Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Adaptive immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Human leukocyte antigen wikipedia , lookup
Molecular mimicry wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
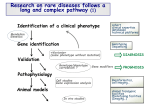
Severe Combined Immunodeficiency Syndrome • A heterogeneous group of congenital disorders which results in the absence of antigen-specific T and B cell responses 1/50-100, 000 live births Newborn screening estimate now 1/30-40,000 live birth Athabascan-speaking Native Americans, an incidence of 52/100,000 live births • Early classification based on presence or absence of adenosine deaminase and the % and absolute numbers of T, B, and NK cells Genetic mutations associated with SCID Gene Function Phenotype Chromosomal location Year Published ADA Purine salvage enzyme Recycles adenosine and deoxyadenosine after DNA breakdown T, B-, NK+ 20q12-13 1972 TCR abn Signaling through TCR Tlo, B+,NK+ 11q23 g chain Common g chain (IL-2,4,6,15,21) T-,B+, NK- Xq13 1987 1993 ZAP 70 Tyrosine Kinase CD8 def 2q12 1994 Janus kinase- 3 Tyrosine kinase Signaling through gC T-, B+, NK- 19p13 1995 RAG1, RAG-2 •Omenn's syndrome Recombinase activating genes initiation of VDJ recombination T-B-NK+ 11p13 1996 T+, B-,NK+ IL7-Ra Cytokine Receptor T-, B+, NK+ 5p13 Artemis DNA repair enzyme T-B-NK+ 10p 1998 1998 Mutations associated with SCID Gene GENE FUNCTION Common Phenotype Chromosoma l location Year published CD45 TYROSINE KINASE T-,B+,NK low Chr 1 2000 DNA ligase IV DNA REPAIR ENZYME T(low),B+, NK+ 11q23 2001 IL-2R/IL-15b subunit Cytokine receptor subunit T (low) B+ NK- Unk 2001 FOXP3 Mutations IPEX T reg deficiency Immune dysfunction polyendocrinopathy Enteropathy X linked Auto variants 2001 Adenylate kinase 2 AK2 Reticular dysgenesis mitochondrial intermembrane space, stria vascularis region of the inner ear T-B-NK+/Absent neutrophils Deafness 1p31–p34 2009 Diagnosis and Outcome of infants identified by newborn Screening Diagnosis Evaluation Treatment Outcome Outcome #1 ADA deficiency now 17 months old 34 lymphs/ul PEG ADA Normal T cell function Vaccinated Successfully #2 X linked + FH Now 16 months B+, NK+, T- TCD HLA-MM Related BMT Normal T cell function #3 ADA deficiency Now 16 months old 117 lymphs/ul 85% NK, 15% B PEG ADA Normal T cell function #4 Normal NL phenotype NL T cell func NL B cell function #5 Transient T lymphopenia Now 9.5 months old CD3-233/ul T cell numbers Normalized NL T cell function Vaccinated Successfully IgG3 deficient #6 T lymphopenia NL ADA, IL-7R, nl NL CD3 d, e Now almost 9m CD3:741/ul, inc B CD4:613/ul CD8:117/ul T cell numbers Increasing but not normal NL T cell function Vaccinated Successfully #7 X linked Now 4 months old B+, NK+, T- TCD HLA –MM RelBMT 3+ m, well No GVHD T cells coming in #8 Likely X-linked NL ADA, PNP ALC 1450, B 1450/ul No T, NK 29/ul Being HLA typed 3 weeks old Vaccinated Successfully Pre HCT Laboratory Evaluation Lymphoid phenotype PHA, MLC, NK function ADA and PNP levels Immunoglobulin levels HIV Ab parents, HIV PCR child HLA Class I and Class II expression +/- phenotyping for CD127 (IL-7R)or CD132 (IL-2g chain) if consistent phenotype Response to PEG-ADA • 20% show no response • Majority see T cell immune response in the short term but it wanes with time • B cell immunity, 50% will need continued IVIG – B cell numbers increase within a few weeks of therapy – T cell numbers may require several months to increase RESPONSE TO PEG-ADA in two infants identified by NBS #CD56 #CD3 #CD4 #CD56 #CD8 #CD3 500 600 400 500 300 400 Cells/ul Cells/ul 600 200 #CD4 #CD8 300 200 100 100 0 0 5 10 0 15 0 Age (months) 5 10 15 Age (months) #CD19 B cells #C19 B cells/ul 2500 600 1500 Cells/ul Cells/ul 2000 1000 400 200 500 0 0 5 10 Age (months) 