Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Brucellosis wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Meningococcal disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Tuberculosis wikipedia , lookup
Chagas disease wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Sarcocystis wikipedia , lookup
Hepatitis C wikipedia , lookup
Trichinosis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Leishmaniasis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Hepatitis B wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Candidiasis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Schistosomiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
PATHOLOGY OF
BACTERIAL INFECTIONS
GRAM POSITIVE BACTERIAL
INFECTIONS
Common gram-positive pathogens include:
Staphylococcus,
Streptococcus,
Enterococcus,
Less common diseases caused by gram-positive rod-shaped
organisms:
diphtheria,
listeriosis,
anthrax, and
nocardiosis.
Clostridia, which are gram-positive, are discussed with the
anaerobes. All these infections are diagnosed by culture and
some special tests mentioned below.
Staphylococcal Infections
Staphylococcus aureus are pyogenic
gram-positive cocci that form clusters like
bunches of grapes.
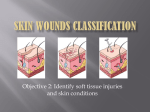
These bacteria cause a myriad of skin
lesions (boils, carbuncles, impetigo, and
scalded-skin syndrome) as well as
abscesses, sepsis, osteomyelitis,
pneumonia, endocarditis, food poisoning,
and toxic shock syndrome (TSS)
Staphylococcal Infections
S. epidermidis, a species that is related to
S. aureus, causes opportunistic infections
in catheterized patients, patients with
prosthetic cardiac valves, and drug
addicts. S. saprophyticus is a common
cause of urinary tract infections in young
women.
Staphylococcal Infections
S. aureus possess a multitude of virulence
factors, which include surface proteins
involved in adherence, secreted enzymes
that degrade proteins, and secreted toxins
that damage host cells
Staphylococcal Infections
A furuncle, or boil, is a focal suppurative
inflammation of the skin and subcutaneous
tissue, either solitary or multiple or
recurrent in successive crops.
Furuncles are most frequent in moist, hairy
areas, such as the face, axillae, groin,
legs, and submammary folds.
Staphylococcal Infections
Beginning in a single hair follicle, a boil
develops into a growing and deepening
abscess that eventually "comes to a head"
by thinning and rupturing the overlying
skin.
Staphylococcal Infections
A carbuncle is a deeper suppurative
infection that spreads laterally beneath the
deep subcutaneous fascia and then
burrows superficially to erupt in multiple
adjacent skin sinuses.
Carbuncles typically appear beneath the
skin of the upper back and posterior neck,
where fascial planes favor their spread.
Staphylococcal Infections
Hidradenitis is a chronic suppurative
infection of apocrine glands, most often in
the axilla.
Infections of the nail bed (paronychia) or
on the palmar side of the fingertips
(felons) are exquisitely painful.
They may follow trauma or embedded
splinters and, if deep enough, destroy the
bone of the terminal phalanx or detach the
fingernail.
S. aureus lung infections usually occur in
people with a hematogenous source, such
as an infected thrombus, or a predisposing
condition such as influenza.
Staphylococcal scalded-skin
syndrome, also called Ritter disease,
most frequently occurs in children with
staphylococcal infections of the
nasopharynx or skin.
There is a sunburn-like rash that spreads
over the entire body and evolves into
fragile bullae that lead to partial or total
skin loss.
The desquamation of the epidermis in
staphylococcal scalded-skin syndrome
occurs at the level of the granulosa layer,
distinguishing it from toxic epidermal
necrolysis, or Lyell's disease, which is
secondary to drug hypersensitivity and
causes desquamation at the level of the
epidermal-dermal junction.
Streptococcal Infections
Streptococci are gram-positive cocci that
grow in pairs or chains and cause a
myriad of suppurative infections of the
skin, oropharynx, lungs, and heart valves..
S. pyogenes (group A) causes pharyngitis,
scarlet fever, erysipelas, impetigo,
rheumatic fever, TSS, and
glomerulonephritis
S. agalactiae (group B) colonizes the
female genital tract and causes sepsis and
meningitis in neonates and
chorioamnionitis in pregnancy.
