Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Schizoaffective disorder wikipedia , lookup
Autism spectrum wikipedia , lookup
Excoriation disorder wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Mental status examination wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Mental disorder wikipedia , lookup
History of psychiatry wikipedia , lookup
Obsessive–compulsive personality disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Conduct disorder wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Spectrum disorder wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Selective mutism wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
History of mental disorders wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Child psychopathology wikipedia , lookup
Obsessive–compulsive disorder wikipedia , lookup
Abnormal psychology wikipedia , lookup
Panic disorder wikipedia , lookup
Claustrophobia wikipedia , lookup
Anxiety disorder wikipedia , lookup
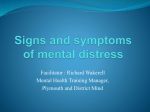
Anxiety Disorders Anxiety: negative mood state characterized by bodily symptoms of tension and apprehension about the future What does anxiety feel like? Heart racing/pounding Sweating Being out of breath Shaking Upset stomach Being “frozen” When is Anxiety Normal/Abnormal? Normal: Motivation Avoiding danger Preparation for uncertainty Abnormal: When it interferes with performance E.g. exams E.g. socially When is Anxiety Helpful/Not Helpful? As arousal increases performance increases, to a point After the optimal point of arousal performance deteriorates as anxiety continues to increase This is called: Yerkes-Dodson Law Yerkes-Dodson Law The optimal point of arousal varies by task For easy tasks: we can tolerate a lot of anxiety and still do well For hard tasks: we can’t tolerate much anxiety When is anxiety an Anxiety Disorder? 1. 2. 3. 4. 5. 6. When the feelings of anxiety constantly interfere with functioning Generalized Anxiety Disorder Panic Disorder & Agoraphobia Specific Phobias Social Phobia Post-traumatic Stress Disorder Obsessive-Compulsive Disorder Causes of Anxiety Disorders Biological Psychological Social Biological Causes of Anxiety Disorders Genetic influences Diathesis X Stress models appy Changes in neurotransmitters Sensitivity of brain circuits to fear Psychological Causes of Anxiety Disorders Behavioralists see anxiety as the result of learning Cognitions regarding danger or uncontrollability Parenting – overprotective and lack of adverse experiences Social Contributions to Anxiety Disorders Reactions to stressful events Social learning Comorbidity of Anxiety Disorders Often co-occuring Share same vulnerabilities 55% comorbidity with depression 50% with additional anxiety disorder 1. Generalized Anxiety Disorder Excessive anxiety/worry about a number of events/activities Worry is difficult to control or stop Worry is not helpful Often about minor things Generalized Anxiety Disorder Restlessness tense muscles concentration problems sleep problems Irritability Fatigue Difficulty focusing attention Generalized Anxiety Disorder Lifetime prevalence = 5% 2x more likely in women Develops early in adulthood Most people do not seek treatment from therapist Is GAD a personality style? Or personality disorder? A risk factor? 80-90% qualify for another disorder What Causes GAD? 1. 2. • • 3. Genes -> first degree relatives 5x likely Differences in physiology Less responsive Except muscle tension Cognitive Influences Drawn to threat cues How do we treat GAD? Medication Benzodiazepines Early = Valium, new = Xanax, Ativan Central nervous system depressants Relieve anxiety but impair thinking, motor performance, induce sleep Many people feel addicted (symptoms quickly return) Psychological Treatments for GAD Lots of treatment but little effectiveness Psychoanalytical: insight & Client centered Several Cognitive treatments Cognitive Therapy – confront worry with images coping strategies Beck & automatic thoughts* Borkovec - confronting worry* Craske’s hybrid treatment* 2. Panic Disorder & Agoraphobia Chills or hot flashes Palpitations, pounding/accelerated heart beat Sweating Trembling/shaking Sensations of smothering/choking Chest pain/discomfort Nausea or other