15 0 0 5 10 Age (months) 15 Response to PEG-ADA 200000 200000 CPM 150000 CPM 250000 PHA Response Patient #1 LLN:>109,000 100000 50000 150000 PHA response Patient #2 LLN: >109,000 100000 50000 0 0 0 5 10 15 0 5 Diph Pert Pre 0.81 1.01 6 Post 3.43 1.39 403 15 Age (months) Age (months) Tet 10 HIB PRE 1(0.6)3(1.40)4(0.0)14(3.4)19(2.0)23(0.9)6B(1.20) 7F(1.3)18c(0.90) POST PCV13x3 1(8.1)3(>37.6)4(6.5)14(2.1)19(7.4)23(3.3)6B(11.8)7F(33.9)18C(12.3 ) Tet Diph Pert HIB Pre 1.21 0.6 5 1.61 Post 6.79 >2.5 37 >9 PRE 1(0.8)3(>37.5)4(0.5)14(2.1)19(1.2)23(0.6)6B(0.7)7F(4.4)18c(0.6) POST PCV13x3 1(9.3)3(34.4)4(4)14(1.6)19(6.4)23(1.3)6B(3.9)7F(18.1)18c(6.6) Results of HCT for ADA deficiency Publication Eur Experience* MSKCC Ulm, Munich HLA MSIB 81%, n=19 none 100%, n=7 81-100% *50% survivors had neurologic deficits Alternative donor 29%, n=26 50%, n=8 63%, n=8 29%-63% Newborn Screening Allows early identification and treatment of affected infants EFS if HCT <2 months of age: 90-100% Currently how well young infants tolerate cytoreduction is unknown How much cytoreduction to ensure B cell engraftment unknown NBS also uncovers infants who may have transient lymphopenia or immune defects that previously were unrecognized and may or may be associated with an increased risk of infection. Need to determine best way to inform parents Current literature needs to be translated into multiple languages Available literature for parents is either too simplistic or too complicated Longitudinal lymphoid phenotype of female child with low-absent TRECS on newborn screen Patient # 1 Serum Ig levels Total lymphs #CD3 #CD4 #CD8 #CD19 #CD56 4000 3000 2000 600 IgG IgA IgM 400 mg/dl Absolute number/ul 5000 200 1000 0 0 0 2 4 6 8 10 0 Months of age 2 4 6 8 10 Months of age Percentage CD4+CD45RA+ cells Absolute numbers of CD4+ CD45RA+ cells 1.0 1500 Normal TRECS cells/ul Percentage 0.8 0.6 0.4 1000 No TRECS 500 0.2 0.0 0 0 2 4 Age (months) 6 0 2 4 Age (months) 6 Lymphoid phenotype and function %CD4/ CD45RA Age ALC CD3 CD4 CD8 CD19 CD56 2 months 1750 228 140 53 735 770 2.5 months 1966 550 354 177 1219 216 0.33 3 months 2674 856 508 321 1444 508 0.47 3.9 months 2700 1161 675 459 1269 351 0.72 5. 1 months 4090 2536 1594 900 1268 286 0.79 PHA OKT3 160,143 13, 478 189, 056 Longitudinal immune phenotype and function of female infant with low but detectable TRECs on newborn screen 1000 900 800 700 600 500 400 300 200 100 0 CD19 Bcells #CD3 #CD4 #CD8 #CD56 1500 1250 Cells/ul Cells/ul T Lymphopenia, normal function NL antibody response 1000 750 500 250 0 0 1 2 3 4 0 5 1 Age at test PHA LLN 109, 576 OKT3 LLN 3, 715 Candida LLN: 6624 1.9 m 262881 101032 3283 2.6m 144050 77453 4.2m 100222 5.7m 185539 2 3 4 5 Age (months) Age (months) Tetanus Toxoid LLN:2417 Vaccine Responses 1050 31749 4673 6614 + Response to Tetanus, Pertussis, Diphtheria PCV13, HIB Why do children with SCID ever need cytoreduction To ensure donor B cell engraftment To prevent graft rejection in patients with NK activity via KIR pathways In pts with ADA deficiency-to ensure 100% donor chimerism including red cell lineage To prevent T cell mediated graft rejection in those with PHA >5% LLN Effect of pre-HCT NK function on engraftment following TCD MMrelated SBA- E- BMT in the absence of cytoreduction PRE HCT Engrafted NK function Failed to engraft Absent 14/14 0/14 Present 1/8 7/8 CHI-SQUARE=17.9, p <.001 Results of unmodified HLA-matched related BMT • Matched sibling transplant remains the treatment of choice • Cytoreduction or GVHD prophylaxis generally unnecessary • European Experience 1968-1999: 81%, n=104, – ADA def: 81%, Reticular Dysgenesis: 75%-HLA matched BMT • Single Center – MSKCC: 1971-2011, 87.5% survival, n=16 – Hopital Necker-Enfants Malades 1971-92, 80% survival, n=30 – Univ of Ulm: 