUNE SYSTEM • • • • Pro-inflammatory cytokines, such as interleukin (IL)-1, IL-6, tumor necrosis factor (TNF)-α, and interferon (IFN) -γ, serve to recruit cells to the site of infection and mediate direct antiviral effects. The up-regulation of anti inflammatory cytokines, such as IL10 and transforming growth factor (TGF)-β, also occurs during infection with the purpose of regulating the extent of inflammation. This forms of regulation are critical to contain excessive inflammation that can cause more harm than good. However, during some infections and pathological conditions, regulation fails, and an unbalanced cytokine response called a cytokine “storm” can develops, leading to uncontrolled inflammation and increased morbidity and/or mortality for the host. Non-cytopathic virus Neutrophil pDC TH1,TH2 & TH17 cells NK cell CTL DAMPs PAMPs iDC Immunity Non-cytopathic virus Cytopathic virus Tissue cell Type 1 IFNs MQ RNS IL-17 ROS IL-1β IL-6 IL-10 TGF-β IL-1β Treg cell TH1,TH2, TH17 cells IFN-γ TNF-α Perforin Immunopathology Granzymes Infected tissue Mature DC CTL MHC-II TCR IL-6 IL-21 B cell IFN-γ IL-12 TH1 IL-4 IL-5 CD4 T cell TGF-β IL-6 TGF-β TFH TH17 Virus inducers Vasulitis glomerulonephritis Immune complex formation & complement activation Lymph node T cell cytokines Treg cell IFN-γ TNF-α IL-10 Almost all Viruses TH2 Treg IL-17 IL-22 IL-21 TNF-α HSV HCV HIV TGF-β IL-10 IL-35 IL-4 IL-5 IL-13 HSV HCV HIV Friend virus Dengue virus RSV IL-21 ? THE IMMUNE RESPONSE TO INFLUENZA Production of proinflammatory cytokines by epithelial and immune cells increases vascular permeability, allowing the additional cells of the immune system to pass through the endothelial barrier and reach the infected tissue. Continuous viral replication leads to a constant influx of immune cells into the site of infection and increased production of cytokines. Without control mechanisms, this positive feedback loop between cytokines and immune cells results in hypercytokinemia, ultimately causing severe damage to the host. HOST DETERMINANT OF PATHOGENESIS -Highly PI viruses can induce the high plasma level of: INF gama- induced protein(IP10; also known asCXCL10) -Monocyte chemoattractant protein 1( also known CCL2) -Interleukin 8(IL-8), IL-6, IL-10 and other pro-inflammatory cytokines that correlate with an elevated pharyngeal viral load and increased frequency of death caused by viral pneumonia -Increased and prolonged of transcription of type 1 IFN , inflammation and innate immune induction are seen during infection with HPH5N1 virus, resulting apoptosis of DC and severe pathology -TNF and IL-1 increase infiltration level of leukocyte, neutrophil and macrophages -CD8 effector T- cell, by producing IL-10 could control the lung inflammation and injury that is induced during acute influenza infection -NK cell, B cell and antigen presenting cell are susceptible to influenza virus 15 Balance between pro- and anti-inflammatory mechanisms may decide the outcome of viral infection! Pro-inflammatory mechanisms Cytokines and chemokines: IL-2, IFNs, TNF, IL-1β, IL-6, IL-8 IL-12, IL-17, CCL2, CCL3 and CXCL2 Chemical mediators: Prostaglandins, histamines and cyclooxygenases Reactive species: Reactive oxygen species Reactive nitrogen species Proteinases: Matrix metalloproteinases Anti-inflammatory mechanisms Treg cells Cytokines: IL-10, TGF-β and IL-23 Chemical mediators: Resolvins, protectins, galectin 1 and galectin 9 Inhibitory receptors: PD-1, LAG3, TIM3 and CTLA4 Innate immune regulatory proteins: TLR signal inhibitors: A20, SOCS1 and SOCS3 RLR regulators: ubiquitin ligase NLR inhibitors: p202 Pro-inflammatory mechanisms Anti-inflammatory mechanisms Tissue damage Homeostasis Viral persistence Nature Reviews Immunology 2010; 10 THE GOOD, THE BAD AND THE UGLY PATHOGENESIS IN INFLUENZA The good : protection afforded by innate and adaptive immunity - To activate rapid response recognition of RNA by toll like receptors and retinoic inducible gene I(RIG-1) is key -These receptor leads to the production of proinfammatory cytokines and type I IFN-α and β - These cytokines exert antiviral activity by inhibiting viral replication and jump stars the adaptive immune response (virus specific B and T responses) and result in clearance of the infection) 17 THE GOOD -Individual that have experienced an influenza infection in the past are more resistant to subsequent infection with influenza viruses of the same type (p2009 H1N1) -Infection with influenza viruses also induce protective immunity to influenza A viruses of other subtypes ( heterotypic Immunity) -Immune response to conserved proteins (NP, M) are at the basis of heterotypic immunity specially cross reactive T-cell response are involved. 