S. pneumoniae, the most important αhemolytic streptococcus, is a common
cause of community-acquired pneumonia
and meningitis in adults.
The viridans group streptococci include
several species of α-hemolytic and
nonhemolytic streptococci that are
normal oral flora and are also a
common cause of endocarditis.
S. mutans is the major cause of dental
caries.
Streptococcal infections are diagnosed
by culture, and the rapid antigen test for
pharyngitis.
Streptococcal infections are characterized
by diffuse interstitial neutrophilic infiltrates
with minimal destruction of host tissues.
The skin lesions caused by streptococci
(furuncles, carbuncles, and impetigo)
resemble those of staphylococci .
Erysipelas is most common among
middle-aged persons in warm climates
and is caused by exotoxins from
superficial infection with S. pyogenes.
It is characterized by rapidly spreading
erythematous cutaneous swelling that may
begin on the face or, less frequently, on
the body or an extremity. The rash has a
sharp, well-demarcated, serpiginous
border and may form a "butterfly"
distribution on the face
On histologic examination there is a
diffuse, edematous, neutrophilic
inflammatory reaction in the dermis and
epidermis extending into the
subcutaneous tissues. Microabscesses
may be formed, but tissue necrosis is
usually minor.
Streptococcal pharyngitis, which is the
major antecedent of poststreptococcal
glomerulonephritis is marked by edema,
epiglottic swelling, and punctate
abscesses of the tonsillar crypts,
sometimes accompanied by cervical
lymphadenopathy. Swelling associated
with severe pharyngeal infection may
encroach on the airways, especially if
there is peritonsillar or retropharyngeal
Scarlet fever, associated with pharyngitis caused by S.
pyogenes, is most common between the ages of 3 and
15 years. It is manifested by a punctate erythematous
rash that is most prominent over the trunk and inner
aspects of the arms and legs. The face is also involved,
but usually a small area about the mouth remains
relatively unaffected to produce a circumoral pallor. The
inflammation of the skin usually leads to hyperkeratosis
and scaling during defervescence.
S. pneumoniae is an important cause of
lobar pneumonia
Enterococcal Infections
Enterococci are also gram-positive cocci
that grow in chains. Enterococci are often
resistant to commonly used antibiotics and
are a significant cause of endocarditis and
urinary tract infections.
Enterococci are also gram-positive cocci
that grow in chains. Enterococci are often
resistant to commonly used antibiotics and
are a significant cause of endocarditis and
urinary tract infections
Diphtheria
Diphtheria is caused by Corynebacterium
diphtheriae, a slender gram-positive rod
with clubbed ends, that is passed from
person to person through aerosols or skin
exudate.
C. diphtheriae may be carried
asymptomatically or cause illnesses
ranging from skin lesions in neglected
wounds of combat troops in the tropics,
and a life-threatening syndrome that
includes formation of a tough pharyngeal
membrane and toxin-mediated damage to
the heart, nerves, and other organs
Listeriosis
Listeria monocytogenes is a gram-positive,
facultative intracellular bacillus that causes
severe food-borne infections
In acute human infections, L.
monocytogenes evokes an exudative
pattern of inflamma-tion with numerous
neutrophils.
The meningitis it causes is
macroscopically and microscopically
indistinguishable from that caused by
other pyogenic bacteria
The finding of gram-positive, mostly
intracellular, bacilli in the CSF is virtually
diagnostic.
More varied lesions may be encountered
in neonates and immunosuppressed
adults.
Focal abscesses alternate with grayish or
yellow nodules representing necrotic
amorphous basophilic tissue debris.
These can occur in any organ, including
the lung, liver, spleen, and lymph nodes. In
infections of longer duration, macrophages
appear in large numbers, but granulomas
are rare
Infants born with L. monocytogenes
sepsis often have a papular red rash over
the extremities, and listerial abscesses
can be seen in the placenta. A smear of
the meconium will disclose the grampositive organisms.
Anthrax
Bacillus anthracis is a large, spore-forming
gram-positive rod-shaped bacterium.
