Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Antihypertensive drug wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
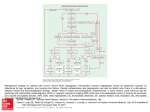
Cardiac Board Review Part 1 A 20-year-old female college student is evaluated at the student health center to establish care. She had no major medical problems prior to college, and there is no family history of cardiovascular disease. BP: 110/60 mm Hg and pulse is 70/min. S1 and S2 are normal and there is an S4 present. There is a harsh grade 2/6 midsystolic murmur heard best at the lower left sternal border. The murmur does not radiate to the carotid arteries. A Valsalva maneuver increases the intensity of the murmur; moving from a standing position to a squatting position, performing a passive leg lift while recumbent, and performing isometric handgrip exercises decrease the intensity. Rapid upstrokes of the carotid pulses are present. Blood pressures in the upper and lower extremities are equal. 100% Which of the following is the most likely diagnosis? 1. 2. 3. 4. 5. Aortic Coarctation Bicuspid Aortic Valve Hypertrophic Cardiomyopathy Mitral Valve Prolapse Ventricular Septal Defect 1 0% 0% 2 3 0% 0% 4 5 Hypertrophic Cardiomyopathy • • Abnormal diastolic function with preserved systolic function Murmur: midsystolic harsh murmur caused by turbulent flow and obstruction of the LV outflow track – Murmur increased with Valsalva or standing – Murmur decreased with hand grip, squatting • Dx: – EKG: LV hypertrophy and strain and Q waves that mimic an MI – Echo – Cardiac MR: ventricular hypertrophy and areas of scarring • Screening: – Echo screening for first degree relatives • Tx: – Avoid strenuous exercise, intense isometric exercise – Symptomatic patients or pts with high risk of cardiac death (prior arrest, sustained VT, FHx of sudden death): B-blockers first line. Verapamil and disopyramide are second line. – ICD for pt with increased risk of sudden death – Myomectomy/alcohol ablation for refractory symptoms A 76-year-old woman residing in an independent living facility is evaluated during a routine examination. She ambulates well, using a cane because of hip pain, but does not exercise regularly and takes public transportation to complete her daily shopping. She does not have exertional chest discomfort, dizziness, palpitations, dyspnea, or fatigue. She has hypertension. There is no known history of coronary artery disease. She does not smoke. Medications are hydrochlorothiazide and low-dose aspirin. On physical examination, temperature is normal and blood pressure is 150/80 mm Hg. BMI is 22. Cardiac examination reveals a sustained apical impulse; normal S1; and a single, soft S2. An S4 is present. There is a grade 3/6 early-onset systolic, late-peaking murmur that is heard best at the right upper sternal border and radiates to the left carotid artery. Carotid pulses are delayed. There is trace pedal edema. Transthoracic echocardiography demonstrates severe aortic stenosis. No other 100% valvular abnormalities are seen. Biventricular function is normal. There is concentric left ventricular hypertrophy. Pulmonary pressures are at the upper limits of normal. Which of the following is the most appropriate test to perform next? 1. 2. 3. 4. 5. Cardiac CT angiography Coronary angiography Exercise Treadmill Stress Test Transesophageal echocardiography No diagnostic testing at this time 0% 1 0% 2 3 0% 0% 4 5 Valvular Heart Disease • Midsystolic murmurs grade 1-2/6 are usually benign • Diagnosis: – TTE for symptomatic pts, systolic mumur 3-6/6, continuous murmur, diastolic murmur – TEE for severe mitral regurgitation, prosthetic valves, endocarditis and evaluation of LA appendage – When symptoms or physical exam findings are discrepant from echo findings, do BNP and exercise testing with echo. • Asymptomic pts with severe disease having other cardiac surgery should undergo surgical valve correction Valvular Heart Disease • Right sided murmurs and heart sounds are louder during inspiration. – The ejection click heard with Pulmonic Stenosis disappears with inspiration • Stand-to-squat maneuver and passive leg lift transiently increase venous return (preload) increases left ventricular chamber size and volume. – Increases most murmurs, but decreased HCM and MVP • The Valsalva maneuver and the squat-to-stand maneuver decrease venous return – Decreases most murmurs, but increases HCM and MVP • Handgrip exercise increases afterload and decreases the relative pressure gradient across the left ventricular outflow tract – Decreases HCM and AS, but increases MVP Valvular Heart Disease S2: results from aortic and pulmonic valve closure at end of ventricular systole Physiologic split= P2 closes after A2 during inspiration, but they close at the same time during expiration. This is NORMAL. Persistently split (widened S2)= Pulmonic stenosis, Mitral regurgitation Fixed split= splitting does not vary with inspiration. ASD Paradoxically split S2= LBBB, HCM Aortic Stenosis • Calcification of tricuspid valve or bicuspid valve – Pts with bicuspid valve should be evaluated for aortic arch dilation with echo • Sx: angina, syncope, heart failure • Murmur: mid to late peaking systolic murmur to the carotids, S4, single S2, pulsus parvus et tardus – Murmur louder with squatting – Standing and valsalva decrease the murmur AS Management • ASYMPTOMATIC patients – Monitor with serial echos • Severe AS (area <1.0 cm2): yearly echos • Moderate AS: echos every 2 years • Mild AS: echos every 5 years – Valve replacement if • undergoing other cardiac surgeries • severe AS and EF <50% • hypotension develops during exercise testing • SYMPTOMATIC patients – Valve replacement Hypertrophic Cardiomyopathy Carotid Pulse Valsalva or SquatStand Stand Squat Carotid radiation Pulsus Bisferiens Aortic Stenosis Pulsus Parvus et tardus Acute Aortic Regurgitation Most common causes are dissection and valve destruction from endocarditis. • Murmur: short diastolic • Dx: TTE; do TEE/CT/MRI if dissection suspected as cause • Tx: IMMEDIATE surgery; avoid IABP Chronic Aortic Regurgitation Results from annular dilation or primary leaflet dysfunction. • Murmur: decrescendo diastolic high pitched blowing, soft S1, enhanced when leaning forward • Wide pulse pressure and bounding pulse • Tx: – ASYMPTOMATIC: • monitor with echos (6-12 months if LV dilation or 2-3 yrs with normal LV) • AV replacement if EF <50% or abnormal hemodynamic response to exercise, undergoing other cardiac surgery – SYMPTOMATIC: • AV replacement Mitral Stenosis • Caused by rheumatic valve disease. • Murmur: diastolic low rumbling murmur with a diastolic opening snap; loud S1 • CXR and EKG demonstrate LAE and normal LV • Tx: – ASYMPTOMATIC: • monitor with echo – SYMPTOMATIC: • Valvotomy • Valve replacement if pt with severe mitral regurgitation Mitral Regurgitation • Acute: from chordae tendineae rupture from endocarditis or papillary mm rupture from MI – HF, shock, pulm edema – Murmur: holosystolic radiates to axilla – Tx: Urgent Surgery • Chronic: from MVP and endocarditis – Murmur: holosystolic murmur, radiates laterally and posteriorly, widely split S2, S3 and increased P2 – Tx: diuretics, BB, ARB/ACEi • ASYMPTOMATIC: monitor with echos; MV repair if EF <60% • SYMPTOMATIC: MV repair (annuloplasty) MVP • Systolic buckling of MV leaflets into the LA; MR occurs if faulty leaflet coaptation • Murmur: high pitched midsystolic click with late systolic murmur – The click moves earlier in systole with standing and valsalva (unlike click with PS which is fixed) – Squatting delays the click and murmur Character Comment SYSTOLIC Aortic Stenosis Midsystolic ejection Hypertrophic Cardiomyopathy Mid to late systolic Mitral Valve Prolapse Late Systolic Mitral Regurge Holosystolic VSD Holosystolic Midsystolic click DIASTOLIC Aortic Regurge Early, high pitched Mitral Stenosis Low pitched rumble Opening snap, Diastolic click Endocarditis • Prophylaxis: Amoxicillin (clinda or azithro if pcn allergic) indicated for dental procedures (no longer indicated for GU/GI procedures), invasive procedure of the respiratory tract and surgery on infected soft tissues: – Prosthetic valves – Previous episode of endocarditis – Congenital Heart Disease: unrepaired, repaired with residual defects or within 6 months of procedure – Cardiac Transplant pts with valve lesions – NO prophylaxis for bicuspid aortic valve, MVP A 54-year-old man is evaluated for right-sided chest pain that is described as sharp, begins following large meals, lasts for several minutes, and usually resolves spontaneously. The episodes are not clearly related to activity, nor are they relieved by rest. He has been experiencing the pain for about 4 months. Several of the episodes have resolved with antacids. The most recent episode, which occurred yesterday while walking, lasted 20 minutes and resolved. Medical history includes hypertension and hyperlipidemia. Family history is notable for a brother who had coronary stent placement at the age of 43 years. Current medications are aspirin, atenolol, and atorvastatin. Physical examination is notable for estimated central venous pressure of 6 cm H2O; normal carotid upstroke; and no cardiac murmurs, rubs, or S3. Lung fields are clear. Extremities show no edema, and peripheral pulses are normal bilaterally. Hematocrit, 44%; troponin I at presentation is 0.0 ng/mL; troponin I at 4 hours is 0.0 ng/mL ; creatine kinase, 50 U/L. EKG: shows normal sinus rhythm and no ST- or T-wave changes. CXR: shows a normal cardiac silhouette, no infiltrates, and no pleural effusions. 100% Which of the following is the best diagnostic option? 1. 2. 3. 4. Coronary angiography Esophagogastroduodenoscopy Exercise stress test Empiric treatment with a proton pump inhibitor 0% 1 0% 2 0% 3 4 A 68-year-old woman is evaluated for atypical chest pain of 3 months’ duration. She describes the pain as a left-sided burning that occurs both at rest and when she exercises. It lasts for about 10 minutes, and is relieved by rest and eating. The patient has no history of cardiac disease. She has hypertension, for which she currently takes hydrochlorothiazide. She is a smoker and she has asthma, for which she takes inhaled corticosteroids and frequently uses inhaled bronchodilators. If she pretreats herself with the inhaled bronchodilator, she can walk long distances at a brisk pace. She is afebrile, her blood pressure is 158/84 mm Hg, her pulse is 64/min, and her respiration rate is 18/min. Estimated central venous pressure is 5 cm H2O. On cardiac examination, no murmurs, rubs, or extra heart sounds are noted. The lungs are clear to auscultation. There is trace peripheral edema. Total cholesterol, 200 mg/dL LDL 140; and HDL 50 mg/dL EKG: normal Which of the following is the most appropriate diagnostic test for this patient? 1. 2. 3. 4. 5. Adenosine nuclear perfusion stress test Coronary angiography Coronary artery calcium score Dobutamine stress echocardiography Exercise stress test Diagnostic test for CAD Exercise Treadmill Testing: 1. 2. 3. EKG: Good for testing functional capacity, ischemia and prognosis; it will NOT localize ischemia Echo: indicates wall motion abnormalities that indicate ischemia Nuclear myocardial perfusion: determine the area of ischemia and if its reversible. Pharmacologic Stress Testing: 1. 2. 3. Dobutamine echo Dobutamine nuclear perfusion Adenosine nuclear perfusion Other: 1. 2. 3. 4. Coronary angiography Coronary artery calcium testing: risk stratify asymptomatic pts at intermediate risk with strong family history Coronary CT imaging CMR imaging Diagnosing CAD 1. Pretest probability of having CAD a) Categorize the nature of the chest pain b) Estimate the pretest probability of CAD based on sex, age, and character 2. Determine if patient can have an exercise test based on their abilities and comorbidities 3. If doing an exercise study, look at the findings on resting EKG 1. Pretest probability of having CAD a) Categorize the nature of the chest pain: 1. Typical Chest Pain: 3 of 3 1. Substernal chest pain or discomfort 2. Provoked by exertion or emotional stress 3. Relieved by rest and/or nitroglycerin 2. Atypical Chest Pain: 2 of the 3 3. Non-anginal Chest Pain: none of the components 1. Pretest probability of having CAD b) Estimate the pretest probability of CAD based on sex, age, and character Low Probability Intermediate Probability High Probability Asymptomatic M and W of all ages Men of all ages with atypical CP Men > 40 with typical CP Women <50 with atypical CP Women >50 with atypical CP Women >60 with typical CP Women < 60 with typical CP •Low risk: no further testing •Intermediate risk: Noninvasive stress test •High risk: begin medical therapy for CAD 2. Can they have an exercise test? • If patient can exercise exercise stress • If patient cannot exercise because of arthritis, severe pulmonary disease or physical deconditioning or with a pacemaker pharmacologic stress – Adenosine/Dipyridamole: Contraindicated with: bronchospastic airway disease, theophylline use, baseline 2nd degree Heart Block – Dobutamine: Contraindicated with: severe hypertension or arrhythmias. Must hold BB before test. • If patient cannot exercise because of the following comorbidities pharmacologic stress: – – – – – – Recent MI or UA Uncontrolled arrhythmias Symptomatic severe aortic stenosis Decompensated heart failure Acute PE Aortic dissection 3. If doing an exercise study, look at the findings on resting EKG If resting EKG ST changes or with any of the following: • WPW • Greater than 1mm ST depression • LBBB • Paced rhythm Must do echo or nuclear myocardial perfusion as the diagnostic test. A 65-year-old man is evaluated during a routine follow-up examination for coronary artery disease. He was diagnosed with a myocardial infarction 5 years previously, and was started on medical therapy with aspirin, metoprolol, atorvastatin, lisinopril, and sublingual nitroglycerin. He was asymptomatic until 3 months ago, when he noted progressive exertional angina after walking two blocks. He now uses sublingual nitroglycerin on a daily basis. He has not had any episodes of pain at rest or prolonged chest pain that were not relieved by sublingual nitroglycerin. He has hyperlipidemia and hypertension. PE: a well-developed man who appears comfortable. BP 140/60 mm Hg HR 85/min. Carotid upstrokes are normal with no bruits. Cardiac examination reveals no murmurs. The lungs are clear. Peripheral pulses are equal throughout and there is no peripheral edema. His electrocardiogram is unchanged since the last visit, with no evidence of acute changes. In addition to adding a long-acting nitrate, which of the following is the most appropriate management for this patient? 100% 1. 2. 3. 4. Add ranolazine Increase metoprolol Coronary angiography Exercise treadmill stress testing 0% 1 0% 2 3 0% 4 Contraindications for BB: bradycardia, severe depression, decompensated HF, severe restrictive airway disease Contraindications for long acting nitrate: severe AS, HCM, PDEi Contraindications for ranolazine: hepatic impairment, QT prolongation or if pt on dilt, verapamil PCI does NOT decrease future cardiovascular events or increase survival, it does decrease frequency and severity of anginal symptoms CABG for: - Severe L main disease - 3 vessel disease - 2 vessel disease (prox LAD) with reduced LV function - DM with multivessel disease A 66-year-old man is evaluated in the emergency department for left-sided chest pain that began at rest, lasted for 15 minutes, and has since resolved. A similar episode occurred at rest yesterday, and multiple similar episodes that were associated with exertion have occurred over the past 2 weeks. Pertinent medical history includes hypertension and type 2 diabetes mellitus. Family history is notable for his father undergoing coronary artery bypass graft surgery at age 69 years and his brother undergoing coronary artery bypass graft surgery at age 54 years. Current medications are amlodipine, glyburide, and aspirin. BP 125/65 mm Hg, HR 70/min, RR 12/min. Estimated central venous pressure is 6 cm H2O, carotid upstroke is normal, there are no cardiac murmurs, and the lung fields are clear. Extremities show no edema, and peripheral pulses are normal bilaterally. Troponin I level of 1.2 ng/mL and a creatinine 1.4 mg/ dL EKG: 1-mm ST-segment depression in leads aVL, V5, and V6. CXR: normal cardiac silhouette, with no infiltrates and no pleural effusions. The patient is treated with aspirin, intravenous nitroglycerin, unfractionated heparin, metoprolol, and pravastatin. 100% Which of the following should be the next step in this patient’s management? 1. 2. 3. 