18 THE BAD Increased virulence is often correlated with: Increased virus replication Tropism Regulation of immune response The best known determinants of virulence are the multibasic cleavage site of HA, receptor binding preference of HA, NA activity, PB2, PB1, NP, NS1 NS1 through it antagonise the innate response specially INF. 19 THE UGLY The excessive or dysbalanced immune response, especially in the LTR, may be determined - Overproduction of cytokines such as TNF-α, IL-6, IL-8, IFN type I or II as well as chemokines can result in severe inflammation, including excessive recruitment of neutrophils and mononuclear cells at the site of infection. This may damage lung tissue , reduce respiratory capacity and cause severe disease and mortality (e.g. H5N1, 1918 H1N1) 20 UGLY -In sufficient expression anti-inflammatory molecule such as HLA-G, interleukin 10, transforming growth factor-beta could influence extent of inflammation and pathogenesis of infection. -Importantly , alveolar macrophages expressing high level of CD200R are critical immune-suppressive cells that upon activation prevent elevated cytokine environment. -In contrast to monocyte-derived macrophages that infiltrate the lung after infection starts, resident alveolar macrophages may be important in suppressing inflammation of the lung. -Recently it was shown that activation of endothelial cells plays a central role in the initiation of excessive cytokine production and inflammatory cell recruitment. 21 POSSIBLE THERAPEUTIC AVENUES Antiviral therapies that directly target the virus (including NA inhibitors: oseltamivir and zanamivir, and M2 inhibitors: amantadine and rimantadine) are currently the main form of influenza treatment. Viral resistance to M2 inhibitors is widespread among seasonal and pandemic influenza strains, while oseltamivir resistance is mainly observed in seasonal influenza and is not very common in pandemic influenza strains. The success of oseltamivir and zanamivir lies in the fact that most influenza viruses have difficulty altering the NA site that they target, making viral escape difficult. However, a low number of oseltamivir-resistant pandemic (H1N1) 2009 as well as H5N1 viruses have been reported in several countries. POSSIBLE THERAPEUTIC AVENUES high rates of viral resistance to currently available drugs and points to the need for strengthening available treatment options, including therapy that targets the host immune response. Anti-inflammatory agents that dampen the cytokine responses during influenza infection have been shown to decrease morbidity and mortality . There are a number of anti-inflammatory treatments used to treat autoimmunity, including TNF blockers, which may be of use in a cytokine storm situation during acute influenza infection. Clearly, more research is required before many of these immunomodulatory concepts can move into the clinic. CONCLUSION • • • • Despite an increase in influenza literature over the last two years, it is still unclear what causes the severe morbidity and mortality associated with pandemic influenza strains. One potential mechanism is the induction of a cytokine storm and an imbalance of protective versus pathogenic immune responses. Since cytokine storms are likely to arise through various mechanisms, treatment options should focus on the overall cytokine imbalance and associated immunopathology rather than targeting specific components of the storm. It is clear that more work is needed to fully understand the pathogenicity of pandemic influenza viruses and correlations of cytokine storms to disease severity, ongoing efforts in this area could lead to better therapeutic approaches to combat the next influenza pandemic.