These bacteria are common pathogens in
farm and wild animals that have contact
with soil contaminated with B. anthracis
spores. Anthrax spores can be ground to a
fine powder, making a potent biologic
weapon.
B. anthracis is typically acquired through
exposure to animals or animal products
such as wool or hides.
There are three major anthrax syndromes.
Cutaneous anthrax, which makes up 95% of
naturally occurring infections, begins as a
painless, pruritic papule that develops into a
vesicle within 2 days. As the vesicle enlarges,
striking edema may form around it, and regional
lymphadenopathy develops. After the vesicle
ruptures, the remaining ulcer becomes covered
with a characteristic black eschar, which dries
and falls off as the person recovers. Bacteremia
is rare with cutaneous anthrax.
Inhalational anthrax occurs when spores are inhaled.
The organism is carried by phagocytes to lymph nodes
where the spores germinate, and the release of toxins
causes hemorrhagic mediastinitis. After a prodromal
illness of 1 to 6 days characterized by fever, cough, and
chest or abdominal pain, there is abrupt onset of
increased fever, hypoxia, and sweating. Frequently,
anthrax meningitis develops from bacteremia.
Inhalational anthrax rapidly leads to shock and frequently
death within 1 to 2 days.
Gastrointestinal anthrax is an uncommon
form of this infection that is usually
contracted by eating undercooked meat
contaminated with B. anthracis. Initially,
the person has nausea, abdominal pain,
and vomiting, followed by severe, bloody
diarrhea. Mortality is over 50%.
Anthrax lesions at any site are typified by
necrosis and exudative inflammation with
infiltration of neutrophils and
macrophages.
The presence of large, boxcar-shaped grampositive extracellular bacteria in chains,
seen histopathologically or recovered in
culture, should suggest the diagnosis.
Inhalational anthrax causes numerous foci of
hemorrhage in the mediastinum with hemorrhagic,
enlarged hilar and peribronchial lymph nodes.
Microscopic examination of the lungs typically shows a
perihilar interstitial pneumonia with infiltration of
macrophages and neutrophils and pulmonary vasculitis.
Hemorrhagic lesions associated with vasculitis are also
present in about half of cases. Mediastinal lymph nodes
show lymphocytosis, macrophages with phagocytosed
apoptotic lymphocytes, and a fibrin-rich edema
B. anthracis is present predominantly in
the alveolar capillaries and venules and, to
a lesser degree, within the alveolar space.
In fatal cases, B. anthracis is evident in
multiple organs (spleen, liver, intestines,
kidneys, adrenal glands, and meninges).
GRAM-NEGATIVE BACTERIAL
INFECTIONS
Neisserial Infections
Neisseria are gram-negative diplococci that are
flattened on the adjoining sides, giving the pair
the shape of a coffee bean
These aerobic bacteria have stringent nutritional
requirements and grow best on enriched media
such as lysed sheep's blood agar ("chocolate"
agar).
The two clinically significant Neisseria are N.
meningitidis and N. gonorrhoeae.
N. meningitidis is a significant cause of bacterial
meningitis, particularly among children younger
than 2 years of age.
The organism is a common colonizer of the
oropharynx and is spread by the respiratory
route.
Approximately 10% of the population is
colonized at any one time, and each episode of
colonization lasts, on average, for several
months.
N. gonorrhoeae is an important cause of sexually
transmitted disease (STD)
It is second only to C. trachomatis as a bacterial
causative agent of STDs.
Infection in men causes urethritis. In women, N.
gonorrhoeae infection is often asymptomatic and so may
go unnoticed. Untreated infection can lead to pelvic
inflammatory disease, which can cause infertility or
ectopic pregnancy
Infection is diagnosed by PCR tests, in addition to
culture.
Whooping Cough
Whooping cough, caused by the gram-negative
coccobacillus Bordetella pertussis, characterized
by paroxysms of violent coughing followed by a
loud inspiratory "whoop."
B. pertussis vaccination, whether with killed
bacteria or the newer acellular vaccine, has
been effective in preventing whooping cough.