4. Coronary angiography Obtain B-type natriuretic peptide level Pharmacologic stress testing Thrombolytic therapy 0% 1 0% 2 3 0% 4 A 65-year-old woman is evaluated in the hospital 36 hours after presenting in the emergency department with midsternal chest pain. Electrocardiogram on presentation demonstrated no ST-segment shifts, but T-wave inversion was present in leads V3 and V4. She was given nitroglycerin, unfractionated heparin, and a glycoprotein IIb/IIIa inhibitor and was admitted to the hospital. She has a history of hypertension and hyperlipidemia and is a prior smoker. Her medications prior to admission were metoprolol, 25 mg twice daily; atorvastatin, 80 mg/d; and aspirin, 325 mg/d. The patient is afebrile. BP 132/82 mm Hg, HR 68/min and regular, RR 16/min. BMI is 25. There is no jugular venous distention, and no crackles are auscultated. Heart sounds are normal. There is no rub, murmur, or gallop. Her serum cardiac troponin I level rose to a peak of 4.2 ng/mL at 24 hours following the index event. Results of a basic metabolic profile, including blood glucose levels, are normal. Coronary angiography demonstrates diffuse, mild luminal irregularities in all coronary arteries, along with diffuse severe disease in the distal left anterior descending coronary artery not amenable to percutaneous coronary intervention. Left ventriculography demonstrates a left ventricular ejection fraction of 55% with a small focal region of hypokinesis in the apex. The left ventricular end-diastolic pressure is 12 mm Hg. The glycoprotein IIb/IIIa inhibitor is discontinued. Which one of the following agents should be added to this patient’s medication regimen? 1. 2. 3. 4. Verapamil Clopidogrel Eplerenone Warfarin Acute Coronary Syndromes • STEMI: ST segment elevation (or new LBBB) with elevated enzymes • NSTEMI: ST segment depression, T wave inversion, or nonspecific EKG with elevated enzymes • Unstable Angina: Nonspecific EKG findings and normal enzymes NSTEMI/UA TIMI: • Age >65yo • > 3 CAD RF • Coronary obs >50% • ST segment deviation • > 2 anginal episodes in last 24 hours • Aspirin use in last week • Elevated biomarkers High/Intermediate Risk (TIMI > 3) • Aspirin • B-blockers: – Avoid in decompensated HF, sBP <90, bradycardia with HR <50, or second degree AV block – Can use CCB (except nifedipine) in those with CI to BB and in those with continued angina despite optimum BB and nitrates • • • • Nitro Clopidogrel Glycoprotein IIb/IIIa inhibitors (tirofiban, eptifibatide, abciximab) Unfractionated heparin, low molecular weight heparin, or direct thrombin inhibitor (bivalirudin) – Avoid low molecular weight heparin in renal failure • High dose statin • Coronary Angiography Low Risk (TIMI 0-2) • • • • • Aspirin B-blockers Nitro Clopidogrel Unfractionated heparin, low molecular weight heparin, or direct thrombin inhibitor (bivalirudin) • High dose statin • Predischarge stress test A 67-year-old woman is evaluated in the ED for substernal chest pressure that has lasted for just over 3 hours. The pressure has not remitted despite administration of one dose of sublingual nitroglycerin on the way to the hospital. The emergency department is in a community hospital that does not have percutaneous coronary intervention (PCI) capability. The nearest hospital with PCI capability is 45 minutes away. The patient has a history of hypertension and hyperlipidemia. There is no history of recent surgery or bleeding diathesis. Current medications include lisinopril, hydrochlorothiazide, and simvastatin. She has no known drug allergies. Aspirin and sublingual nitroglycerin are administered upon arrival. Temperature is 37.2 °C (99.0 °F), BP 146/92 mm Hg, HR 104/min and regular, RR 18/min. The patient appears uncomfortable. Crackles are heard at the bases of both lung fields. The S1 is normal; the S2 is paradoxically split. No murmur or gallop is present. Results of a complete blood count, basic metabolic profile, and clotting studies are normal. Initial serum troponin I level is 0.5 ng/mL. A stool sample tests negative for occult blood. EKG: normal sinus rhythm with a left bundle branch block. No prior tracing is available for comparison. Intravenous heparin, β-blockers, and morphine are administered. Which of the following is the most appropriate next step in the management of this patient? 