Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Common cold wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Adaptive immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
West Nile fever wikipedia , lookup
DNA vaccination wikipedia , lookup
Marburg virus disease wikipedia , lookup
Molecular mimicry wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Neonatal infection wikipedia , lookup
Innate immune system wikipedia , lookup
Henipavirus wikipedia , lookup
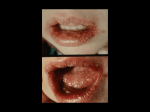
Herpes Simplex Virus Case Study # 12 Maryna Glavatska Michelle Chua Background • • • • • • There are 2 types of HSV: HSV-1 and HSV-2. Family Herpesviridae, subfamily Alphaherpesvirinae. Baltimore classification- group I. Large ds, linear DNA genome. Enveloped viruses. HSV has icosahedral nucleocapsid that contains 162 capsomeres. • The HSV genome encodes approximately 80 proteins and at least 10 glycoproteins. • HSV-1 and HSV-2 establish lifelong infections, they persist in the body by becoming latent and hiding from the immune system in the cell bodies of neurons. Similarities of HSV-1 and HSV-2 Similarities: Under the electronic microscope HSV-1 and HSV-2 look identical; Share more than 50% of their DNA; Both infect body mucosal surfaces (usually the mouth or genitals); Both establish latency in the nervous system; Both types can recur A 2-year-old child with fever for 2 days has not been eating and has been crying often. On examination, the physician notes that the mucous membranes of the mouth are covered with numerous shallow, pale ulcerations. A few red papules and blisters are also observed around the border of the lips. The symptoms worsen over the next 5 days and then slowly resolve, with complete healing after 2 weeks. 1. HSV infection was suspected. How would the diagnosis be confirmed? • Visual examination: multiple vesicular lesions on an erythematous base on mucocutaneous sites that later progress to pustular lesions, ulcers, and crusted lesions; • Location of lesions (anatomic site ); • Age; • Clinical symptoms: - Fever - Malaise - Inability to eat - Irritability; • Duration of symptoms (3-14 days). Laboratory confirmation: Tzanck smear- staining of scrapings from the base of the lesions, which demonstrates giant cells or intranuclear inclusions. Limitation- does not differentiate between HSV and varicella –zoster virus infections. Viral isolation -from vesicular fluid and inoculation in cell culture. Cytopathogenic effects apparent by 24 hours and include the formation of large, round, “balloon” cells and, less commonly, multinucleated syncytial giant cells. Limitation-confirms Herpesviridae family. Laboratory confirmation (cont…) PCR- can make many copies of the virus’ DNA so that even small amounts of DNA in the sample can be detected. Limitation- very expensive. ELISA – serologic test that can identify antibodies that are specific to the virus and its type, HSV-1 or HSV-2. Limitation- useful only for diagnosing a primary HSV infection, because there is no significant rise in antibody titers in recurrent disease Laboratory confirmation (cont…) Direct fluorescent antibody stain for HSV- The fluid from blisters is processed and stained with specific fluorescently-labeled antibodies. Limitations-Proper specimen collection and transport are critical in the detection of etiological agents. A negative result does not rule out a viral infection and has to be supported by PCR. Western Blot blood test - can distinguish between type 1 and type 2 herpes simplex antibody with extremely high accuracy approaching 99% 2. How could you determine whether this infection was caused by HSV-1 or HSV-2? • Oral herpes in children commonly caused by HSV-1. • Genital herpes can be caused by either the HSV-1 or HSV-2 and commonly found in adolescents and adults. • Congenital herpes simplex can be found in newborns and is transmitted from mother to baby in utero or during vaginal delivery. Most often caused by HSV-2. 