The diagnosis is best made by PCR, because
culture is less sensitive.
Bordetella bacteria cause a
laryngotracheobronchitis that in severe cases
features bronchial mucosal erosion, hyperemia,
and copious mucopurulent exudate
Unless superinfected, the lung alveoli remain
open and intact. In parallel with a striking
peripheral lymphocytosis (up to 90%), there is
hypercellularity and enlargement of the mucosal
lymph follicles and peribronchial lymph nodes.
Pseudomonas Infection
Pseudomonas aeruginosa is an
opportunistic aerobic gram-negative
bacillus that is a frequent, deadly
pathogen of people with cystic fibrosis,
severe burns, or neutropenia.93 Many
people with cystic fibrosis die of pulmonary
failure secondary to chronic infection with
P. aeruginosa. P. aeruginosa can be very
resistant to antibiotics, making these
infections difficult to treat. P. aeruginosa
Pseudomonas causes a necrotizing
pneumonia that is distributed through the
terminal airways in a fleur-de-lis pattern, with
striking pale necrotic centers and red,
hemorrhagic peripheral areas.
On microscopic examination, masses of
organisms cloud the tissue with a bluish haze,
concentrating in the walls of blood vessels,
where host cells undergo coagulative
necrosis
This picture of gram-negative vasculitis
accompanied by thrombosis and
hemorrhage, although not pathognomonic,
is highly suggestive of P. aeruginosa
infection.
In skin burns, P. aeruginosa proliferates
penetrating deeply into the veins and spreading
hematogenously.
Well-demarcated necrotic and hemorrhagic oval
skin lesions, called ecthyma gangrenosum
Disseminated intravascular coagulation (DIC) is
a frequent complication of bacteremia.
Plague
Yersinia pestis is a gram-negative
facultative intracellular bacterium that is
transmitted from rodents to humans by
fleabites or, less often, from one human to
another by aerosols
Yersinia pestis causes lymph node
enlargement (buboes), pneumonia, or
sepsis with a striking neutrophilia.
The distinctive histologic features
(1) massive proliferation of the organisms,
(2) early appearance of protein-rich and polysacchariderich effusions with few inflammatory cells but with
marked tissue swelling,
(3) necrosis of tissues and blood vessels with
hemorrhage and thrombosis,
(4) neutrophilic infiltrates that accumulate adjacent to
necrotic areas as healing begins.
In bubonic plague the infected fleabite is
usually on the legs and is marked by a small
pustule or ulcer. The draining lymph nodes
enlarge dramatically within a few days and
become soft, pulpy, and plum colored, and may
infarct or rupture through the skin
In pneumonic plague there is a severe,
confluent, hemorrhagic and necrotizing
bronchopneumonia, often with fibrinous pleuritis.
In septicemic plague lymph nodes throughout
the body as well as organs rich in mononuclear
phagocytes develop foci of necrosis.
Fulminant bacteremias also induce DIC with
widespread hemorrhages and thrombi.
Chancroid (Soft Chancre)
Chancroid is an acute, sexually
transmitted, ulcerative infection caused by
Hemophilus ducreyi.
The disease is most common in tropical
and subtropical areas among lower
socioeconomic groups and men who have
regular contact with prostitutes. Chancroid
is one of the most common causes of
genital ulcers in
Four to seven days after inoculation the person
develops a tender, erythematous papule
involving the external genitalia. In males the
primary lesion is usually on the penis; in females
most lesions occur in the vagina or the
periurethral area.
Over the course of several days the surface of
the primary lesion erodes to produce an irregular
ulcer, which is more apt to be painful in males
than in females
In contrast to the primary chancre of syphilis, the ulcer
of chancroid is not indurated, and multiple lesions may
be present. The base of the ulcer is covered by shaggy,
yellow-gray exudate.