1. 2. 3. 4. Administer thrombolytics Administer glycoprotein IIb/IIIa Obtain serial cardiac enzyme measurements Transfer to nearest hospital with PCI capability A 62-year-old woman is brought to the emergency department by paramedics for chest pain that has been present for 5 hours. Medical history is notable for type 2 diabetes mellitus, hypertension, and a stroke 1 year ago. Medications include glyburide, lisinopril, atorvastatin, and aspirin. On physical examination, she appears comfortable. She is afebrile, blood pressure is 190/90 mm Hg, pulse rate is 88/min and respiration rate is 16/min. Cardiac examination shows no murmurs, extra sounds, or rubs. The lungs are clear and pulses are equal bilaterally. Neurologic examination is normal. The electrocardiogram shows 2-mm ST-segment elevation in leads II, III, and aVF. A coronary catheterization laboratory is not available, and the nearest hospital with percutaneous intervention capability is 1 hour away. Which of the following is the best management option for this patient? 100% 1. Aggressive medical therapy without reperfusion attempt 2. Immediate thrombolytic therapy 3. Transfer for coronary artery bypass graft surgery 4. Transfer for percutaneous coronary intervention 0% 1 0% 2 3 0% 4 STEMI management • Initiate medical therapy: aspirin, clopidogrel, BB, nitrates, heparin, statins – ACEi with reduced EF • Decide on reperfusion therapy. Evaluate: – Contraindications to thrombolytics: PCI preferred – If > 3 hours from symptom onset: PCI preferred – High risk features (shock or HF or h/o CABG): PCI preferred • If facility without onsite PCI: give thrombolytics, place IABP and transfer to PCI facility – Time to achieve balloon inflation • Door to balloon time: < 90 minutes • Door to needle time: < 30 minutes – If facility without onsite PCI, transfer to facility with PCI capability only if they can undergo PCI within 90 minutes of first medical contact (medical contact to balloon time) Contraindications to Thrombolytics • Absolute: – – – – – previous hemorrhagic stroke any time or any CVA within 3 months Intracranial neoplasm or cerebrovascular lesion Active internal bleeding Suspected aortic dissection Closed head or facial trauma within last 3 months • Relative: – – – – – – – BP >180/110 INR >2-3 Recent major trauma (2-4 wks) Pregnancy Active peptic ulcer Non-compressible vascular puncture Any stroke history Thrombolytics • Continued CP, lack of ST elevation improvement, hemodynamic instability, and ventricular arrhythmias indicate failure of thrombolytics rescue PCI • Improvement in ST elevation >50% on EKG obtained 60 min after therapy indicates successful reperfusion. – Reperfusion arrhythmias (accelerated idioventricular arrhythmia) indicate successful thrombolysis • Must risk stratify prior to discharge: – Echo or nuclear imaging to assess LV function • EF <40% angiography – Pharmacologic stress test • Significant ischemia angiography An 85-year-old woman is admitted to the coronary care unit following successful thrombolytic therapy for an acute anterior wall STEMI. Prior to the myocardial infarction she had been active without any medical problems and was taking no medications. BP 120/70 mm Hg and heart rate is 90/ min. There is no jugular venous distention and no cardiac murmurs. The lung fields are clear and there is no peripheral edema. Medications started in the hospital are aspirin, low-molecular-weight heparin, intravenous nitroglycerin, and oral metoprolol. EKG shows Q waves in the anterior leads with upsloping ST segments. On hospital day 3, the patient experiences acute onset of respiratory distress, and her systolic blood pressure falls to 80 mm Hg. Her oxygen saturation remains at 80% despite the administration of 100% oxygen by face mask. She is given dopamine and intravenous furosemide. On physical examination, blood pressure is 96/40 mm Hg, pulse rate is 100/min, and respiration rate is 28/min. Findings include jugular venous distention, crackles throughout both lung fields, and a grade 4/6 systolic murmur associated with a thrill. A pulmonary artery catheter is placed via the right internal jugular vein. The pulmonary capillary wedge pressure tracing shows prominent v waves Which of the following is the best immediate treatment option? 