abdominal distress Feeling dizzy, light headed, faint Fear of losing control/going crazy/dying Numbness/tingling sensations What is Panic Disorder? Recurrent and unexpected panic attacks (cued or uncued) Anxiety re: having other attacks (escape/embarrassment) Patients avoid situations where panic attacks may happen (agoraphobia) Withdrawal reduces anxiety Negative reinforcement*** Panic Disorder Lifetime prevalence = 3.5% (without) 2-3x more likely in women Develops during late adolescence/early adulthood Chronic without treatment Many experience panic attacks (8-12%) but no disorder develops Causes of Panic Disorder Genetic influences Biology Psychological Factors in Panic Personality/trait like variables of risk 1. 2. 3. Some people have attacks, no disorder 3 Proposed Variables: A tendency to fear panic attacks A tendency to over interpret unusual body sensations Tendency to respond to fear w/ anxiety symptoms Psychological Factors in Panic 1. 2. A tendency to fear fear Hypervigilant about physiology (looking for fear) May trigger panic attacks Misinterpret body signals as impending panic (e.g. during a walk) Focus on own body, not possible danger Psychological Factors in Panic 3. Anxiety Sensitivity Respond fearfully to symptoms of anxiety Overreact then avoid, then hypervigilant May trigger a panic attack What's the converging info? Reaction to panic makes panic more likely!!! Avoiding Panic (Agoraphobia) Why is withdrawal so bad for panic? Opportunities for corrective feedback are nil How can you know something works if you don’t test it? Treating Panic & Agoraphobia 1. 2. There are 2 ways: Medication Cognitive Behavioral Therapy Medication Antidepressants can reduce panic attacks So do benzodiazepines (anti-anxiety) but they have problems: Symptoms return quickly (short 1/2 life) If stop too quickly, can be worse Thus, can produce dependence Medication 66% do well, if stay on medication 20-50% relapse after discontinuing antidepressants 90% after discontinuing benzodiazepines Cognitive Behavioral Treatment A number of elements: 1. Psychoeducation 2. Anxiety reducing techniques (a toolbox) • • 3. 4. Diaphragmatic breathing Progressive muscle relaxation Distraction, labeling anxiety as safe, challenging thoughts Exposure (!!!) Cognitive Behavioral Therapy We give our clients a “toolbox” Then we give them a chance to use them Education + techniques + challenges Exposures Sometimes we desensitize to internal feelings (e.g. running in place) Panic Control Treatment (PCT) Exposure to sensations that remind of panic Also receive cognitive therapy Address the cognitions re: dangerousness of feared, yet harmful, situations Examples: Shaking head from side to side loosely for 30 sec Breathe through thin straw for 1 minute Hyperventilate for 1 minute 3. Specific Phobias Unreasonable fears of objects, places, situations Anxiety response triggered by specifics Functioning beyond phobia is fine www.phobialist.com Specific Phobias In theory, anything can = phobia Small # account for most: Animal phobias (zoophobia) = 40% Environmental situations (e.g. heights hysphobia) Blood-injection-injury** (vasovagal response) Avg age of onset = 9 years Situational (planes, elevators) Specific Phobias Lifetime prevalence rate = 11% Children experience more Culture can impact Gender ratio 4:1 (women higher) Some may be developmentally normal E.g. strangers, separation, the dark, etc Except heights (equal) Chronic across lifecourse Separation Anxiety Disorder Unrealistic and persistent worry that something will happen to parents OR something will separate child from parents School refusal Nightmares, difficulty sleeping alone Causes of Specific Phobias Not traumatic experiences Often panic attacks trigger Vicariously from others • • • Also genetic role – 31% of people with 1st degree relatives • • Specific to subtype Behavioral Factors & Specific Phobias Classical conditioning - Little Albert Phobias are learned May not need direct experience “modeling” fear of parents Many phobics show no related experience 50% of dog phobics no experience Many people don’t develop after experience Evolution, Learning & Specific Phobias 1. 