Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Electrocardiography wikipedia , lookup
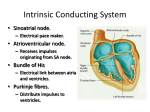
Pacemaker Therapy and the Conducting System of the Heart By: Tom Kerrigan Conducting System of the Heart • Consists of the sinoatrial node (SA node), atrioventicular node (AV node), the bundle of His, the bundle branches and the Purkinje fibers. Sinoatrial node • The natural pacemaker of the heart. • Small mass of specialized cells in the right atrium of the heart. • Creates electrical impulses and conducts them through the myocardium until it reaches the atrioventricular node (~0.03 seconds) Atrioventricular Node • Cluster of cells situated on interatrial septum close to the tricuspid valve. • Receive impulses from the SA node and conducts them to the bundle of HIS. • Must be conducted though the AV node because the atria and ventricles are separated by a fibrous connective tissue septum that has poor conductivity. • AV node slows down electrical current to insure that the atria have fully contracted before ventricles are stimulated. Bundle of HIS • Emerges from the AV node to begin the conduction to the ventricles. • located in the proximal interventricular septum • Branches into three bundle branches. Bundle Branches • Runs along the interventricular septum • Three bundle branches: the right, left anteriosuperior and left postrioinferior bundle branches. • Known as the trifascular system. • Bundles give rise to thin filaments known as Purkinje fibers Purkinje Fibers • Distribute impulse to ventricular muscle, causing the myocardium to contract at a paced interval. • The bundle branches and purkinje network comprises the ventricular conduction system. • It takes ~ 0.03-0.04s for the impulse to travel from the bundle of His to the ventricular muscle. Normal Conduction Dysfunctions of Conduction System • SA node • The signal starts in the SA node but may be slow or delayed in progressing to the atria, causing a very slow or irregular heart beat. (bradycardia) • AV node • Atrioventricular block occurs when atrial impulses fail to reach the ventricles or when atrial impulses are conducted with a delay, leading to partial or complete heart failure. • SA/AV node • SA node sends out electrical impulses too slowly and impulses are partially or fully blocked between the atria and the ventricles. The combination of SA and AV node defects cause uncoordinated contraction of atria and ventricles. Treatment • Implantation of artificial pacemaker to monitor the electrical activity of the heart and respond appropriately. History of Pacemaker • The first artificial pacemaker was designed and built in 1950 by the Canadian electrical engineer, John Hopps. • It was not implanted into the body and relied on external electrodes that had to be plugged into a wall outlet. • Patient could go only as far as the extension cord and a power blackout was of constant concern. • In 1958 the first pacemaker was implanted into the body which had a battery life of ~12 to 18 months. Parts of Pacemaker • Pulse generator • Has a depth of ½” and a width of about 1 ½”. • Produces impulses and houses the electrical circuitry. • Constructed of titanium and contains a lithium battery with a life of ~5 to 10 years • The battery will provide a low warning months before it has fatigued. • Generator sends out electrical impulses through leads that are attached to the myocardium. Parts of Pacemaker • Lead(s) • Insulated wires that not only receive impulses, but carry signals back from the heart to the generator. • Lead(s) are steroid eluting to decrease the inflammation of the interface between the distal tip of the lead and myocardium. Parts of Pacemaker Pacing Systems • Fixed Rate • Emits electrical stimuli at a constant frequency regardless of the hearts rhythm. • Used if heart is able to increase its rate according to the person’s needs. • The pulse rate is set and programmed by the physician. Pacing systems • Rate-Responsive • Has capability to interpret the body’s changes and increase or decrease the heart rhythm at an appropriate rate. • Used when the heart cannot increase its rate with activity. • Most pacemakers today are rate-responsive. Single-Chamber Pacemaker for SA Node Dysfunction • Has one lead that is placed into the right atrium. • Must have a normal conduction of the AV node. • Can only send and receive signals from right atrium. • Candidates for this type of pacing usually have symptomatic bradycardia. • Disadvantage of this pacing method is that AV block develops in 0.6 to 5.0% of patients with symptomatic bradycardia every year. Single-Chamber Pacemaker for SA Node Dysfunction Single-Chamber Pacemaker for AV Node dysfunction • Has one lead placed into right ventricle to be effective. • Must have a normal SA node conduction. • Patients with this type of pacing typically have atrial impulses that delay or fail to reach the ventricles. • Ventricular pacing can be associated with pacemaker syndrome. This occurs when the right ventricle sacrifices the atrial contribution to the ventricle output. This is due to atrial contraction against closed atrioventricular valves. • The ultimate treatment involves an upgrade to a dualchamber pacemaker. Single-Chamber Pacemaker for AV Node Dysfunction Dual-Chamber Pacemaker for SA and AV Node Dysfunction • More sophisticated and costly than singlechamber pacemaker. • Has two leads, with one leading into the right atrium and one in the right ventricle. • Can pace and sense the both right chambers of the heart. • Beneficial for patients that have acquired symtomatic bradycardia and partial or complete block of the heart. Dual-Chamber Pacemaker for SA and AV Node Dysfunction Implantation procedure • A small 2 to 3” incision is made parallel to and just below the clavicle in the deltopectoral groove. • Small pocket will be made under skin for generator and lead(s). • Under fluoroscopy, lead(s) travel through the subclavian vein, brachiocephalic vein, superior vena cava, and finally into the desired chamber. • Physician will create an arrhythmia to insure the pacemaker is responding appropriately. • Hospitalization usually last 1 to 3 days. Devices That Put Your Pacemaker at Risk • MRI and large amounts of radiation can interrupt the circuitry. • If an MRI must be done, the pacemaker output in some models can be reprogrammed. • If exposed to excessive amounts of radiation, it should be shielded as much as possible. • Diagnostic radiology appears to no effect towards pulse generators. CXR’s are actually beneficial to evaluate lead position. The Future of Pacemakers • There are currently more than 3 million patients worldwide with an implantable pacemakers, and indications are expanding. • Major advancements of pacemaker technology has enabled patients with life threatening symptoms to increase their survival and live a higher quality of life.