Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hormone replacement therapy (female-to-male) wikipedia , lookup
Growth hormone therapy wikipedia , lookup
Metabolic syndrome wikipedia , lookup
Polycystic ovary syndrome wikipedia , lookup
Hypothalamic–pituitary–adrenal axis wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Hypothalamus wikipedia , lookup
Androgen insensitivity syndrome wikipedia , lookup
Pituitary apoplexy wikipedia , lookup
Hypopituitarism wikipedia , lookup
Congenital adrenal hyperplasia due to 21-hydroxylase deficiency wikipedia , lookup
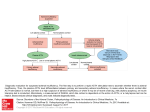
The Adrenal Cortex Basic principles of steroid endocrinology • Steroid effects fall into 3 categories: – Mineralocorticoid – Glucocorticoid – Androgen/Estrogen • Small differences in steroid molecules have large effects on activity • Steroids act through nuclear receptors, so their major effects involve changes in the expression of particular genes Major Corticosteroid Hormones • Aldosterone – mineralocorticoid • Cortisol (human); corticosterone (some mammals) – glucocorticoid • Adrenal androgens: dehydroepiandrosterone (DHEA), androstenedione, androstenediol, Corticosteroid effects Hormone Actions/Effects Aldosterone Stimulates Na+ reabsorption and H+ and K+ secretion in nephron; indirectly regulates ECF volume Cortisol Permissive for epi and glucagon Stimulates lipolysis, protein catabolism and gluconeogenesis Essential for normal inflammatory and immune responses; but immunosuppressive and antiinflammatory at pharmacological doses; also stimulates bone breakdown Androgens Masculinizing effect at high doses, especially during prenatal development; postnatal effects probably trivial for males but essential for sustaining sex interest in females Pathways of adrenal steroid biosynthesis Important points: This reaction occurs in the periphery, not in the adrenal itself multiple reactions are catalyzed by the same enzymes – however, in different regions of the cortex, different parts of the map are favored. Enzyme mutations are responsible for a number of clinical syndromes: for example – 21 alpha hydroxylase deficiency • Leads to inadequate production of both mineralocorticoid and glucocorticoid, but excessive production of adrenal androgen • Symptoms: salt-losing diuresis, increased susceptibility to infection, premature masculinizing puberty • Adrenal hypertrophy occurs as a result of the lack of feedback from cortisol – so ACTH levels are elevated. • Appropriate therapy: replacement cortisol Control of ACTH secretion • The hypothalamus releases CRH in regular pulses, about every 20 min. • Circadian rhythm: greatest secretion (increased pulse amplitude) occurs in the early morning before awakening • Stress or hypoglycemia strongly stimulate pulse amplitude. • ADH also stimulates ACTH secretion. What is stress, anyway? • • • • • • • Emotional Situational Surgical Forced exercise Confinement/handling (animals) Pain Ultimately, physiologists have decided to define stress as any stimulus that elevates ACTH secretion. Hyper and hypoadrenal syndromes • Cushing’s Syndrome: excessive corticosteroid – hypertension, hyperglycemia, hypokalemia, alkalosis, characteristic pattern of fat loss from lower body and fat deposition around neck and face. This syndrome is very commonly iatrogenic. • Addison’s Syndrome: hypotension, poor survival in fasting, increased susceptibility to infection, hyperkalemia, acidosis, potential for ‘Addisonian crisis’. • Causes may be at level of hypothalamus, pituitary or adrenal itself – diagnosis involves measurement of ACTH levels Post-translational processing of POMC in pituitary corticotrophs ‘POMC’ is proopiomelanocortin. The primary gene product can be clipped at different places to produce a variety of hormones. During adult life, the major corticotroph products are ACTH and betalipotropin. During fetal life and in pregnant women, the pars intermedia of the pituitary processes the gene product differently, yielding gamma lipotropin, beta endorphin, and two versions of melanocyte stimulating hormone. Addison’s Syndrome hypoadrenalism • • • • • • Hypoglycemia Hypotension Poor resistance to infection Fatigue, muscle weakness Susceptibility to Addisonian crises Hyperpigmentation – in primary hypoadrenalism Primary versus secondary disease • In primary hypoadrenalism, the adrenal cortex is the site of the lesion and ACTH levels are elevated, giving hyperpigmentation. • In secondary hypoadrenalism, the pituitary or brain is the site of the lesion, and ACTH levels are low. Visible symptoms of Cushing’s syndrome Symptoms of Hyperadrenalism • Obesity – including characteristic fat deposit on back of neck • Skin changes • Symptoms of androgen excess • Muscle and bone loss • Menstrual irregularity • Hypertension • Glucose intolerance