Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
History of psychiatry wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Conduct disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Autism spectrum wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Spectrum disorder wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Classification of mental disorders wikipedia , lookup
History of mental disorders wikipedia , lookup
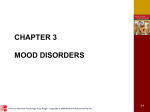
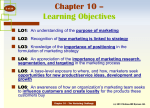
Abnormal Psychology Leading Researcher Perspectives Edited by Elizabeth Rieger Images, Figures and Tables Chapter 10 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-1 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-2 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-3 iStock Oppositional defiant disorder is characterised by a persistent pattern of negativistic, spiteful, irritable and non-compliant behaviour. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-4 Figure 1 Differences in the proportion of problems between the persistent and low/non-antisocial groups and between the experimental and low/nonantisocial groups throughout childhood and adolescence Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-5 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-6 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-7 Continued on next slide Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al 10-8 continued Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-9 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-10 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-11 Disorders of childhood are common, although they are often unrecognised and untreated. Many adult disorders can be traced back to childhood symptoms, highlighting the importance of prevention and early intervention. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-12 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-13 Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-14 SPL/Photolibrary Down Syndrome is a common cause of intellectual impairment, which occurs when a third copy of chromosome 21 is present in the genome. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-15 Proposed changes for childhood disorders in DSM-V Externalising disorders: • In terms of oppositional defiant disorder, the current recommendations for the DSM-V are to maintain the symptom structure, but to distinguish between emotional symptoms (i.e., indications of an angry/irritable mood such as the child losing his/her temper) and behavioural symptoms (e.g., indications of defiant/headstrong behaviour such as the child arguing with or defying adults). In addition, it is proposed that the exclusionary criteria for conduct disorder be removed (so that a child will now be able to be diagnosed with both oppositional defiant disorder and conduct disorder) and that the symptoms occur at different frequencies and intensities for children at different ages in order to more clearly demarcate behaviour that is developmentally normal at a certain age from that which is not. • For conduct disorder there are no proposed changes to the criteria, except for a proposal to add callous, unemotional traits. • For ADHD, adding more symptoms for diagnosing impulsivity (e.g., being uncomfortable doing things slowly and finding it difficult to resist temptations) and requiring fewer symptoms to meet the diagnosis in older individuals. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-16 Proposed changes for childhood disorders in DSM-V (continued) Internalising disorders: • For separation anxiety disorder, it has been proposed that this be re-classified from the category of ‘Disorders Usually First Diagnosed in Infancy, Childhood or Adolescence’ to ‘Anxiety Disorders’, with some minor revisions to the criteria to allow for its diagnosis in adults (e.g., impairment in the work context). • Several new disorders have also been proposed, such as the addition of posttraumatic stress disorder in preschool children to account for developmental differences in the way in which trauma symptoms are experienced. Elimination disorders: • For enuresis, minor changes include the removal of the need for the child to be distressed regarding the behaviour. Learning disorders: • Change to the name of reading disorder to ‘dyslexia’. Similarly, the name for the mathematics disorder will be changed to ‘dyscalculia’. • Because there is little evidence to support the DSM-IV-TR criterion of a substantial discrepancy between the individual’s level of achievement in reading and his/her intellectual ability, the primary criterion will be re-worded to ‘difficulties in accuracy or fluency of reading that are not consistent with the person’s chronological age, educational opportunities or intellectual abilities’. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-17 Proposed changes for childhood disorders in DSM-V (continued) Pervasive developmental disorders: • A range of pervasive developmental disorders (e.g., Asperger’s syndrome) will be subsumed under the autistic disorder category. Autism will be represented as a single diagnostic category that is adapted to the individual’s clinical presentation by specifying the individual’s clinical characteristics (e.g., severity of symptoms and verbal abilities) and associated features (e.g., known genetic disorders, epilepsy, and intellectual disability). • There will be two (rather than three) main domains of criteria: social/communication deficits, and fixated interests and repetitive behaviours. Intellectual impairment: • Changes mainly reflect more rigour in the definitions (e.g., the requirement that psychometrically-sound and culturally-appropriate assessment tools be used to determine the individual’s intellectual ability), and less reliance on IQ testing. For example, severity levels will no longer be based on specific IQ cut-offs as this practice failed to consider the individual’s level of functional skills. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-18 Chapter 10 Summary • Disorders of childhood are common, although they are often unrecognised and untreated. Many adult disorders can be traced back to childhood symptoms, highlighting the importance of prevention and early intervention. • An important message of this chapter is the extent to which the family environment can play a role in the development and maintenance of psychological and behavioural problems in children. Fortunately, effective evidence-based parenting interventions are available to assist parents in changing their child’s behaviour and improving coping skills. • The primary challenge now is to ensure that such interventions are widely available and easily accessible to parents. Psychologists have been at the forefront of tackling this issue by designing more flexible interventions that reach more parents. • In reaching broad sections of the community, such innovative approaches have the potential to undermine pervasive myths that downplay the severity of psychological problems in childhood and prevent children gaining the help they need. Copyright © 2011 McGraw-Hill Australia Pty Ltd PPTs t/a Abnormal Psychology: Leading Researcher Perspectives 2e by Rieger et al. 10-19