The regional lymph nodes, particularly in the inguinal
region, become enlarged and tender in about 50% of
cases within 1 to 2 weeks of the primary inoculation. In
untreated cases the inflamed and enlarged nodes
(buboes) may erode the overlying skin to produce
chronic, draining ulcers
Microscopically, the ulcer of chancroid contains a
superficial zone of neutrophilic debris and fibrin, with an
underlying zone of granulation tissue containing areas of
necrosis and thrombosed vessels. A dense,
lymphoplasmacytic inflammatory infiltrate is present
beneath the layer of granulation tissue. Coccobacilli are
sometimes demonstrable in Gram or silver stains, but
they are often obscured by other bacteria that colonize
the ulcer base.
Granuloma Inguinale
Granuloma inguinale, or donovanosis, is a
chronic inflammatory disease caused by
Klebsiella granulomatis (formerly called
Calymmatobacterium donovani), a minute,
encapsulated, coccobacillus.
The organism is sexually transmitted
Granuloma inguinale begins as a raised, papular lesion
on the moist, stratified squamous epithelium of the
genitalia or, rarely, the oral mucosa or pharynx.
The lesion eventually ulcerates and develops abundant
granulation tissue, which is manifested grossly as a
protuberant, soft, painless mass.
As the lesion enlarges, its borders become raised and
indurated.
Disfiguring scars may develop in untreated cases and
are sometimes associated with urethral, vulvar, or anal
strictures.
Regional lymph nodes typically are spared
or show only nonspecific reactive
changes, in contrast to chancroid.
Microscopic examination of active lesions reveals
marked epithelial hyperplasia at the borders of the ulcer,
sometimes mimicking carcinoma
(pseudoepitheliomatous hyperplasia). A mixture of
neutrophils and mononuclear inflammatory cells is
present at the base of the ulcer and beneath the
surrounding epithelium. The organisms are
demonstrable in Giemsa-stained smears of the exudate
as minute, encapsulated coccobacilli (Donovan bodies)
in macrophages. Silver stains (e.g., the Warthin-Starry
stain) may also be used to demonstrate the organism.
CHLAMYDIAL DISEASES
Chlamydiae are obligate intracellular organisms,
larger than viruses.
The host response is neutrophilic.
Chlamydiae are passively taken up into
phagocytic vacuoles of host cells in which they
multiply; they are best visualized by
immunofluorescence or Giemsa-stained cell
smears.
Cytoplasmic chlamydial inclusions, important in
microscopic diagnosis, consist of aggregates of
these bodies in their vacuoles.
C. trachomatis
– the most common cause of sexually
transmitted diseases, in men:
nongonococcal urethritis and epididymitis;
– in women: cervicitis, urethritis, and pelvic
inflammatory
– Reiter's syndrome;
– neonatal conjunctivitis and pneumonia
acquired through maternal transmission.
– C. trachomatis has been implicated in 20%
of adults with pharyngitis.
C. psittaci
– infects many animals,
– but human infection is closely related to contact
with birds.
C. pneumoniae
– a serotype of C. psittaci,
– can cause pneumonia, especially in children and
young adults.
– It may be clinically indistinguishable from
pneumonia caused by Mycoplasma pneumoniae.
– The organism has been found in atheromatous
lesions, and infection is associated with increased
risk of coronary artery disease.
Chlamydial infection
Tissue response
Inclusion body
conjunctivitis
Acute
Ornithosis
Acute
Trachoma
Chronic, including
granulomas
Veneral disease
Chronic, including
granulomas
Ornithosis (Psittacosis, parrot fever)
Ornithosis is caused by Chlamydia psittaci,
transmitted to man by inhalation of dusts
containing infected-bird excreta.
Most any kind of bird can do it; the classic is
parrots.
Inhalation of the agent may lead to an
asymptomatic infection (a flu like illness), or a
serious, even fatal neutrophilic pneumonia.
In severe cases there is edema, alveolar
damage, consodalition, and bacterial
superinfection.
Histologically, there is edema and mononuclear
leukocytic infiltration within the alveolar septa.
Seroproteinaceous fluid or fibrin may accumulate within
the alveoli.
Alveolar septal cells may contain intracytoplasmic
chlamydial inclusions (Giemsa or immunofluorescence
stain shows inclusion bodies in the cytoplasm).