81% survival, n=21 – DUMC: 1982-98, 100% survival, n=12 – Univ of Brescia: >80%, n=35 T and B cell function following unmodified HLAmatched BMT for SCID Normal T cell numbers rapidly restored 2-4 weeks 2000 Pt #1 Pt #2 Pt #3 1500 Normal T cell mitogen and specific antigen responses restored Pt #4 1000 500 B cell function returns by one year post transplant 0 pre HCT 1-29d 30-59d 60-89d What about patients who lack HLA matched sibling donor TCD HLA Mismatched BMT Depending on efficiency of T cell depletion Current outcomes: 70-80%, and if HCT <2 months: 90-100% Low incidence of GVHD Parent readily available Probability of Overall Survival after Unrelated Donor Transplants for SCID, 1990-2004, n=200 Probability 1.0 Overall survival, 60% (95% CI 52-67) @ 5 years 0.8 0.6 0.4 No significant advantage over parental T cell depleted HLA non-identical marrow grafts when comparable preparative regimens are used 0.2 Potential risk of infectious complications due to time needed to procure a donor Increased Risk of GVHD 0.0 0 1 2 3 Years 4 5 Probability of Overall Survival after Unrelated Donor Transplants for SCID, 1990-2004, n=200 Probability 1.0 Overall survival, 60% (95% CI 52-67) @ 5 years 0.8 0.6 0.4 No significant advantage over parental T cell depleted HLA non-identical marrow grafts when comparable preparative regimens are used 0.2 Potential risk of infectious complications due to time needed to procure a donor Increased Risk of GVHD 0.0 0 1 2 3 Years 4 5 Probability of Overall Survival after Unrelated Donor Cord Blood Transplants for SCID, 19902005, n=76, CIBMTR Probability of survival 1.0 0.8 Overall survival, 57% (95% CI 44-69) @ 5 years 0.6 Immediately available unlike MUD HCT Viral naïve, CMV seronegative Less acute and chronic GVHD despite 1-2 Ag MM No clear advantage over HLA MM-Rel HCT Higher risk of GHVD, appox 25% aGVHD, 13% chronic 0.4 0.2 0.0 0 1 2 3 Years Post HCT CIBMTR data, 2007 4 5 Immune Function • 50% of children have normal T cell function in the first 6 months post BMT • 80% have normal T cell function by 6 to 12 months post BMT • However, without cytoreduction, lack of donor B cell engraftment, IVIG dependent Recovery of T cells post SBA- E- parental BMT for SCID 10000 1000 100 SCID, with cytoreduction 10 SCID, without cytoreduction 1 Months post Mis-related parental TCD BMT for SCID Recovery of CD4+ T cells post SBA- E- parental BMT for SCID 2000 SCID, with cytoreduction 1600 SCID, without cytoreduction 1200 800 400 0 Months post Mis-related parental TCD BMT for SCID Numbers of circulating naive CD4+ T cells post HCT For SCID CD4+ RA+ T cells per µl 800 700 600 500 400 300 200 100 0 HLA MATCHED SIBLING HLA MM RELATED No cytoreduction HLA MM RELATED With cytoreduction Comparison of the percentage of children with normal PHA post SBA- E- BMT for SCID: With and Without pretransplant cytoreduction 100 80 60 40 20 0 Median serum IgG Levels post Mis-matched TCD BMT for SCID 1200 1000 CYTO NON-CYTO 800 600 400 200 0 0-6M 6-12M 12-18M 18-24M 24-36M 36-48M Median serum IgA Levels post Mis-matched TCD BMT for SCID 100 CYTO NON-CYTO 50 0 0-6m 6-12m 12-18m 18-24m 24-36m 36-48m Conclusions and Future directions The majority of children with SCID can be cured by a HCT providing it is performed early Primary immunodeficiency Treatment Consortium (PIDTC) Retrospective study to determine variables associated with outcome Prospective study to determine outcome of patients identified through newborn screening HCT Gene therapy PEG-ADA Trial under development to determine lowest amt of cytoreduction to ensure T and B cell engraftment Need to determine the best way to inform parents of NBS which require further evaluation Need to develop ways to promptly direct parents to centers which can quickly evaluate and treat children with PID