2. Are we predisposed to certain phobias? Can we learn phobias from others? Evolution, Learning, & Specific Phobias Are we prepared to be phobic of certain things? E.g. snakes Arbitrary objects do not often = phobia (despite danger or instructions) Electric outlets, stoves, hammers Bicycles, etc Evolution, Learning, & Specific Phobias Mineka’s monkeys (1984, Experiment 2) Can lab-born monkeys learn snake phobia from their wild-born parents? Study 1 established that wild-born monkeys were more fearful than their offspring Offspring observed parental response to: real snake, toy snake, neutral objects Behavioral Avoidance of Snakes 60 50 40 Parent Chld Pre Cld Post 30 20 10 0 Real Toy Model Neutral Evolution, Learning & Specific Phobias Offspring learned phobias by watching parents Results were intense & rapid (one try) In evolutionary terms, we don’t have several “tries” with a fatal object Retention 3 months later Evolution, Learning, & Specific Phobias Mineka’s follow-up (Cook & Mineka, 1991) Spliced videos so it appears parent monkeys are reacting to flowers Observer monkeys did not learn flowerphobia This is consistent with the idea that we are prepared for certain phobias How do we treat a specific phobia? 1. 2. Exposure! Two types of exposure: Systematic desensitization Flooding Systematic Desensitization 3. Imaginal vs. in vivo exposure In vivo treats well (75-95% of patients) Create a hierarchy of feared experiences Teach progressive muscle relaxation Combine Note: this is gradual 1. 2. Flooding This is not gradual Intense & prolonged exposure E.g. stay on the roof until you are calm Usually in vivo Emotionally draining Can make anxiety worse if quit early In Vivo Different sizes of spiders Patients stand in room, approach, touch jar, change size of spider, touch spider 3 hour treatment What about imaginal? Some people have problems imagining Imagined spiders might not be scary Virtual Reality Treatment for Anxiety (Garcia-Palacios et al., 2001) Phobias are extremely common & easy to treat but most people never seek treatment Less than 15% of the 10% of the pop. with a phobia Why do VR therapy? 25% refuse exposure-based therapy Too afraid to confront Ost (a spider pioneer) - 90% of spider phobic patients refuse one-session tx How can we improve therapy? Make it less intimidating Use virtual reality! VR Therapy for Phobias The illusion of in vivo Position tracking devices Changing orientation Tactile augmentation “cyber-heft” Present separate images to each eye Why is VR “better”? More control over feared object Therapist controls “fright level” In Vivo can be expensive 1. 2. 3. • 4. 5. E.g in vivo for flying phobias In Vivo can breach confidentiality VR can treat “residual” fears 4. Social Phobia/Social Anxiety Disorder www.socialphobia.org Lifetime prevalence rate is more than 13% 3rd most common disorder That’s 2340 UD students! (depression, alcohol) Men outnumber women (1.4:1) Social Phobia Fear of evaluation socially E.g. public speaking (specific) More common in women Common problems: Meeting new people & talking to authority figures Performing in front of others Dating! Causes of Social Phobia Tend to run in families (nature or nurture?) Generalized may be trait-like Vs. avoidant personality disorder May be classically conditioned May actually be less skilled & more awkward Causes of Social Phobia People with social phobia: Often do things to maintain their anxiety Overestimate negative consequences Think social costs are worse “safety behaviors” Often focus on themselves, not the environment Treatment of Social Phobia: Medications Beta-blockers (lower heart rate, blood pressure) antidepressants Treatment of Social Phobia CBT + Exposure May include roleplaying, skills training Often done in groups Problems inherent to group therapy 5. Post-Traumatic Stress Disorder Long-term response to life-threatening danger (war, rape, robbery, etc) Symptoms can last for years Derealization (emotional numbing) Depersonalization Flashbacks Hyperarousal, agitation, irritable, jumpy 3 Major Types of Symptoms 1. Avoidance 2. Hypervigilance 3. Re-experiencing PTSD Lifetime prevalence = 8% More common in women Many do not develop (so PTSD different) Most events interpersonal Causes of PTSD 1. 2. 