Lethal generalized disease is marked by focal necrosis
in the liver and spleen and by diffuse mononuclear
leukocytic infiltration in the kidneys, heart, and brain.
Recovery is the rule after a few weeks. The infection
may remain latent, and may recur.
Trachoma
Trachoma is a chronic suppurative eye disease
follicular keratoconjunctivitis caused by
Chlamydia trachomatis .
A disease of the poor nations, and the world's
most important cause of preventable blindness.
Infection of the surface of the eye with an
aggressive strain (A-C) of Chlamydia
trachomatis, a micro-organism which flourishes
in arid and sandy countries
Chlamydia reaches the eyes by means of fingers, contaminated
particles, or flies.
The resulting inflammation produces proliferation of the conjunctival
surface tissue. Infection can be either self-limiting or progressive.
In a progressive infection, there is a suppuration with
lymphoplasmacytic infiltration and formation of lymphoid cell
follicles.
Lymphoid follicles and epithelial hyperplasia help establish the
diagnosis.
Soon, the conjunctiva ulcerates, and penetration into the cornea
leads to pannus (inflammatory membrane) formation with scarring
granulation tissue.
With enough scarring, the eyelids fail to close properly.
Many of these people are also vitamin A deficient. With no access to antibiotics (or any medical
care) blindness will result.
Inclusion conjunctivitis
Inclusion conjunctivitis is a benign, self-limited,
suppurative conjunctivitis that occurs in babies of
mothers having Chlamydia trachomatis birth canal
infection.
Or caught from people with genital chlamydia (fingers,
un-halogenated swimming pools). The latter produces
"swimming pool conjunctivitis".
It is characterized by conjunctival hyperemia, edema and
monocyte-rich purulent exudate infiltration.
The pannus and corneal scarring seen in trachoma do
not occur.
Lymphogranuloma venereum (LGV)
Infection of the anogenital region with aggressive Chlamydia
trachomatis (serotypes L-1, -2, or -3).
Fortunately rare, this disease is encountered primarily in the tropics;
non-tropical cases have mostly been in gay men.
Stages of the disease:
Stage I. The disease begins with a small vesicle that promptly bursts
and ulcerates with abundant neutrophilic exudation at the site of
inoculation (genital, labial, anorectal, buccopharyngeal, digital).
Later, granulomas may form at the ulcer base, and clamydial
inclusions can be seen by specific immunofluorescence technique.
Stage II. It spreads to the axillary or inguinal lymph nodes,
which suppurate (buboes; there is a granulomatous
admixture; stellate microabscesses rimmed by
granulomas are typical). In heterosexual males, inguinal
lymphadenopathy is rule; in females, spread is to the
deep pelvic and perirectal lymph nodes. The disease
does not become systemic.
Stage III. The end stage is rectal strictures and/or
elephantiasis due to dense fibrosis, and chronic
inflammatory infiltration with abundant plasma cells.
Chlamydial urethritis and cervicitis
Very common sexually transmitted diseases, usually caused by less
virulent strains of Chlamydia trachomatis than cause LGV. This
organism is our most important cause of nongonococcal urethritis
and nongonococcal cervicitis.
This is an important cause of fallopian tube infections ("pelvic
inflammatory disease"), and it can be transmitted to the baby
during birth.
Look for DNA probes as the future's preferred way of making the
diagnosis of chlamydial genital infections. Rapid enzyme
immunoassay to screen a man's urine to see if he has chlamydia on
board.
Chlamydia pneumoniae is an important cause of wheezy
adult lung infections and very likely a major player in much chronic
asthma.
RICKETTSIAL DISEASES
- Rickettsiae are obligate intracellular bacteria that cannot
grow except within cells.
- They are inhabit ticks, mites fleas or lice.
- Infection is contracted either by an arthropod bite or by
contact of arthropod excreta with abraded skin.
- Rickettsiae never part of the "normal flora", and always
indicate disease.
Typhus fever (epidemic typhus)
A dread disease caused by Rickettsia prowazekii, transmitted by
louse feces. Epidemics occur during wartime, famine, and natural
disaster.
