Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Mental status examination wikipedia , lookup
Panic disorder wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
History of mental disorders wikipedia , lookup
Asperger syndrome wikipedia , lookup
Depersonalization disorder wikipedia , lookup
History of psychiatry wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Child psychopathology wikipedia , lookup
Conduct disorder wikipedia , lookup
Schizoaffective disorder wikipedia , lookup
Major depressive disorder wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Spectrum disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Bipolar disorder wikipedia , lookup
Depression in childhood and adolescence wikipedia , lookup
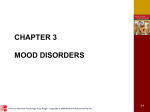
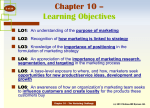
Abnormal Psychology Leading Researcher Perspectives Edited by Elizabeth Rieger Images, Figures and Tables Chapter 3 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-1 2008 Getty Images Andrew Johns, previously a professional rugby league player, has spoken publicly about his bipolar disorder to raise awareness of mood disorders. This will contribute to the destigmatisation and acceptance of these conditions in the community. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-2 Figure 1 The percentage of males and females from the ages of 11–21 years who were diagnosed with major depressive disorder or dysthymia during a one-year period Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-3 Figure 2 Beck’s (1976) cognitive model regarding the development of depressive episodes Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-4 Figure 3 In both forms of cognitive behaviour therapy (CBT1 and CBT2), there was a significantly greater amount of improvement in negative thinking in the session (the ‘pre-gain session’) before a large improvement in depressive symptoms compared with the control session (the session just before the pre-gain session) Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-5 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. Courtesy Michelle Wilson, Macquarie University Transcranial magnetic stimulation (TMS) is a brain stimulation technique that uses magnetic fields to stimulate focal brain areas. The magnetic field is produced by a coil in either a figure 8/butterfly or a circular shape depending on the type of stimulation required. The coil is held against the scalp at the identified site. The stimulation is non-invasive and is given while the person is fully awake and alert. 3-6 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-7 John Cade, the Australian psychiatrist who discovered the beneficial effects of lithium, which was to transform the treatment of individuals with bipolar disorder. Courtesy the family of Professor John Cade Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-8 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-9 Figure 4 The percentage of patients who developed panic disorder, obsessive-compulsive disorder (OCD) or social phobia before, during or after their first manic or hypomanic episode Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-10 Figure 5 The Diathesis-Stress Model of bipolar disorder Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-11 Figure 6 The percentage of bipolar disorder patients in the CBT and control groups who experienced a manic/hypomanic episode or a depressive episode over a two and a half year period Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-12 Figure 7 The Instability Model of relapse in bipolar disorder Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-13 Proposed changes for mood disorders in DSM-V • A new mood disorder is to be added—mixed anxiety depressive disorder— characterised by the presence of a partial major depressive episode (three or four symptoms including mood disturbance and/or anhedonia) accompanied by significant anxiety such as irrational worry, inability to relax or a sense of impending threat. • Dysthymic disorder is to be renamed as chronic depressive disorder. • A diagnosis of major depressive episode will no longer be excluded when the symptoms occur in the context of a bereavement. • A specifier for major depressive disorder called ‘mixed features’ will be included for when some symptoms of elevated mood are present alongside depression. • ‘Mixed episodes’ will be removed as a distinct episode type within bipolar disorder. In the proposed DSM-V; ‘mixed features’ will become a specifier rather than a distinct type of episode. • ‘Temper dysregulation disorder with dysphoria’ will be introduced. This new diagnostic entity has arisen out of the controversy over the high rate of ‘paediatric’ (or ‘juvenile’) bipolar disorder. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-14 Chapter 3 Summary • • • • • Unipolar depression is characterised by periods of depressed mood and/or a loss of interest in activities, together with a range of other symptoms. The main depressive disorders in the DSM-IV-TR are major depressive disorder and dysthymia. Depressive disorders are among the most prevalent psychological problems in Australia. Women are twice as likely to experience depressive episodes compared to men. The aetiology of depressive disorders is thought to be related to biological, environmental and psychological factors, and this multiplicity of factors is reflected in the diverse treatments for depression, which include a range of both medical and psychological approaches. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-15 Chapter 3 Summary (continued) • • The bipolar disorders are defined by the occurrence of manic or hypomanic episodes, characterised by abnormally elevated or irritable mood with a range of accompanying symptoms such as inflated self-esteem, a decreased need for sleep, and increased talkativeness, goal-pursuit and risktaking behaviours. The efficacy of psychological treatments in conjunction with pharmacotherapy has now been established in the treatment of bipolar disorder. Further psychological research is needed to develop interventions that will result in greater long-term maintenance of the benefits from these psychosocial treatments. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 3-16