1. 2. 3. 4. Mitral valve repair Pericardiocentesis Pulmonary artery thrombectomy Ventricular septal defect repair Complications after MI • RV infarction: hypotension, clear lungs and elevated JVD in setting of inferior wall MI – DX: R sided EKG and echo – Tx: IVF, dobutamine and PCI. Avoid nitrates and preload reducing agents • Arrhythmias and blocks • Mechanical complications: – Rupture of papillary muscle with mitral regurge: 3-7days after inferior MI. Pt develops shock. Short early systolic murmur. – VSD: 3-7days after anteroseptal MI. Shock. Loud, holosystolic mumur with a thrill – LV free wall rupture: 3-7 days after anterior MI. Syncope and tamponade – LV thrombus: most common with anterior MI. Anticoagulate for 3-6 mo to treat. A 67-year-old business man is evaluated during a routine health examination. He has a 30 packyear history of smoking, but quit 5 years ago. He consumes two or more alcoholic beverages on most days. He is asymptomatic, but performs no regular physical exercise. He takes no medications. On physical examination, his blood pressure is 148/92 mm Hg and heart rate is 78/min and regular. His pulses are full, he has no bruits, and results of his lung, heart, abdominal, and rectal examinations are unremarkable. Total serum cholesterol is 240 mg/dL (6.2 mmol/L), HDL cholesterol is 40 mg/dL (1.0 mmol/L), and triglyceride level is 100 mg/dL (1.1 mmol/L). Results of other serum laboratory studies are normal. An abdominal ultrasound for screening purposes demonstrates an infrarenal abdominal aortic aneurysm measuring 4 cm in diameter. In addition to treatment of this patient’s hyperlipidemia and hypertension and discussion about his at-risk drinking, which of the following is the best management option? 1. 2. 3. 4. Abdominal CT with IV contrast Antithrombotic therapy Follow up US in 6-12 months Placement of endovascular stent graft Thoracic Aortic Aneurysm • Serial CT or MRI for surveillance • Tx: B-blockers or ARBs – Surgical Repair if: • • • • symptoms (hoarseness, dysphagia, back pain) Dissection rapid growth (>1 cm/yr) Severe dilation (>5 cm ascending or >6 cm descending) Abdominal Aortic Aneurysm • Screen with US in men 65-75 yo who have ever smoked • US q6-12 months for AAA >4cm • Tx: – Surgical Repair: • AAA >5.5 cm • Progression of > 0.5cm per year • Ruptured AAA signs: abdominal/back/flank pain, hypotension, syncope or shock. – Dx: CT or MRI (US is not accurate for diagnosis) A 48-year-old man is evaluated in the emergency department for sudden onset of severe discomfort in the chest and between the shoulder blades. The pain was maximal in intensity at its onset 90 minutes ago and is unaffected by position or breathing. He has a history of hypertension, for which he takes hydrochlorothiazide, 25 mg/d; and lisinopril, 40 mg/d. BP is 200/120 mm Hg, pulse is 100/min, and respiration rate is 20/min. An S4 gallop is present. No cardiac murmur or pericardial rub is present. The lungs are clear to auscultation. Distal pulses are equal and symmetric. Results of a neurologic examination are normal. UDS: positive for cocaine. Serum creatinine is 2.2 mg/dL. His creatinine 0.8 mg/dL at the time of his last office evaluation. Serum cardiac troponin and myoglobin levels are normal. An electrocardiogram reveals left ventricular hypertrophy with a secondary repolarization abnormality and sinus tachycardia. Chest radiograph is normal. In addition to emergently lowering the blood pressure and heart rate, which of the following diagnostic tests should be performed next? 1. 2. 3. 4. CT scan of chest with intravenous contrast Nuclear myocardial perfusion scan Transesophageal echocardiogram Ventilation-perfusion lung scan Aortic Dissection • Dx: – CT – MRI – Trasesophageal echo • Type A: ascending aortic arch – Surgical emergency • Type B: distal to L subclavian artery. – Tx medically with IV B-blockers with goal HR 60-80. – Monitor at 1,3,6 months then q6-12 months if aneurysmal dilation present