Death is not uncommon in untreated cases. It results from brain,
heart, and lung involvement.
Patients have generalized skin rash, headache, fever, mental
changes, and even gangrene (from vasculitis).
The essential pathology is swelling and necrosis of the endothelial
cells in many parts of the body.
Endothelial proliferation and swelling in the capillaries, arterioles,
and venules may narrow the lumina of these vessels.
In milder cases, the macroscopic changes are limited to the skin
rash and small hemorrhages.
In severe cases there may be areas of necrosis of the skin with
gangrene of the tips of fingers, nose, ear lobes, scrotum, penis, and
vulva.
In such cases, irregular ecchymotic hemorrhages may be found
internally, principally in the brain, heart muscle, testes, serosal
membrane, lung, and kidneys.
In the brain of untreated patients, reactive glia mixed with
inflammatory cells produce characteristic typhus nodules.
Mononuclear cell meningitis, and ring hemorrhages about the small
vessels may occur.
Typically, there is also nonspesific lymphadenitis and splenitis.
Foci resembling the typhus nodules of the brain may appear in the
heart, kidney, testes, and liver.
Rocky Mountain spotted fever of Americans is caused
by Rickettsia rickettsi. It is a tick-borne rickettsia which
invades both endothelial and vascular smooth muscle
cells. Hemorrhages (spots) from necrosis of the skin
arterioles are present everywhere, including on the
palms and soles, also the scrotum/vulva.
Patients are systemically sick, and the vasculitis and
hemostatic chaos can be fatal if untreated.
Scrub typhus (tsutsugamushi fever) is caused by
Orientia tsutsugamushi, carried by a mite, endemic
throughout the Far East and Pacific rim.
Q-fever is a pneumonitis caused by
Coxiella burnetti. The "Q" comes from
Queensland, Australia, but this infection is
found worldwide.
The disease is common among sheep, and
can be transmitted by ticks or by droplets.
Coxiella can tolerate drying, unlike the
other rickettsia.
Bacillary angiomatosis
is an opportunistic infections (AIDS
patients) caused by either Bartonella
henselae (the cat-scratch fever organism)
or Bartonella (Rochalimaea) quintana (the
trench fever organism).
Dilated vessels in the liver, spleen, and
elsewhere are typical. Bacteria can
accumulate in masses dense enough to
appear as granular hyaline. The disease
responds to antibiotics.
MYCOPLASMAL DISEASES
Mycoplasmas are also called pleuropneumonia-like organisms
(PPLO's) or Eaton agent. They are little (0.3-0.8 ) bacteria
without cell walls.
Mycoplasma genitalium and Ureaplasma urealyticum are
causes purulent, acute, nongonococcal urethritis as well as
chronic pelvic inflammatory disease.
Mycoplasma pneumoniae is probably the commonest cause
of a chest cold (primary atypical pneumonia), generally with an
upper respiratory infection. It behaves as an extracellular
human parasite, and incites epithelial damage in the airways.
The pulmonary involvement mimics to viral pneumonia. The
epidemics are mostly seen in closed institutions (e.g., military
recruits, prisons). Death is rare.
ACTINOMYCETES
Nocardiosis
Actinomycosis
NOCARDIOSIS
Infection with "Nocardia", a lowvirulence, filamentous, gram-positive,
weakly acid-fast bacterium
An acute or chronic, often disseminated,
granulomatous-suppurative infectious
disease usually caused by the aerobic
gram-positive bacillus Nocardia
asteroides, a soil saprophyte.
N. asteroides usually enters the body
via the lungs and rarely via the GI tract
or skin.
Immunosuppressed patients develop lung infections with
Nocardia asteroides. Nocardia typically cause single or
multipl, chronic, necrotizing, walled-off abscesses
without granuloma formation.
Predisposing factors:
–
–
–
–
–
–
–
Lymphoreticular malignancies,
organ transplantation,
high-dose corticosteroid
immunosuppressive therapy,
HIV,
underlying pulmonary disease.