2. How could you determine whether this infection was caused by HSV-1 or HSV-2? (cont…) • There is some difference between the cytopathic effect caused by HSV-1 and HSV-2 in the cell culture. HSV-1 produces CPE throughout the cells’ monolayer, whereas HSV-2 CPE tend to be focal. • Although HSV-1 and HSV-2 have many antigens in common, the glycoprotein G (gG) antigen is unique to each type; thus, gG1 is found only on HSV-1, and gG2 is found only on HSV-2. • ELISA based test can be used to detect type-specific IgG antibodies (sensitivity around 90%). • Western Blot • PCR 3. What immune responses were most helpful in resolving this infection, and when were they activated? INNATE Immediate ADAPTIVE Late , after 96 h IFN α, IFNβ NK cells- kill virally infected cells Dendritic cells - produce IFN I type Complement system CD8+ T cells -recognize viral peptides by MHC class I molecules on the infected cell surface and kill the cell + produce IFN γ How HSV escapes complete immune resolution? • HSV-1 expresses an immediate-early protein, ICP 47, that effectively blocks the MHC class I antigen presentation pathway. ICP 47 binds with high affinity to the human transporter associated with antigen presentation (TAP) and blocks the binding of antigenic peptides. • Some HSV surface glycoproteins (gC, gE and gI) also help the virus to escape from the immune response. • gC binds complement C3 protein and thus depletes it from the host's serum and inhibits complementmediated reactions. • The virus gE and gI proteins can also bind IgG via the Fc portion of the immunoglobulin. This coats the virus with immunoglobulin and hides it from the immune system. How HSV escapes complete immune resolution? Why sensory neuron remains infected? The virus is quiescent and generates few virus derived peptides to present on MHC class I molecules Neurons carry very low levels of MHC class I molecules, which makes it harder for CD8 cytotoxic T cells to recognize infected neurons and attack them. 4. Sites of latency HSV-1 - usually establishes latency in the trigeminal ganglion, a collection of nerve cells near the ear. From there, it tends to recur on the lower lip or face. So, the site of latency in our patient was trigeminal ganglion. 4. Sites of latency (cont…) HSV-2 - usually sets up residence in the sacral ganglion at the base of the spine. From there, it recurs in the genital area. 4. What might promote future recurrences? • • • • • • • • • sunlight wind fever physical injury surgery menstruation suppression of the immune system emotional stress Oral herpes can be provoked within about 3 days of intense dental work, particularly root canal or tooth extraction. 5. What were the most probable means by which the child was infected with HSV? Oral HSV-1, is typically spread simply by the kind of social kiss that a relative gives a child or sharing utensils. Because children have no prior infection with any HSV type, they have no immune defense against the virus. 6. Which antiviral drugs are available for the treatment of HSV infection? What are the targets? • Acyclovir - This is the drug of choice. Acyclovir require the presence of a HSV-encoded thymidine kinase in order to be converted into its active acyclovir triphosphate form. Acyclovir triphosphate is a potent selective inhibitor of HSV DNA polymerase and causes premature chain termination when it competes with guanine triphosphate for incorporation into newly synthesized viral DNA. Very safe to use. 6. Which antiviral drugs are available for the treatment of HSV infection? What are the targets? (cont…) • Ganciclovir, famciclovir, valacyclovir- have similar mechanism of action; however, ganciclovir is more toxic. • Topical treatment- penciclovir cream or acyclovir cream are generally not highly effective. • These drugs act against the replicating virus and therefore they are ineffective against latent virus. Bibliography • • • • • • • • • Murray, P., Rosental, K., Pfaller, M. Medical microbiology. Fifth edition. 2005. Braunwald, F., Wilson, I., Kasper, M., Longo, H. Harrison’s principles of internal medicine. Fourteenth edition. Volume 1. 1998. Murphy, K. Janeway’s immunobiology. Eight edition. 2012. Slonczewski, J., Foster, J. Microbiology an evolving science. Second edition. 2009. Wagner, E., Hewlett, M., Bloom, D., Camerini, D. Basic virology. Third edition. 2008. http://pathmicro.med.sc.edu/virol/herpes.htm http://www.herpes.com/hsv1-2.html http://health.nytimes.com/health/guides/disease/herpessimplex/diagnosis.html http://www.zeusscientific.com/fileadmin/media/pdfs/inserts/elisa/ infectious/R2206E.PDF