3. Nature of the trauma Biological Factors Psychological Factors 1. Nature of the Trauma More traumatic = more PTSD likelihood Level of trauma depends on: Physical reality of the event Individual experience, including closeness to event 2. Biological Factors in PTSD Family history of anxiety disorders Personal history of any disorder Physical symptoms suggest physiological dysfunction Dysregulation of natural opiods Changed sleep cycles Immune/metabolic suppresion 3. Psychological Factors Previous trauma Social support is a buffer Lots of individual differences Treating PTSD Antianxiety drugs + sleep aids (control physiological symptoms) Psychological treatment Exposure Rethinking of experience Can be done in groups 6. Obsessive-Compulsive Disorder Obsessions: unwanted, intrusive thoughts that cannot be controlled Compulsions: Behaviors one feels compelled to perform (may reduce obsessions) OCD Compulsions can also be called rituals Obsessions increase anxiety, compulsions temporarily reduce OCD We used to believe this was extremely rare Hiding symptoms Many can appear to function normally Most did not seek treatment Lifetime prevalence 2.6% As common in children Some normal (10-15% college students) OCD Common Compulsions: Washing Checking & Counting rituals Common Obsessions: Harming others (Sexually, physically) Safety of others Contamination of self & others Principal Symptom Factors 1. Aggressive, sexual, and religious obsessions with checking compulsions 2. Symmetry/Order obsessions with ordering, arranging, and repeating compulsions (Leckman et al., 1997) Principal Symptom Factors 3. Contamination obsessions with washing and cleaning compulsions 4. Hoarding and Saving symptoms OCD Usually aware of “silliness” but can’t stop (anxiety will skyrocket) Subtype with a lack of insight Some things not to misunderstand: Compulsions are not set (can change) Some people can have obsessions OR compulsions Causes of OCD 1. 2. 3. Psychodynamic Factors Biological Factors Cognitive & Behavioral Factors Biological Factors 5-10x more likely in first degree relatives Rates in identical twins 20x general pop. Found in Tourettes (a strong genetic component) Brain dysfunction: failure to filter repetitive impulses? Cognitive-Behavioral Factors Black & White thinking? E.g. contamination risks (if no guarantee, then I’m not touching it) The ‘normal’ level of acceptance of risk is too high Magical Thinking Thoughts/actions have specific consequences “If I don’t do this, my partner will die” Cognitive Factors Thought-action fusion Thoughts are equated with the actions or activity represented by the thoughts How do we treat OCD? 1. 2. 3. Medication Exposure/Response Prevention Psychosurgery Medication for OCD Antidepressants (in higher doses) This means serotonin is likely involved Most people respond well Also a subset who will not respond Exposure/Response Prevention Exposure is key to almost all anxiety treatments When we do something scary over and over and over and over and over and over and over again, is it still scary? Exposure/Response Prevention Put clients in an anxiety provoking situation Block their response (compulsion) E.g. touching public toilets/sinks Forbid them to wash their hands The more you give into OCD, the stronger the symptoms become The more you resist, the weaker they become Special Cases of OCD: Hoarding Hoarding: acquisition of, and inability to discard, worthless items, though they appear to have no value (18-24% of OCD patients) Also common in other disorders: Schizophrenia Dementia Eating disorders Mental retardation Features Associated with Hoarding Indecisiveness Perfectionism Procrastination Difficulty organizing tasks Avoidance Obsessions: losing important items, distortion re: importance, emotional attachment to items Treatment of Hoarding Worse prognosis & more disability Intensive CBT (e.g., daily) ERP Excavation of saved material (w/ rules - no sorting, grab first pile) & with help Decision-making training - what to keep? Immediately needs a place Cognitive restructuring - nothing terrible happens Anxiety Disorders Conclusions Anxiety disorders, combined, are relatively prevalent Easy to treat Many people do not seek treatment Usually treated with exposure (and maintained by avoidance and negative reinforcement)