About half the patients have no preexisting disease.
Primary skin lesions are necrotizing or
purulent, or both.
"Immunologically normal" people can
develop Nocardia brasiliensis skin
infections ("mycetomas", a generic name
for hard-to-treat, nodular "fungal" skin
infections, especially common on the feet
in countries where shoes are a luxury).
– The problem is common in Latin America.
An acute or chronic, often disseminated,
granulomatous-suppurative infectious
disease usually caused by the aerobic
gram-positive bacillus Nocardia
asteroides, a soil saprophyte.
N. asteroides usually enters the body via
the lungs and rarely via the GI tract or
skin.
Disseminated nocardiosis usually
begins as a pulmonary infection that
may resemble actinomycosis,
N. asteroides is more likely to
disseminate hematogenously with
abscess formation in the brain, kidneys
or in multiple organs.
Skin or subcutaneous abscesses occur
frequently, sometimes as a primary site
of localized infection.
Lung lesions are nonspecific and
resemble those of TB or suppurative
pneumonia.
Pleural effusion also may occur.
Metastatic brain abscesses may occur
in as many as 1/3 of cases.
Nocardia asteroides
ACTINOMYCOSIS
Chronic fibrosing, pus-producing infections
with multiple draining sinuses due to an
anaerobic "Actinomyces" bacterium,
usually Actinomyces israelii.
The causative anaerobic, gram-positive
microorganisms, species of Actinomyces
or Propionobacterium (most commonly A.
israelii), are often present comensally on
the gums, tonsils, and teeth.
The characteristic lesion is an indurated
area of multiple, small, communicating
abscesses surrounded by granulation
tissue.
Tissue lesions tend to form sinus tracts
that communicate to the skin and drain
a purulent discharge containing yellow
sulfur granules.
The classic form is cervicofacial actinomycosis, with
running sores in the mouth, and on the face and neck.
At first the gingivae and adjacent soft tissues become
swollen and indurated.
In course of time, a large, woody swelling
develops,characteristically over the angle of the jaw.
The inflammation often extends to the skin to perforate
and form multiple sinuses.
Periostitis and osteomyelitis with extensive destruction of
bone are common accompaniments.
In the cervicofacial (lumpy jaw) form, the
most common portal of entry is decayed teeth
– The cheek, tongue, pharynx, salivary glands,
cranial bones, meninges, or brain may be affected,
usually by direct extension.
Lung abscesses (thoracic actinomycosis)
– pulmonary disease results from aspiration of oral
secretions.
The peritoneal cavity may become involved
after rupture of the gut (abdominal
actinomycosis)
– a break in the mucosa of a diverticulum, the
appendix, or during trauma.
In a localized pelvic form, actinomycosis is a
complication of certain types of intrauterine
device (IUD) contraceptives.
Abdominal actinomycosis arises from invasion
of the intestinal mucosa, most commonly of the
appendix or colon.
– Bowel lesions produce localized peritoneal abscess,
sometimes with the formation of draining external
sinuses.
Thoracic actinomycosis: lung abscesses may
cause pulmonopleural fistulas, and empyeme.
– Further spread may erode the ribs and the anterior
chest wall or extends into the vertebral column and
pericardium.
Smears of actinomycosis pus show naked-eye
"sulfur granules" (large yellow actinomyces
colonies).
The histologic features:
– central suppuration surrounded by granulation tissue
– intense fibrosis
– bacterial colony consisting of intertwined radiating
flaments (rays), capped by eosinophilic material
(sunburst pattern).
Spread from primary sites occurs rarely, presumably by
hematogenous spread from primary sites of infection
In the generalized form, infection spreads
hematogenously to the skin, vertebral bodies, brain,
liver, kidney, ureter, and (in women) pelvic organs.
Actinomycosis of other sites follows bites or punch
injuries.
Pelvic actinomycosis was a complication of the oldfashioned intra-uterine devices.
The radially-oriented bacteria at their edges earned the
actinomyces the unfortunate name "ray fungi".
Actinomyces israelii